
Abstract
The mitral valve apparatus is a complex structure consisting of several coordinating components: the annulus, two leaflets, the chordae tendineae, and the papillary muscles. Due to the intricate interplay between the mitral valve and the left ventricle, a disease of the latter may influence the normal function of the former. As a consequence, valve insufficiency may arise despite the absence of organic valve disease. This is designated as functional or secondary mitral regurgitation, and it arises from a series of distortions to the valve components. This narrative review describes the normal anatomy and the pathophysiology behind the mitral valve changes in ischemic and non-ischemic dilated cardiomyopathies. It also explains the value of a complete multiparametric assessment of this structure. Not only must an assessment include quantitative measures of regurgitation, but also various anatomical parameters from the mitral apparatus and left ventricle, since they carry prognostic value and are predictors of mitral valve repair success and durability.
Keywords
Background
Heart failure is traditionally defined as an abnormality of cardiac structure/function leading to an inadequate cardiac output or to an adequate cardiac output secondary to compensatory neurohormonal activation and increased left ventricular filling pressure. 1 With its worldwide impact, heart failure has reached the status of a global pandemic, as evidenced by estimates of 64.3 million affected individuals in 2017. 2 Whilst the etiology of heart failure displays significant geographic diversity, ischemic and non-ischemic dilated cardiomyopathies seem to be predominant etiologies of this clinical syndrome.3–5
The mitral valve stands out as particularly susceptible to alterations brought by the progression of heart failure, primarily due to its intricate nature and reliance on the coordinated function of the left ventricle (LV). 6 The pattern of insufficiency notoriously varies depending on the affected valvular component. The widely accepted Carpentier classification delineates three distinct groups of mitral regurgitation (MR) according to the valvular mechanism independent of underlying cardiomyopathy: type I (coaptation of the leaflets at the annular plane) due to annular dilatation or leaflet perforation; type II (coaptation beyond the annular plane) secondary to leaflet prolapse or papillary muscle rupture; or type III (coaptation proximal to the annular plane) associated with valvular and subvalvular sclerosis with restricted leaflet motion during diastole and systole (IIIa) or restricted leaflet motion predominantly during systole (IIIb). 7
Mitral regurgitation that arises in the absence of organic mitral valve disease, usually from LV disease, is designated as secondary (sMR) or functional, according to the most recent recommendations for MR. 8 Within the framework of the Carpentier classification system, this valvulopathy corresponds to class I or IIIb types. 6 The impact of modifications in the mitral apparatus is evidenced by the high prevalence of this disease in the presence of significant cardiomyopathy, since moderate to severe regurgitation has been reported in 60% of ischemic patients and in 40% of cases of non-ischemic disease.9,10 On the other hand, sMR itself is an independent risk factor for death and hospitalization. 11 Also of note, this disease sets in motion a cascade of effects that increase preload, wall stress, and LV workload, exacerbating the progression of heart failure. The burden of sMR-induced LV volume overload fuels a vicious cycle of LV remodeling, accentuating the severity of the regurgitation and its associated consequences. 12
The main aim of this narrative review is to describe the spectrum of alterations occurring to the mitral apparatus in the context of dilated cardiomyopathy, highlighting the differences between ischemic and non-ischemic pathological changes. Additionally, the different parameters useful for the comprehensive evaluation of this complex cardiac structure are depicted.
