
Abstract
We tested the hypothesis that olmesartan, an angiotensin II receptor blocker (ARB) devoid of peroxisome proliferator-activated receptor γ agonist activity, would improve whole-body insulin sensitivity in overweight and obese individuals with elevated blood pressure (BP). Sixteen individuals (8 women, 8 men; age=49.5 ± 2.9 years; body mass index=33.0 ± 1.7 kg/m2) were randomly assigned in a crossover manner to control and ARB interventions. Insulin sensitivity was determined from intravenous glucose tolerances tests before and after each 8-week intervention. BP, body weight, body fat, lipid and lipoprotein concentrations, and insulin sensitivity were similar at baseline for both treatments (all p > 0.05). Diastolic BP and triglyceride concentrations were higher (p = 0.007 and 0.042 respectively) at baseline for the ARB compared with the control intervention. Systolic (−11.7 mmHg; p = 0.008) and diastolic (−12.1 mmHg; p = 0.0001) BP decreased, however insulin sensitivity did not change (p > 0.05) following ARB treatment. Furthermore, there were no significant correlates of changes in insulin sensitivity following the ARB intervention. In summary, our findings indicate that short-term ARB treatment did not affect whole-body insulin sensitivity in overweight or obese individuals with elevated BP. Future studies are needed to clarify the effect of individual ARBs on insulin sensitivity in obesity.
Introduction
Obesity is a major risk factor for the development of numerous chronic diseases [Wang et al. 2011]. More than half of overweight and obese individuals develop hypertension [Garrison et al. 1987]. In addition, obese individuals are also insulin resistant and at increased risk of type 2 diabetes [Defronzo and Ferrannini, 1991; Moller and Flier, 1991; Chan et al. 1994].
Overactivation of the renin–angiotensin system (RAS) has been implicated as a mechanism contributing to insulin resistance and type 2 diabetes in overweight and obese individuals with hypertension [Prasad and Quyyumi, 2004; Scheen, 2004a,b]. The primary role of the RAS is to regulate arterial pressure and sodium balance. However, chronic elevations in angiotensin II impair whole-body insulin sensitivity and insulin signaling in skeletal muscle via angiotensin II type 1 receptor activation [Henriksen et al. 2001; Sloniger et al. 2005; Wei et al. 2006, 2008]. In addition, the results of several meta-analyses suggest that the incidence of new-onset diabetes is lower in patients taking ARBs compared with placebo or other antihypertensives including diuretics, β blockers and calcium channel blockers [Scheen, 2004a; Andraws and Brown, 2007; Elliott and Meyer, 2007].
Randomized controlled trials addressing the influence of angiotensin II receptor blockers (ARBs) on insulin sensitivity have been conflicting. Some [Fogari et al. 2005; Vitale et al. 2005; Ichikawa, 2007; Nishimura et al. 2008; Fogari et al. 2009; De Luis et al. 2010; Derosa et al. 2011; Van Der Zijl et al. 2011] but not all studies [Moan et al. 1996; Fogari et al. 1998; Parhofer et al. 2010; Mori et al. 2011; Goossens et al. 2012; Lteif et al. 2012; Perlstein et al. 2012] support an insulin-sensitizing effect of ARBs. ARBs with partial peroxisome proliferator-activated receptor γ (PPARγ) agonist activity, such as telemisartan, appear to consistently improve insulin sensitivity [Vitale et al. 2005; Ichikawa, 2007; Fogari et al. 2009; De Luis et al. 2010]. However, the outcomes of studies involving ARBs other than telemisartan are equivocal [Moan et al. 1996; Fogari et al. 1998, 2005; Vitale et al. 2005; Ichikawa, 2007; Nishimura et al. 2008; De Luis et al. 2010; Parhofer et al. 2010; Derosa et al. 2011; Van Der Zijl et al. 2011; Goossens et al. 2012; Lteif et al. 2012; Perlstein et al. 2012]. In addition, many of these studies have relied on indirect, surrogate measures of insulin sensitivity. Thus, the impact of other ARBs on insulin sensitivity remains unclear. To clarify this issue, we tested the hypothesis that olmesartan, an ARB devoid of the PPARγ agonist activity [Benson et al. 2004; Erbe et al. 2006], would improve insulin sensitivity in middle-aged to older overweight and obese adults with elevated blood pressure (BP). To address this, we conducted a randomized crossover study and assessed insulin sensitivity using the insulin-modified intravenous glucose tolerance test (IVGTT) before and after each treatment period. In addition, skeletal muscle is the primary tissue responsible for insulin-stimulated glucose disposal [Ferrannini et al. 1988] and inflammation and alterations in the extracellular matrix of skeletal muscle have been associated with the development of insulin resistance [Berria et al. 2006; Shoelson et al. 2006]. Therefore, a secondary exploratory aim of the study was to determine whether changes in expression of proinflammatory and extracellular matrix genes predict changes in insulin sensitivity in our sample.
