
Abstract
Background:
The appropriate treatment strategy for secondary stroke prevention in patients with cryptogenic stroke and patent foramen ovale (PFO) remains challenging. The aim of this study was to describe a case series of patients with PFO and complex septal anatomy who underwent percutaneous correction using a FIGULLA (Occlutech®) septal occluder (FSO).
Patients:
Ten consecutive patients (6 females, 4 males, mean age 41.6 ± 16.0 years, range 17–52 years; Group 1) with cryptogenetic stroke and/or transient cerebral ischemia and complex septal anatomy, as defined by intraprocedural transesophageal echocardiogram (TEE) were compared with a group of 25 patients (10 females, 15 males, mean age 43.7 ± 12.3 years; Group 2) with usual tunnel-like PFO anatomy in whom PFO was closed by an Amplatzer septal occluder (ASO; AGA®).
Results:
No significant differences were noted between Group 1 and Group 2 for immediate success rate, residual intraprosthetic shunt at the end of the procedure, discharge, 1, 6 and 12 months follow up, number of attempts, procedure time, fluoroscopy time, or cardiac complication (atrial arrhythmias, device embolism).
The only significant difference was shown for delivery sheath size (11 ± 2 versus 9 ± 1 F) and incidence of local hematoma (30% versus 12 %) between Group 1 and Group 2, without any clinical consequence (need of transfusion) or increase in length of stay.
Conclusion:
FSO shows high performance in patients with PFO and complex septal anatomy when compared with patients with PFO and uncomplicated atrial anatomy treated by ASO. Its favorable behavior is probably related to fabric features such as the total amount of metal and the presence of titanium.
Introduction
The appropriate treatment strategy for secondary stroke prevention in patients with cryptogenic stroke [Ma et al. 2004; Homma et al. 1994] and patent foramen ovale (PFO) remains challenging.
The clinical and anatomic risk factors associated with stroke recurrence include older age [Ma et al. 2004], large PFO [Homma et al. 1994; Hausmann et al. 1995; Stone et al. 1996; Schuchlenz et al. 2000] and large right-to-left shunting [De Castro et al. 2000], combined atrial septal aneurysm (ASA) [Meissner et al. 2006; Mas et al. 2001] and hypertrophic Eustachian valve (HEV) [Meier, 2009]. PFO is an anatomical variant of the atrial septum, providing communication between the atrial chambers of the heart through fossa ovalis on the right side and the ostium secundum on the left side. Septum primum acts as a one-way valve allowing for blood flow from the right to left atria. This septum normally remains patent before birth and closes with the first breath [Gill, 2005].
Autopsy studies have shown an overall PFO prevalence of 27% in the general population, decreasing with increasing age (35% and 20% in age groups less than 30 years and more than 80 years, respectively) [Lechat et al. 1988; Hagen et al. 1984], secondary to either selective mortality of patients with PFO with age or late spontaneous closure.
Transthoracic echocardiography (TTE) allows the population screening by the detection of a shunt with either color Doppler or agitated saline contrast with Valsalva maneuver [Gill and Quaife, 2005; Gramiak et al. 1969; Woods and Patel, 2006; Ha et al. 2001].
Transcranial Doppler (TCD) provides the detection of cerebral flow modification due to right to left shunt during Valsalva maneuver [Droste et al. 1999; Nedeltchev and Mattle, 2006].
Transesophageal echocardiogram (TEE) or intracardiac echocardiogram are generally used during percutaneous closure to monitor the procedures [Meier, 2009].
The classic tunnel-like anatomy of PFO may be more complex for the presence of several associated defects such as: large defects (greater than 4 mm), ASA, HEV and septal multiple cribrosity (SMC) [Meier, 2009; Roelandt and Budts, 2009; Butera et al. 2006].
The aim of this study is to describe a case series of patients with PFO and complex septal anatomy who underwent percutaneous correction by FIGULLA (Occlutech ®) septal occluder (FSO) as compared with a group of patients with usual PFO anatomy who underwent percutaneous closure by Amplatzer (AGA®) septal occluder (ASO).
Patients and methods
Ten consecutive patients (6 females, 4 males, mean age 41.6 ± 16.0 years, range 17–52 years; Group 1) with cryptogenetic stroke and/or transient cerebral ischemia and complex septal anatomy, as defined by intraprocedural TEE, were referred to our institution for PFO percutaneous closure (Table 1 and Figures 1–3). They were compared with 25 patients (10 females, 15 males, mean age 43.7 ± 12.3 years; Group 2) with usual tunnel-like PFO anatomy in whom PFO was closed by an Amplatzer septal occluder (ASO; AGA®) (Table 1). Diagnosis was done in all of these patients by TTE and TCD. Hypercoagulability was screened and excluded in all.
Patients’ anatomic and clinical features.