Normal mitral anatomy and function
The mitral valve apparatus is a complex structure that separates the left atrium (LA) posteriorly from the more anterior LV. It consists of several coordinating components: the mitral annulus, two leaflets, the chordae tendineae, and the papillary muscles. Acknowledging the basic valvular anatomy is of paramount importance in order to understand the mechanisms that culminate in sMR. 13
The mitral annulus is a D-shaped ring localized at the intersection between the LA, LV, and mitral leaflets. Bordering this structure are the left circumflex artery laterally and the coronary sinus posteriorly, which vascularize the leaflets. 13 It is non-planar and shaped like a saddle, with a dynamic movement throughout the cardiac cycle, due to its flexible parallel collagen fibers. 14 The anterior portion of the mitral annulus is continuous with the aortic annulus and constitutes the most atrial part of the saddle. 13 The posterior part of the annulus includes the lowest portion of the saddle in proximity to the lateral and medial commissures, and is not as strongly anchored to the surrounding tissues as the anterior mitral annulus. This allows a higher range of movement during myocardial contraction and relaxation. The posterior part of the annulus is also less densely fibrotic and is prone to dilation. 15 Of note, the normal mitral annulus area is around 10 cm2. Dynamics during systole are characterized by early systolic anteroposterior contraction along with LV longitudinal shortening. This results in a sphincter-like pattern that accentuates the saddle-shape prominence and contributes to preventing MR.14,16
The anterior and posterior mitral valve leaflets are separated by the anterolateral and posteromedial commissures. Both leaflets have a smooth and rough zone. The most distal part of the leaflets, close to the tips, corresponds to the rough zone and represents the coaptation surface. Normal leaflet thickness is 1–3 mm and is slightly thicker at the level of the rough zone close to its tip. 13 Because of the mitral annulus shape, the two leaflets have distinct sizes. The anterior leaflet is shaped like a sail, is attached to one-third of the mitral annulus, and is longer in length. The posterior leaflet is crescentic in shape, shorter, and attaches to the remaining two-thirds of the annulus. 17 It is scalloped and divided into three sections separated by 2 indentations that do not reach the mitral annulus in a normal mitral valve, according to Carpentier’s nomenclature: P1 lateral scallop (close to the left atrial appendage), and a larger central P2 and medial P3 scallop, anatomically related to the interatrial septum and to the cardiac right side structures. 13 The anterior leaflet is not scalloped but its segments are referred to as A1, A2, and A3, which are correspondent to P1-P2-P3. 13
The mitral valve subvalvular apparatus comprises papillary muscles and chordae tendineae. 13 The chordae tendineae are thin strands of tissue consisting of collagen and elastin fibrils surrounded by a layer of endothelium, which allows the distribution of chordal forces over the leaflet surface. 18 There are different types of chordae with several classification systems and extremely variable anatomy and branching patterns. 19 They originate from the tip of the papillary muscles and form a network near the free edges of the leaflets. 19 Primary chordae tendineae are attached to the free margins of leaflets, secondary chords connect to the ventricular surface of leaflets, and tertiary chordae arise directly from the LV wall or muscular trabeculae to the posterior leaflet. 20 Each papillary muscle distributes chordae to the ipsilateral half of both leaflets. 21 Chordae hold both leaflets in position to guarantee coaptation during systole without extrusion into the LA. 20
Normally, the LV comprises two papillary muscles one anterolateral, arising from the LV apicolateral third, and one posteromedial, arising from the middle of the LV inferior wall. 13 The anterolateral papillary muscle has a single head and has a dual blood supply from the left anterior descending and diagonal or marginal coronary branches. Left circumflex or right coronary arteries (depending on dominance) supply the two-headed posteromedial papillary muscle with often single coronary supply, which justifies its susceptibility to ischemia and rupture. 17 During the first half of systole, papillary muscles move closer together and concurrently towards the mitral annulus due to unopposed longitudinal contraction of the LV base. Because the mitral leaflets move upwards towards the LA at the same pace as the papillary muscles, the distance between the papillary muscle tips and leaflets remains constant, which avoids distortion of the mitral leaflets. 17 At the mid and late systolic period, papillary muscle bodies contract, and tips are pulled downwards, away from the annulus, which closes the leaflets, and keeps them under directed tension and posterior restrain to prevent their systolic anterior motion. 17