Materials and methods
Study participants
Sixteen sedentary (moderate to hard activity ≤3 days/week), overweight and obese [body mass index (BMI)
Intervention
Study participants first completed baseline testing sessions within a 2-week period. They were then randomized to one of two treatments olmesartan medoxomil (Benicar, Daiichi Sankyo, Inc., Parsippany, NJ; ARB) or no medication (control) for 8 weeks. The study used a randomized crossover design. When assigned to the olmesartan treatment, participants were provided with daily 20 mg pills for the first 2 weeks. They received additional daily doses of 40 mg olmesartan for the remainder of the study period. The dose remained at 20 mg per day, however, if their BP fell below 110/70 mmHg during the first 2 weeks. They also continued taking the drug during the 2-week follow-up period. There was no drug intervention during the control period. After the first 8-week intervention, study participants participated in post-testing sessions, followed by a 2-week washout period. They then completed the testing sessions again and participated in the opposite intervention. This was followed by post-testing sessions after 8 weeks. During each intervention period and the washout period, BP was measured weekly. Study participants were asked to maintain their current physical activity level, dietary intake and body weight throughout the study.
Measurements
All testing sessions were performed between 7 a.m. and 1 p.m. after a 12-hr fast. Before each testing session, study participants recorded recent infection or illness on an infection/inflammation questionnaire. If an infection/illness was reported, testing was delayed 1–2 weeks for recovery. Study participants refrained from vigorous physical activity for 48 h before testing. They also abstained from ingesting nonsteroidal anti-inflammatory drugs or other medication that may have interfered with study measurements for 72 h prior to the session. BP measurements were documented at each visit.
Resting blood pressure
BP measurements were performed between 7 a.m. and 11 a.m. with serial BP appointments scheduled at the same time for each individual. BP was measured by automated sphygmomanometry (Pilot model 9200, Colin Instruments Corp., San Antonio, TX) in the upright seated posture. Measurements were taken every 3 min after a 5–10 min seated rest and continued until BP stability [± 6 mmHg systolic BP (SBP) and diastolic BP (DBP)] was reached between three consecutive recordings. Baseline BP stability was established after three BP sessions spanning at least 1 week were completed before any testing sessions were performed. For individuals who discontinued their BP medications, six testing sessions over 2 weeks were completed to ensure BP stability.
Body mass and composition
Body weight was measured to the nearest ±0.1 kg on a digital scale (Model 5002, Scale-Tronix, White Plains, NY). Height was measured to the nearest ±0.1 cm using a stadiometer. Body composition (total fat and fat-free mass) was analyzed by dual-energy x-ray absorptiometry (GE Lunar Prodigy Advance, software version 8.10e, Brookfield, WI).
Dietary and physical activity assessment
Before and after each 8-week intervention period, habitual dietary intake was assessed from self-reported 4-day food records. A registered dietitian provided study participants with written and verbal instruction for accurately measuring and recording food intake. The Nutrition Data Systems for Research software (NDS-R 2006, University of Minnesota, Minneapolis, MN, USA) was used to estimate energy and macronutrient content. Habitual physical activity level was measured by an accelerometer (GT1M, Actigraph, Pensacola, FL) worn for 4 consecutive days before and after each intervention.
Plasma lipid and lipoprotein concentrations
Blood samples were drawn with minimal venous stasis. Plasma total cholesterol, high-density and low-density lipoprotein, and triglyceride concentrations were measured by a commercial laboratory (Solstas Lab Partners, Roanoke, VA, USA) using conventional enzymatic methods.
Circulating inflammatory peptides
A Bioplex Pro coupled magnetic bead assay (Bio-rad, Hercules, CA, USA) assessed plasma concentrations of inflammatory markers, tumor necrosis factor α (TNFα), interleukin (IL)-6, IL-10, and monocyte chemoattractant protein 1 (MCP-1). Enzyme-linked immunosorbent assays (ELISAs) were performed to measure total and high-molecular weight adiponectin (ALPCO Diagnostics, Salem, NH, USA).
