
Abstract
Aim:
The main objectives of this study were to investigate the relationship between prolonged QRS interval and its prognosis in patients with dilated cardiomyopathy (DCM), and to determine the effects of cardiac pacing with an implantable cardioverter-defibrillator (ICD) on mortality in patients with a QRS width > 150 ms.
Methods:
We retrospectively queried the healthcare enterprise data warehouse and the patient medical records from January 2007 to December 2012 for 1453 cases of DCM at a university- affiliated hospital. Of the 1453 cases, 989 patients were included in the final analyses. Primary outcome variable was all-cause mortality.
Results:
Of the 989 patients, 20% (n = 198) of the patients had a QRS width > 150 ms. Compared with patients who had a QRS < 120 ms, patients with a QRS > 150 ms had significantly higher rates of death (p < 0.001). Among the subgroup of 198 patients who had a QRS width > 150 ms, survival (84.3%, n = 75) was significantly higher (p < 0.001) in patients with a pacemaker inserted compared with those (45.0%, n = 49) who had not been paced.
Conclusions:
Prolonged QRS interval is significantly associated with a higher rate of mortality. However, we believe that cardiac pacing with an ICD in such patients can significantly improve outcomes.
Introduction
With an annual incidence of approximately 36 per 100,000 cases, dilated cardiomyopathy (DCM) is a common cause of heart failure in the USA [Olbrich, 2001]. Patients with DCM can present with severe arrhythmias, and in such cases, use of cardiac pacing with an implantable cardioverter-defibrillator (ICD) improves survival by treating life-threatening ventricular arrhythmias. QRS-interval prolongation is mainly representative of intraventricular conduction delay and has been associated as a risk marker of underlying structural heart disease. QRS prolongation is also commonly seen in the general population with elderly people at the most risk [Cheng et al. 2010]. Previous literature has shown that cardiac pacing with an ICD, especially among patients with a QRS interval > 160 ms, can help lower mortality [Xiao et al. 1996; Borne et al. 2013; Schaer et al. 2006]. With this evidence, it can be suggested that prolonged QRS interval might be an important prognostic factor.
Whether QRS prolongation is simply a risk marker of heart failure and its severity, or actually a risk factor for heart-failure progression and mortality remains a subject of interest [Tabrizi et al. 2007; Barsheshet et al. 2011; Lund et al. 2013; Li et al. 2014]. Our study attempts to support the growing literature by conducting an investigation to determine the effects of biventricular pacing with an ICD, and the relationship between prolonged QRS interval and its prognosis in patients with ischemic or idiopathic DCM.
Methods
This study was conducted with approval from the institutional review board and was compliant with the Health Insurance Portability and Accountability Act. The requirement for written informed consent was waived due to the retrospective nature of our study.
Study design
We retrospectively queried the healthcare enterprise data warehouse and patient medical records from January 2007 to December 2012 for 1453 cases of echocardiography-confirmed DCM at a university-affiliated hospital. DCM was defined as an ejection fraction of lower than 45%, and/or a fractional shortening of lower than 25% in association with a left ventricular end diastolic dimension greater than 112% of predicted dimension [Thomas et al. 2009]. As coronary arteriography was not regularly performed, it is probable that our sample population will have patients with idiopathic as well as ischemic cardiomyopathy. Of the 1453 cases, 464 cases were excluded because of missing electrocardiograms and incomplete reports. The remaining 989 patients were included in our investigation. The primary outcome variable was all-cause mortality, which was checked through medical records and follow-up calls. The patients were divided into three groups based on QRS width namely: > 150 ms, 120–150 ms, and < 120 ms.
Electrocardiography
The electrocardiograms used were standard 12 lead with a calibration of 0.1 mV/mm and paper speed 25 mm/s. QRS interval, PR interval, and QT interval were calculated and printed out by built-in software.
Echocardiography
Echocardiograms had been generated using cross-sectional, image-guided M-mode echocardiograms at the level of mitral tips using 2.5-MHz phased-array transducer.
Statistical analysis
All statistical analyses were performed using SAS 9.3.1 (SAS Institute, Cary, NC, USA). Continuous variables were expressed as mean (± standard deviation) and categorical variables as frequency (percentage). The chi-square test was used to assess the differences in categorical variables while the analysis of variance was performed to compare means among the different groups. Root mean square values and coefficient of variation were used to assess reproducibility. p ≤ .05 was considered statistically significant.