Mitral valve apparatus in ischemic cardiomyopathy
After a myocardial infarction, several complex geometric changes to the mitral valve might occur. The leading mechanism to MR in this context is tethering of the chordae and leaflets. This results from LV regional wall motion abnormalities, changes in papillary muscle position, and the direction of tension exerted on mitral leaflets.21,22 Consequently, it leads to a more apical leaflet coaptation and a restricted leaflet closure, resulting in regurgitation. 23 Nevertheless, it is important to highlight that, depending on the infarct location, distinctive ventricular adaptations and tethering patterns may occur, a fact that contributes to the variable degrees of valve incompetence. According to Agricola, et al., 24 ischemic mitral regurgitation may be divided into two subtypes, asymmetric or symmetric,1,2 according to the type of chordae tethering. Depending on the extent and location of LV remodeling, one or both papillary muscles may be affected, resulting in eccentric or central MR, respectively. 25 The first is more frequently associated with an infero-posterior myocardial infarction. The resulting regional wall motion abnormalities lead to leaflet tethering associated with apical, lateral, and/or posterior displacement of the papillary muscles. 26 This leads to the restriction of systolic leaflet motion, particularly the posteromedial scallop and subsequent asymmetric tethering of the chordae tendineae. 22 Under these circumstances, the ejection fraction is often normal or mildly reduced. 22 In contrast, symmetric tethering is more frequently a consequence of a large anterior or multiple previous myocardial infarctions, resulting in global diffuse remodeling with LV systolic dysfunction and reduced ejection fraction. 22
Annular dilation is another finding that plays an additional role in the development of ischemic MR. Post-myocardial infarction, the mitral annular shape tends to become flattened, losing its usual saddle shape and overall height. 21 Furthermore, its diameter and area tend to increase significantly, which further aggravates the insufficiency. 21 This change is frequently asymmetric and often occurs with a higher magnitude along the posterior annulus, as this is an area under increased stress and less densely fibrotic.27,28 Nevertheless, it should be noted that all segments of the mitral annulus dilate in this disease, including the anterior annulus. 27
The annular motion may also be impaired with loss of systolic apical bending that leads to an increase in the circumferential area of the annulus during systole. 13 This loss has been shown to have a good correlation with the degree of reduction in LV global longitudinal strain and ejection fraction.27,28 More recently, LA mechanical dysfunction, namely reservoir strain reduction, seems to play an important role in mitral annulus mechanics after myocardial infarction, especially in the context of preserved ejection fraction.29,30
Several other factors may also influence normal behavior of the mitral valve apparatus. Changes in closing forces generated by the LV may contribute to the development of MR. In a normal-sized LV, little force is necessary to close this valve, even when there is global LV dysfunction. 31 However, in the presence of increased tethering, an even smaller force is exerted over the leaflets, further impairing normal closure of the mitral valve. This results in greater flow and regurgitant orifice area during early and late systole, but paradoxically decreased in mid-systole (when LV pressure is highest). 31 Moreover, the presence of a left bundle branch block may contribute to worsening MR, since papillary muscle contraction becomes dyssynchronous, resulting in complex LV longitudinal, circumferential, and rotational LV mechanics modifications. 25
Leaflet remodeling is also hypothesized to play a role in the development of MR. 21 Patients with mild or low MR seem to have more elongated anterior leaflets, protecting them from valve regurgitation, 32 supporting the theory that the anterior leaflet may actively reshape in response to the mechanical stretching that is exerted.21,32
This complex interplay of papillary muscle displacement, systolic symmetric or asymmetric leaflet tetherings, regional or global LV remodeling, annular dilatation and flattened shape, along with abnormal leaflet remodeling, may result in incomplete mitral leaflet closure and consequent MR after myocardial infarction, even in the absence of organic mitral valve disease.