Estimated insulin sensitivity
Systemic insulin sensitivity was estimated using Bergman’s minimal model (MINMOD Millennium software, version 6.02, Minmod, Inc., Pasadena, CA) during a modified frequently sampled IVGTT [Boston et al. 2003]. An intravenous catheter was inserted in an antecubital vein of each arm for blood collection or glucose and insulin injection. Two baseline plasma blood samples [(t) = −10 and −1 min] were drawn. Glucose (0.3 g/kg; 50% solution) was injected at time 0 and insulin (0.025 U/kg) at (t) = 20 min. Additional blood samples (6 ml) were collected at (t) = 1, 2, 3, 4, 5, 6, 7, 8, 10, 12, 14, 16, 18, 22, 23, 24, 25, 27, 30, 40, 50, 60, 70, 80, 90, 100, 120, 150, and 180 min during the 3-hr protocol. Glucose concentration (mg/dl) was analyzed immediately using a YSI Glucose Analyzer (Yellow Springs, OH, USA). Insulin (µU/ml) was determined later via ELISA (ALPCO Diagnostics, Salem, NH, USA). Samples were analyzed in duplicate. Thirteen individuals successfully completed all IVGTTs.
Skeletal muscle biopsy
Skeletal muscle samples were taken by needle aspiration from the vastus lateralis. The skin was cleaned with a providone-iodine solution and local anesthetic (50:50 2% xylocaine/0.25% bupivacaine; 10 ml total) was used to numb the skin and tissue. A small (~1/4”) incision was made with a #10 scalpel. Approximately 500 mg of skeletal muscle tissue was collected using suction applied to a 5 mm modified Bergstrom needle. The incision was cleaned with saline and closed with sterile bandage strips. Ice and pressure was applied to minimize discomfort. Tissue samples were immediately washed in 0.9% sterile saline to remove blood and connective tissue. Samples were weighed and immediately flash frozen in liquid nitrogen for future analysis. One study participant declined to have biopsies performed.
Skeletal muscle RNA extraction and quantitative real-time polymerase chain reaction
RNA extraction and quantification were determined using methods previously described by Frisard and colleagues [Frisard et al. 2010]. Briefly, an RNeasy Mini Fibrous Kit and DNase I treatment (Qiagen, Valencia, CA, USA) were used according to the manufacturer’s directions for mRNA extraction. Quantitative real-time polymerase chain reaction (qRT-PCR) measured the expression of nicotinamide adenine dinucleotide phosphate oxidase 4, transforming growth factor β, IL-6, collagen III, and MCP-1 using an ABI PRISM 7900 Sequence Detection System instrument and TaqMan Universal PCR Master Mix according to the manufacturer’s instructions (Applied Biosystems, Foster City, CA, USA). Relative gene expression levels were determined using the number of cycles necessary to reach threshold and results were normalized to cyclophilin B RNA levels.
Statistical analysis
Repeated measures analysis of variance was used to assess the effect of treatment (olmesartan treatment versus control), time, and treatment by time interaction on the dependent variables of interest. Treatment order was used as a covariate in models when its main effect was significant. There was no effect of gender on the study outcomes. Thus, the men and women are presented as a single group. Since we have a small sample, we reran these analyses with standard error estimates based on 1000 bootstrap samples to obtain bias-corrected confidence intervals by repeated re-estimations of the parameter estimates. Paired sample t-tests were used to compare the changes in dependent variables of interest. Pairwise associations among variables were analyzed using Pearson’s product moment correlations. All data are presented as means ± standard error of the mean. Significance level was set a priori at p < 0.05.
Results
A total of 16 out of 20 (80%) randomized study participants completed the interventions. The study medication, olmesartan, was well tolerated and there were no adverse events reported. Seven study participants remained on the 20 mg dose for the duration of the intervention while nine received an increased dose of 40 mg after the initial 2-week period. Adherence during the 8-week olmesartan intervention was 98.4% overall, with no individual missing more than three daily doses in total.