Results
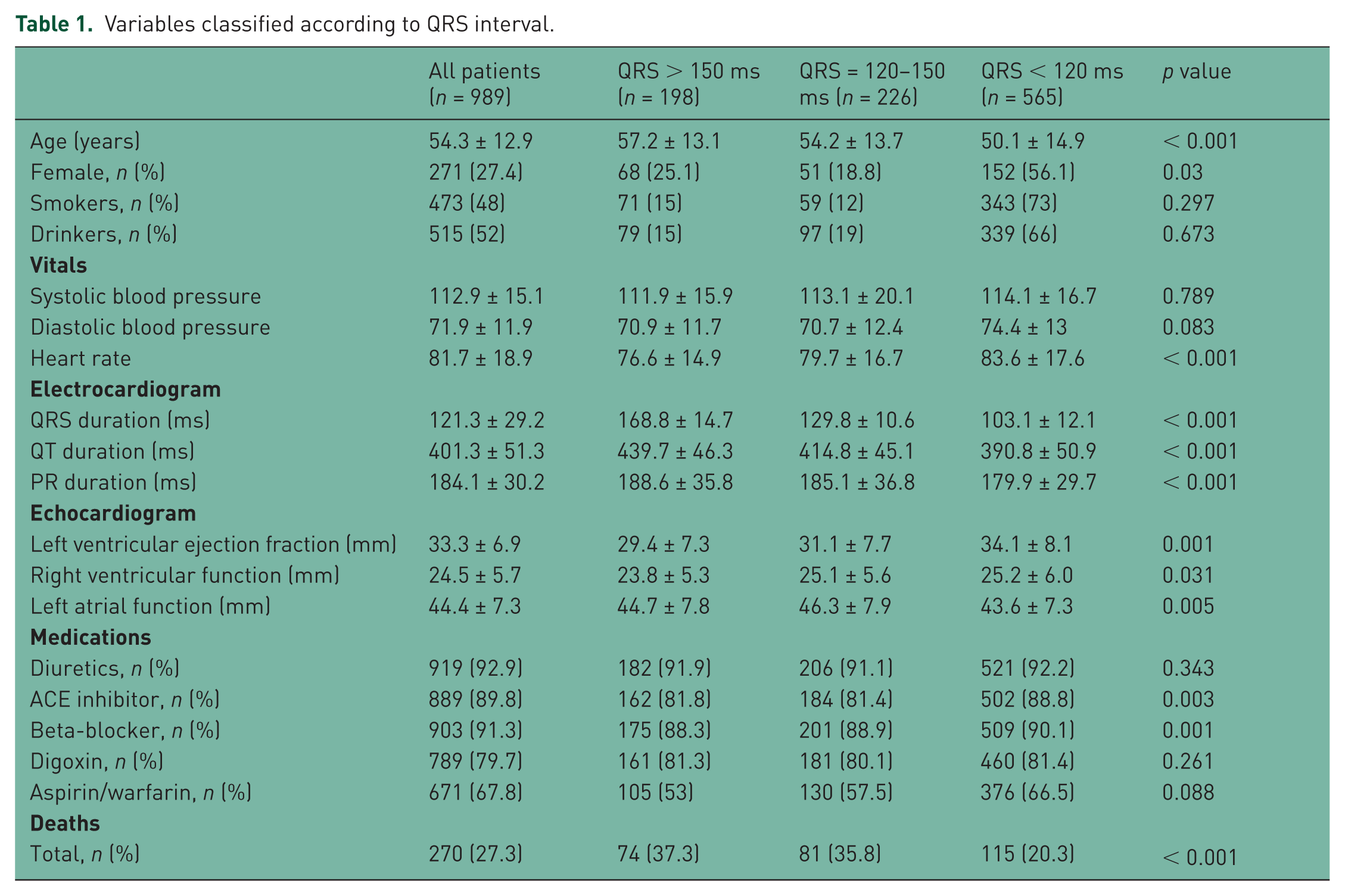
The mean age of the study subjects was 54.3 ± 12.9 years, with a male (n = 718) to female (n = 271) ratio of approximately 2.5:1. Of the 989 patients included, 20% (n = 198) of the patients had a QRS width > 150 ms. Patients with QRS interval > 150 ms were more likely to be older (p < 0.001) males (p = 0.03), and have slower heart rates (p < 0.001), lower left ventricular ejection fraction (p < 0.001), and larger left atrium diameter (p = 0.005). Moreover, patients with QRS interval > 150 ms were less likely to be using beta-blockers (p < 0.001) and angiotensin-converting enzyme (ACE) inhibitors (p = 0.003) (Table 1).