Mitral valve apparatus in non-ischemic dilated cardiomyopathy
In the setting of non-ischemic dilated cardiomyopathy, significant mitral valve distortion may be present. This tends to occur as a consequence of diffuse and uniform injury to the myocardium, which explains the similarities to symmetric ischemic MR. 33 Global LV remodeling seems to be crucial to the development of MR in this pathology. Indeed, LV diameter, volume, and sphericity are important determinants of the severity of sMR. 34 As a consequence of myocardial disease, the LV may readapt towards a progressively more spherical shape. The increased LV sphericity index leads to radial papillary muscle displacement, symmetric mitral valve leaflet tethering, and sMR.21,22,25
Another major influencing factor is mitral annulus dilatation and loss of annular contraction. 35 As a consequence of myocardial disease, there is increased circularization and a reduction in ring height. 25 However, in contrast to ischemic MR, the annulus enlargement is usually symmetric in non-ischemic circumstances. 21
Mitral valve leaflets also seem to readapt in response to tethering. 36 Just like in ischemic MR, the degree of remodeling may explain the differences in valve competency, despite significant ventricular dilation. Increased mitral leaflet surface seems to be a protective mechanism against the development of sMR.32,36 Another contributing factor is the presence of weaker closing forces of the valve, which is associated with the reduction of LV ejection fraction. 33 Likewise, the presence of left bundle branch block can exacerbate MR through the reduction of closing forces and dyssynchronous papillary muscle contraction. 25
Evaluation of the mitral valve apparatus in cardiomyopathies
A complete evaluation of mitral valve changes in sMR should incorporate not only the recommended measurements to determine severity, but also a thorough evaluation of mitral valve apparatus deformation and LV changes.
Regarding the evaluation of MR severity, various guidelines, including the American Society of Echocardiography (ASE), the European Society of Cardiology (ESC), and the American College of Cardiology/American Heart Association (ACC/AHA) recommend the use of effective regurgitant orifice area (EROA), regurgitant volume (RV), and regurgitant fraction (RF) as quantitative measures.37–39 These can be determined by several different techniques, with the proximal isovelocity surface area (PISA) method being the most frequently used. Depending on the findings, MR may be classified as mild, moderate, or severe. These recommendations are fairly consensual in defining severe MR, recommending the following cutoffs: RV ≥ 60 ml; RF ≥ 50%; and EROA ≥ 0.4 cm2.
The regurgitation orifice is well known to be crescentic and does not fulfill the assumption of a circle orifice in sMR, which is assumed by the PISA method. This can underestimate its severity. Therefore, lower thresholds may be considered when the regurgitant orifice area is elliptical. Indeed, according to the ESC 2021 guidelines, an EROA ≥30 mm2 by the PISA method suggests the presence of severe MR. 38 Moreover, it should be highlighted that patients who fulfill the criteria for moderate MR (EROA ≥0.2 cm2 and RV ≥30 ml) have worse outcomes. 40 This was the reason that ACC/AHA 2014 guidelines stated that this cutoff could be used to identify patients for mitral valve repair. Nevertheless, while acknowledging the inherent limitations of the echocardiographic evaluation of sMR, and despite the fact that use of these lower criteria is more sensitive for the presence of significant sMR, the authors of the 2017 AHA/ACC update of the valvular heart disease guidelines opted for a more specific cutoff of EROA ≥0.4 cm2 and RV ≥60 ml.
Furthermore, sMR has a characteristic biphasic pattern during systole, being maximum during early systole and minimum in mid-systole. This pattern may lead to significant severity overestimation or underestimation, as the PISA method only uses a single time-point measurement. Additionally, the measurement of the PISA radius can be difficult because the exact point of flow convergence is not always clear. These limitations emphasize the importance of a careful and complete evaluation of the MR using a multiparametric approach and including other factors besides the strict quantitative measurements.