Characteristics of study participants before and after each treatment are depicted in Table 1. There were no significant differences between ARB and control before the treatment period with the exception that DBP and triglycerides were higher in the ARB treatment compared with the control treatment at baseline (p = 0.007 and 0.042 respectively). As expected, there was a significant reduction in both SBP (–11.7 mmHg; –8.3%) and DBP (–12.1 mmHg; –14.2%) with ARB treatment. Body weight, BMI, body fat %, and total body fat mass increased (all p < 0.05) over time but there were no significant differences between treatments. Triglyceride levels remained higher throughout treatment in the ARB compared with the control (p = 0.038). No differences in lipid and lipoprotein or fasting plasma glucose concentrations were observed between treatments (all p > 0.05).
Study participant characteristics before and after the control and ARB treatment.
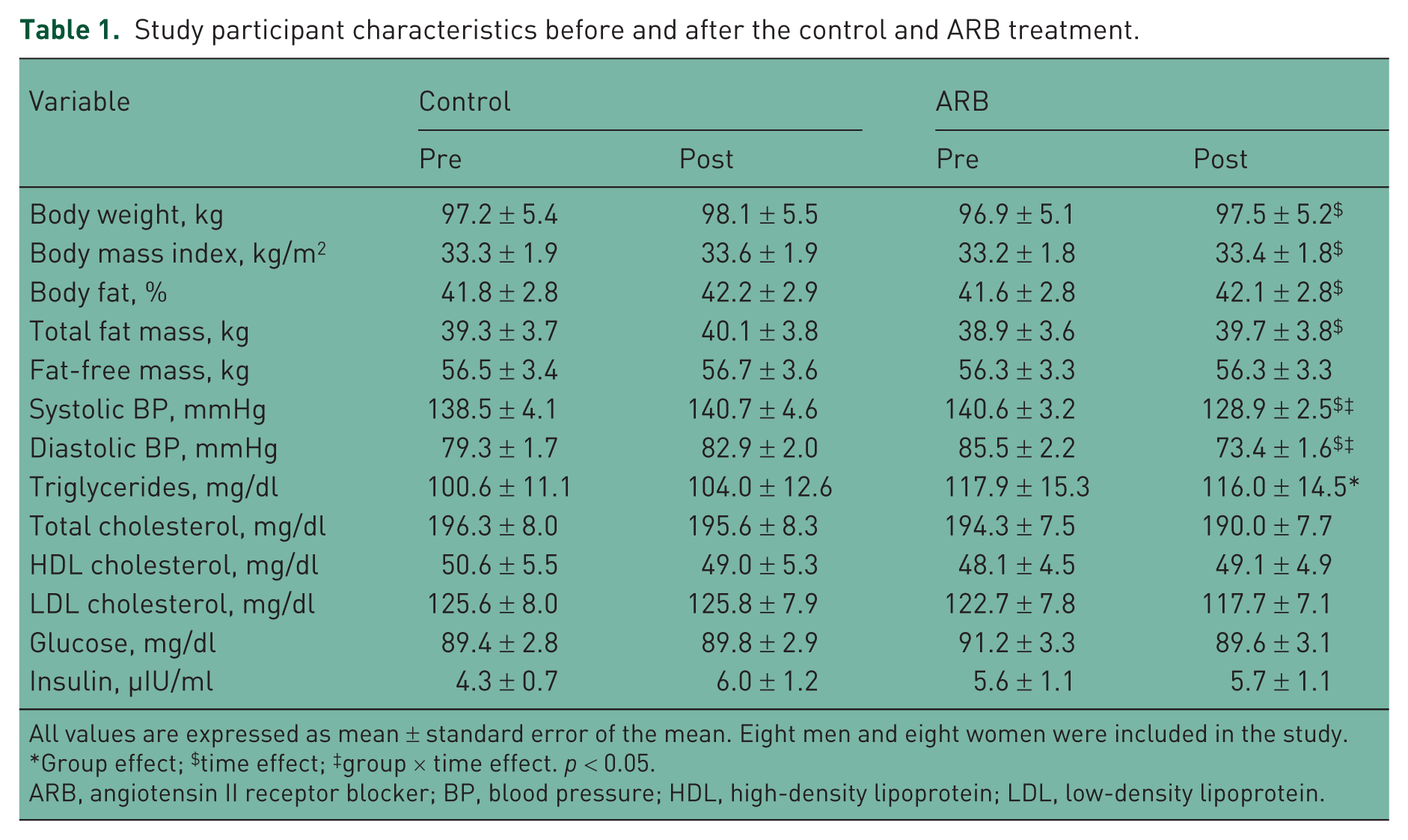
All values are expressed as mean ± standard error of the mean. Eight men and eight women were included in the study.