Variables classified according to QRS interval.
Overall mortality rate was 27.3 % (n = 270). Compared with patients who had a QRS < 120 ms, patients with QRS > 150 ms had significantly higher rates of death (p < 0.001). Among the subgroup of 198 patients who had a QRS width > 150 ms, 89 (44.9%) patients were paced with an ICD. Survival (84.3%, n = 75) in patients with a pacemaker was significantly higher (p < 0.001) compared with patients (45.0%, n = 49) who had not been paced (Table 2).
Effect of cardiac pacing with implantable cardioverter-defibrillators on mortality in patients with QRS width > 150 ms.

Discussion
In this study population, approximately 40% (n = 424) of the patients with DCM had a QRS width > 120 ms, which is comparable to other recent studies [Lund et al. 2013; Li et al. 2014]. QRS prolongation has been established to predict the necessity of a pacemaker [Cheng et al. 2010], and cardiovascular mortality [Desai et al. 2006], in the general population. It is important to note that incidence of QRS prolongation rises steeply with age, and is closely related with cardiac size and thus gender. QRS prolongation has also been associated with hypertension, fibrosis, and ischemic heart disease [Cheng et al. 2010]. Here we show that QRS width > 150 ms is also a significant predictor of mortality in patients with DCM. These findings echo those of Li and colleagues who reported a mortality rate of 17.2% and 33.3% in patients with a QRS < 120 ms and > 150 ms, respectively [Li et al. 2014].
We also found that cardiac pacing with an ICD has the potential to reduce significantly the rates of mortality in DCM patients. This confirms the findings of Xiao and colleagues who also reported significantly more deaths in the nonpaced group compared with the paced group [Xiao et al. 1996]. Cardiac resynchronization therapy (CRT) has recently been gaining popularity as a new therapy for patients with systolic heart failure. By reversing the harmful effects of cardiac dyssynchrony through optimization of the atrioventricular gap, CRT can improve cardiac output, mitral regurgitation, and left atrial pressure along with reducing myocardial energy consumption leading to better survival [Strickberger et al. 2005; Morani et al. 2013; Gold et al. 2013; Reitan et al. 2014]. Furthermore, a recent multicenter trial has also shown that early intervention using CRT with a defibrillator in patients with mild heart-failure symptoms and left bundle branch block can significantly increase long-term survival [Goldenberg et al. 2014].
Limitations
There are a number of limitations to our study. The study was not randomized to establish a difference in mortality between patients with and without a pacemaker. In addition, the QRS values were not measured simultaneously during patient care in an electrophysiology laboratory and were taken from medical records. Furthermore, inability on the basis of this retrospective review to define definitively every patient as having ischemic or nonischemic DCM led to the likely inclusion of both patients in the analysis, and may have biased towards a positive effect from pacing with ICD as ischemic DCM patients are known to benefit from this intervention [Wasmer et al. 2013]. In spite of these limitations, we believe our cohort has expanded the body of evidence and indicated a future direction towards large multicenter randomized trials.
Conclusion
In summary, it can be suggested that prolonged QRS interval is significantly associated with a higher rate of mortality making electrophysiological approaches an important adjunctive therapy in the management of DCM patients. We believe cardiac pacing with ICDs may have an equally important role in the future compared with currently used drugs such as beta-blockers and ACE inhibitors.
Footnotes
Acknowledgements
We would like to thank Dr Anthony Donato for revising our manuscript. Also Belty Feraro for her insight on the data collection.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
This is an institutional review board-approved retrospective study. There are no conflicts of interests or competing interests. All authors contributed equally to the work. The authors have full control over all the data.