The vena contracta size is also one of the main parameters to be measured. These recommendations set a cutoff of ≥7 mm for severe MR. However, it has a significant limitation, since the great majority of patients who have sMR have a non-circular vena contracta. 41 One way to overcome this limitation is to perform a biplane measurement (average between apical two- and four-chamber views), with a threshold of >8 mm for severe insufficiency. 39 With the advent of 3D echocardiography, 3D vena contracta area of >0.4 cm2 has also been proposed as a robust parameter to identify severe MR.42,43
Several complementary measures are recommended, including the pattern of origin and distribution of the MR jet, the evaluation of pulmonary vein systolic flow, and the evaluation of mitral inflow pattern and E wave peak velocity. The morphology of the sMR jet is of utmost importance since it reflects the underlying mechanism. When LV global symmetric remodeling occurs, the typical pattern is a central jet in its origin and direction along the LA with the above-referred biphasic behavior, which may change from mainly early systolic to holosystolic according to patient congestive status (Figure 1a; Supplementary video 1). Conversely, an eccentric jet can occur with a pattern of ‘mitral valve anterior leaflet pseudo prolapse’ in the setting of LV regional wall motion abnormalities inducing pronounced asymmetric tethering with dominant systolic restriction of the posterior leaflet. During systole, the anterior leaflet slides along the restricted posterior leaflet, producing the pseudo prolapse pattern, and an eccentric jet swirls along the posterior lateral wall of the LA (Figure 1b; Supplementary video 2). 8

Echocardiograph images showing examples of functional mitral regurgitation: (a) central mitral regurgitation; and (b) eccentric mitral regurgitation in the setting of anterior leaflet pseudo prolapse.