Group effect; $time effect; ‡group × time effect. p < 0.05.
ARB, angiotensin II receptor blocker; BP, blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Habitual physical activity and self-reported dietary intake during ARB and control treatment are shown in Table 2. There were no significant changes in physical activity level or self-reported total calorie or macronutrient intake during either treatment period. The absolute (g) and relative (%) fat intake were lower (p = 0.021 and 0.047 respectively) during the ARB compared with control treatment. The percentage carbohydrate intake was higher (p = 0.012) in the ARB compared with the control treatment. Protein and alcohol intake did not differ during the ARB or control treatment. Cholesterol, saturated fatty acid, fiber, and sodium intake all remained unchanged during the treatments.
Physical activity and dietary intake before and after the control and ARB treatment.

All values are expressed as mean ± standard error of the mean. Eight men and eight women were included in the study.
Group effect. p < 0.05.
ARB, angiotensin II receptor blocker; SFA, saturated fatty acid.
The IVGTT variables before and after each treatment period are depicted in Figure 1. There were no significant differences for any of the IVGTT variables at baseline between the ARB and control treatments. Insulin sensitivity index (SI) and glucose effectiveness (Sg) did not change throughout the study. A significant effect of time was detected for acute insulin response to glucose (AIRg) and disposition index (DI) (p = 0.026 and 0.045 respectively) during the treatment periods (Figure 2). However, neither AIRg nor DI changed significantly during ARB or control treatment. There was no significant effect of olmesartan dose on the IVGTT-related outcomes. In addition, the removal of smoker status from the analysis did not change the primary findings except that the time effect for AIRg was no longer significant (p = 0.072). The bootstrapping procedure did not change the results of the IVGTT outcomes described above.

Absolute values of insulin sensitivity index (SI) (a) and glucose effectiveness (Sg) (b) before and after the control and angiotensin II receptor blocker (ARB) treatment. Values are mean ± standard error of the mean. n =12 study participants.

Absolute values of the acute insulin response to glucose (AIRg) (a) and disposition index (b) before and after the control and angiotensin II receptor blocker (ARB) treatment. Time effect (†), p < 0.05. Values are mean ± standard error of the mean. n = 12 study participants.
Circulating cytokine and adiponectin concentrations are presented in Table 3. Baseline concentrations of all circulating inflammatory markers were not different between the treatment periods (p > 0.05). There was a trend (treatment effect, p = 0.065) for a higher MCP-1 concentration in the ARB compared with the control treatment. There were no significant changes in IL-6, IL-10, or TNFα with ARB treatment. Similarly, there were no significant changes in circulating total or high-molecular weight adiponectin concentrations in the ARB or control treatment.
Circulating plasma cytokine and adiponectin levels before and after the control and ARB treatment.

All values are expressed as mean ± standard error of the mean. Eight men and eight women were included in the study.
ARB, angiotensin II receptor blocker; HMW, high molecular weight; IL, interleukin; MCP-1, monocyte chemoattractant protein 1; TNFα, tumor necrosis factor α.
Muscle mRNA expression levels are presented only for the ARB treatment due to insufficient RNA yield for the majority of participants during the control treatment (Table 4). There were no significant changes in mRNA expression levels of any of the target genes from pre- to post-ARB treatment.
Skeletal muscle mRNA before and after ARB treatment.

All values are expressed as mean ± standard error of the mean.
ARB, angiotensin II receptor blocker; COL3, collagen III; IL, interleukin; MCP-1, monocyte chemoattractant protein 1; NOX4, nicotinamide adenine dinucleotide phosphate oxidase 4; TGFβ, transforming growth factor β.
There were no baseline characteristics or IVGTT-related variables that were correlated with changes in SI, Sg, or DI (all p > 0.05). The change in fasting insulin was associated with the change in AIRg (p = 0.011). However, there were no other changes in variables that correlated with SI, Sg, or DI (all p > 0.05).
Discussion
The results of our randomized crossover trial demonstrate that an 8-week period of olmesartan treatment does not affect insulin sensitivity in overweight and obese people with elevated BP. We did not observe significant changes in circulating inflammatory markers or skeletal muscle inflammatory or collagen gene expression following olmesartan treatment. In addition, there were no significant correlates of changes in insulin sensitivity in response to olmesartan treatment.