Taking everything into account, the assessment of multiple parameters is essential in order to determine MR severity, and no single parameter should serve as a stand-alone indicator. Instead, several of the above-mentioned parameters should be integrated, in order to stratify the MR into four different stages, according to the ACC/AHA (Table 1). 37
Stages of secondary mitral regurgitation according to American College of Cardiology/American Heart Association 2020 guideline for the management of patients with valvular heart disease. 37

ERO, effective regurgitant orifice; LA, left atrium; MR, mitral regurgitation.
Despite not being included in the algorithms for grading sMR severity, several other parameters also have clinical significance (Table 2).13,44–48 The degree of mitral valve apparatus deformation and adaptation can be determined by the measurement of several variables (Figure 2). The tenting area is calculated by quantifying the triangular area between the mitral valve leaflets and the mitral annulus. Increased mitral tenting is associated with a more severe mitral valve deformation and consequent worsening MR.49,50 Similarly, tenting volume has been demonstrated to have a significant association with the degree of regurgitation.51,52 An additional simple measurement that renders the degree of distortion of the mitral valve is the tenting height (also known as coaptation height). It corresponds to the distance between the mitral annulus and the coaptation point and has been associated with sMR severity. 53 In addition, an increase in these parameters is associated with a higher probability of unsuccessful mitral valve repair. 21
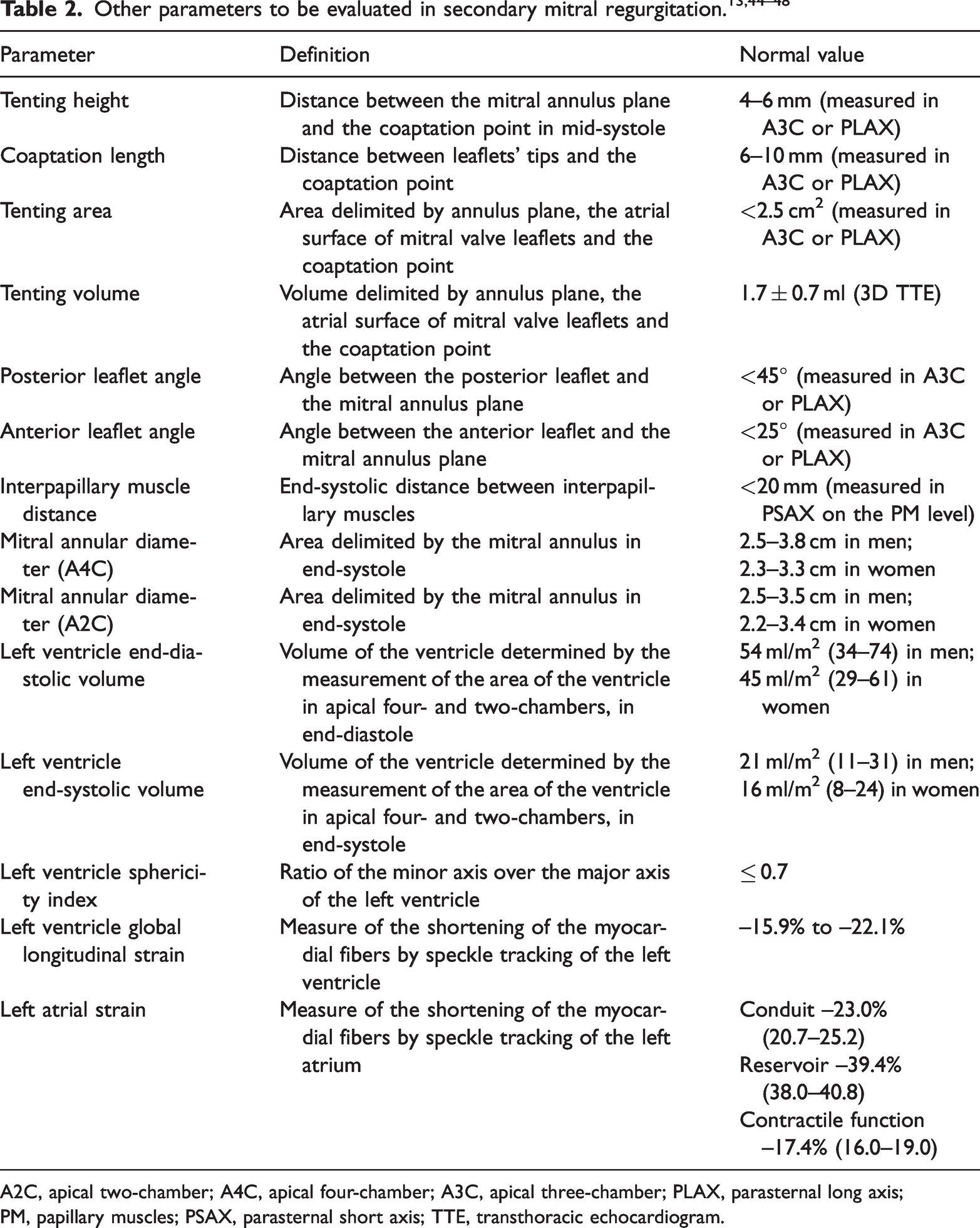
A2C, apical two-chamber; A4C, apical four-chamber; A3C, apical three-chamber; PLAX, parasternal long axis; PM, papillary muscles; PSAX, parasternal short axis; TTE, transthoracic echocardiogram.

Echocardiograph images showing mitral valve displacement measurements: (a) tenting height; (b) coaptation reserve; and (c) tenting area.