Meta-analyses of large clinical trials of antihypertensive therapy have suggested that the incidence of new-onset diabetes is lower in patients taking ARBs compared with placebo or other antihypertensives such as diuretics, β blockers, and calcium channel blockers [Scheen, 2004a; Elliott and Meyer, 2007]. In addition, numerous studies in nondiabetic hypertensive or diabetic animal models have demonstrated improvements in whole-body insulin sensitivity after ARB therapy [Sasaki et al. 1999; Henriksen et al. 2001; Furuhashi et al. 2004; Shiuchi et al. 2004].
Previous trials on the effects of ARB on insulin sensitivity in humans have been conflicting. The results of some randomized controlled trials have suggested improvements in insulin sensitivity with ARB treatment compared with other antihypertensive medications [Paolisso et al. 1997; Fogari et al. 2005, 2009; Vitale et al. 2005; Ichikawa, 2007; Nishimura et al. 2008; De Luis et al. 2010; Derosa et al. 2011; Van Der Zijl et al. 2011]. However, many of these studies relied on imprecise measures of insulin sensitivity (e.g. Homeostasis Model of Assessment-Insulin Resistance) [Fogari et al. 2005; Vitale et al. 2005; Ichikawa, 2007; Nishimura et al. 2008; De Luis et al. 2010]. Van der Zijl and colleagues reported a significant improvement in insulin sensitivity in people treated with valsartan compared with those on placebo [Van Der Zijl et al. 2011]. However, the small treatment effect and relatively larger reduction in insulin sensitivity in the placebo-treated individuals makes interpretation of this study difficult. Our present study and others [Laakso et al. 1996; Moan et al. 1996; Fogari et al. 1998; Parhofer et al. 2010; Goossens et al. 2012; Lteif et al. 2012; Perlstein et al. 2012] suggest no improvement in whole-body insulin sensitivity following ARB treatment. The reasons for this apparent discrepancy are unclear but do not appear to be related to the duration of treatment, method used to assess insulin sensitivity, or study population. Rather, the partial PPARγ agonist activity of the particular ARB studied may be important.
Some ARBs, such as telmisartan, exhibit partial PPARγ agonist activity [Benson et al. 2004; Schupp et al. 2004; Kurtz, 2005, 2006]. PPARγ activation enhances insulin’s effectiveness to promote glucose uptake in peripheral metabolic tissues [Picard and Auwerx, 2002]. Thus, some ARBs can influence insulin action via pathways independent of angiotensin II signaling [Schupp et al. 2004; Kurtz, 2005, 2006]. This observation may contribute, at least in part, to the different outcomes observed in previous studies on this issue [Vitale et al. 2005; Benndorf et al. 2006; Ichikawa, 2007; Fogari et al. 2009; De Luis et al. 2010]. We used olmesartan in the present study because it is devoid of partial PPARγ agonist activity [Benson et al. 2004; Erbe et al. 2006]. Therefore, future studies are necessary to clarify whether the ability of ARBs to improve insulin sensitivity depend on intrinsic PPARγ agonist activity.
There are some limitations of our study that should be considered. The sample size was small and the majority of study participants were white. In addition, our sample was limited to overweight and obese individuals with high normal or stage 1 hypertension. Furthermore, it is possible that the ability of ARB treatment to improve insulin sensitivity may depend on baseline insulin resistance. Although overweight and obese individuals tend to be insulin resistant as a population, baseline insulin sensitivity was not correlated with the change in insulin sensitivity with ARB treatment. Future studies will be necessary to more comprehensively address this issue. Finally, the statistical analysis of the inflammatory and collagen gene targets by qRT-PCR was limited by the extraction of sufficient mRNA from the samples collected during each biopsy.
In conclusion, our findings suggest that ARB treatment with olmesartan for 8 weeks does not improve insulin sensitivity in overweight and obese individuals with elevated BP. Furthermore, there were no significant changes in inflammatory and collagen mRNA expression in skeletal muscle following ARB treatment. Taken together, the results of our study suggest that an improvement in insulin sensitivity is not among the additional benefits of olmesartan that extend beyond its BP-lowering capability [Benson et al. 2004]. Further research is needed to delineate which RAS antagonists improve whole-body insulin sensitivity during RAS inhibition and, if so, what populations are most likely to benefit.
Footnotes
Acknowledgements
We would like to thank the participants for their time and commitment to the study.
Funding
This study was supported by a National Institutes of Health HL092572 grant (to KPD).
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.