Another important parameter to consider in MR evaluation is the coaptation length. With deformation of the mitral valve apparatus, the overlap of leaflets during mitral valve closure shortens, and, consequently, the coaptation length is shortened. This is relevant, as it gives a measure of the coaptation reserve of the leaflets and is a predictor of mitral valve repair success and durability.21,54 Calculating the amplitude of the posterior angle (angle between the posterior leaflet and the mitral annulus plane, in mid-systole) is also relevant, as its increase was associated with worse outcomes in patients with ischemic sMR submitted to restrictive annuloplasty. 55 Measuring the mitral annulus’s diameters and area is also pertinent, as these parameters are associated with MR severity. 56 Likewise, the distance between papillary muscles (measured in parasternal short axis) is significantly correlated with regurgitation severity and is a predictor of the success of restrictive annuloplasty.53,57
In order to fully evaluate the mitral valve apparatus, a detailed assessment of the LV is also essential. Besides myocardial function and the estimation of LV ejection fraction, several other factors are of particular relevance in the setting of sMR. As described previously, LV dilation, sphericity, regional wall motion abnormalities, and dyssynchrony are crucial components to the development of this type of regurgitation. Therefore, the measurement of both diastolic and systolic LV volumes is required.58,59 Quantification of LV diameters is also relevant, as a diastolic value above 65 mm and a systolic value over 51 mm seem to be predictors of poor response to mitral valve repair. 44 Similarly, the sphericity of this cavity, estimated by the LV sphericity index, is important, as a more spherical cavity is associated with higher degrees of sMR. Besides their role in the assessment of the regurgitation’s severity and mechanism, these variables are also relevant tools to monitor the progressive remodeling of the LV. More recently, the determination of the LV global longitudinal strain, as well as the LA strain, have come up as important prognostic factors in these patients, providing incremental value for predicting all-cause mortality over routine parameters.30,60,61
Additionally, it is mandatory to assess the presence of LV electro-mechanical dyssynchrony, which produces significant regurgitation (either central or eccentric). In these cases, sMR is expected to be reduced or resolved with cardiac resynchronization therapy. The guideline parameters to be checked are left bundle branch block with a QRS duration of more than 130 ms and LV ejection fraction of less than 35%. 62 It is important to emphasize that LV mechanical parameters can add prognostic information with respect to cardiac resynchronization therapy response grading. The presence of pre-systolic septal contraction (septal flash) and apical rocking as markers of left bundle branch block dyssynchrony, along with time to peak longitudinal strain, LV remodeling, and sMR, are the main clue parameters to be depicted as adjunctive to the guideline.63,64
Cardiac magnetic resonance imaging can also provide complementary information to echocardiography in patients with MR. This method has emerged as a new technique in the evaluation of these patients and may be useful in the assessment of the unclear severity of MR measured by echocardiography. Furthermore, it can provide an accurate assessment of LV volumes and function, in addition to the identification and quantification of myocardial scar (focal and diffuse).65,66 New advances in 4D flow cardiac magnetic resonance imaging are growing, and potentially will be helpful in the future management of mitral valve regurgitation. 67
Conclusion
Mitral valve morphological and mechanical disturbance in cardiomyopathy is a multifactorial problem that arises from a distortion of the mitral valve apparatus in the presence of an apparently normal mitral valve. Depending on the etiology, ischemic or non-ischemic, different mechanisms and sMR patterns may predominate. A complete assessment of these patients is essential, not only to determine the severity and prognosis of the underlying pathology, but also to establish the predominant mechanism in order to define the most appropriate treatment approach for each patient.
Supplemental Material
sj-mp4-1-imr-10.1177_03000605231218645 - Supplemental material for Parameters of the mitral apparatus in patients with ischemic and nonischemic dilated cardiomyopathy
Supplemental material, sj-mp4-1-imr-10.1177_03000605231218645 for Parameters of the mitral apparatus in patients with ischemic and nonischemic dilated cardiomyopathy by João Presume, Mariana S Paiva, Sara Guerreiro and Regina Ribeiras in Journal of International Medical Research
Supplemental Material
sj-mp4-2-imr-10.1177_03000605231218645 - Supplemental material for Parameters of the mitral apparatus in patients with ischemic and nonischemic dilated cardiomyopathy
Supplemental material, sj-mp4-2-imr-10.1177_03000605231218645 for Parameters of the mitral apparatus in patients with ischemic and nonischemic dilated cardiomyopathy by João Presume, Mariana S Paiva, Sara Guerreiro and Regina Ribeiras in Journal of International Medical Research
Footnotes
Author contributions
Conception and design (JP, MSP, SG, RR), drafting (JP, MSP, RR), revising (JP, MSP, SG, RR). All authors read and approved the final manuscript.
Declaration of conflicting interests
The Authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.