HEV, hypertrophy of Eustachian valve; SMC, septal multicribrosity; ASA, atrial septal aneurysm; mTIA, multiple transient ischemic attack; PFO, patent foramen ovale; H, hemicrania.
Patient in work up for liver retransplantation.

Atrial septal aneurysm.

Septal multicribrosity.

Eustachian hypertrophy.
All patients underwent percutaneous PFO closure under general anesthesia and orotracheal intubation. All procedural steps were monitored by TEE.
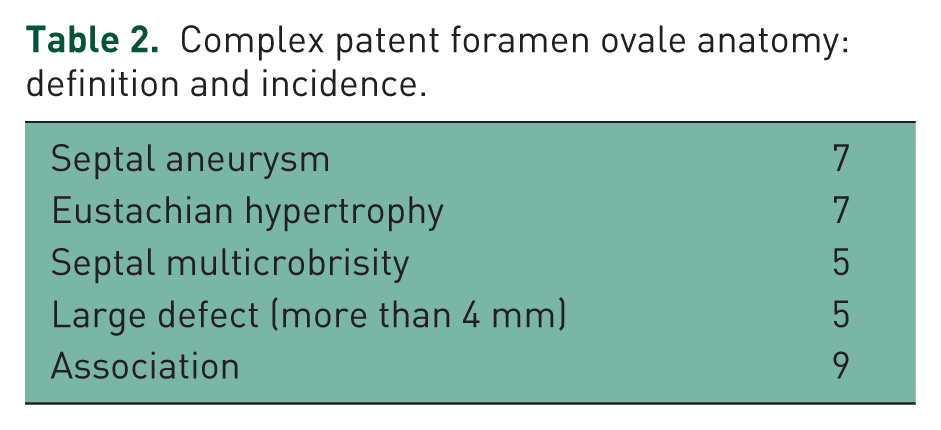
Complex septal anatomy was defined as the presence and/or association of the following parameters: (1) large or long defects (greater than 4 and/or 7 mm, respectively); (2) ASA; (3) HEV; (4) SMC (Tables 1 and 2 and Figures 1–3).
Complex patent foramen ovale anatomy: definition and incidence.
Given its conformability and elasticity, the double-layer FSO (Occlutech®) was chosen to treat these complex cases.
The FSO device is constructed from 0.082–0.186 mm nitinol wires that are tightly woven into two flat round disks with a 4 mm connecting waist.
The prosthesis is filled with a polyester patch to enhance thrombogenicity. There is only one stainless steel hub (microscrew) at the right atrial disk for cable connection (Figure 4).

FIGULLA device.
A Mullins long sheath was selected for delivery of the device, advanced over an angiographic wire to the left atrium.
After sheath de-airing, the device was then vigorously flushed with saline before introduction into the loading catheter. It was then engaged into the delivery sheath and advanced into the left atrium. Under fluoroscopic guidance, withdrawal of the Mullins sheath allowed the release of the left atrial disk. Then the whole system was withdrawn so that the disk engaged the septum. If the position of the left disk was satisfactory under TEE study, the right disk was extruded by pulling back the sheath.
The operator then pushed and pulled the loading catheter several times to confirm the stability of the device. Once the device was implanted well in the position, it was released by releasing the loader.
A residual shunt was considered to be present if echo-contrast showed a right to left shunt across the atrial septum during Valsalva maneuver.
Trivial shunt occurring across the device fabric immediately after the deployment of the device was not considered significant [Butera et al 2004].
Cardiac complication was defined as (1) prosthesis immediate or late embolism and (2) significant atrial arrhythmias (sustained atrial tachycardia or transient atrial fibrillation).
All patients underwent clinical examination, electrocardiography, chest radiographs and TTE before discharge, at 1, 6 and 12 months after the procedure.
Antiplatelet therapy with aspirin, 5 mg/kg orally per day, was prescribed for 6 months.
Statistical analysis
All analyses were performed using SPSS version 10.0 (SPSS, Inc., Chicago, IL) statistical software. The results were expressed as the mean ± SD, unless otherwise stated. Differences between outcomes in different groups of patients were analyzed by unpaired Student’s t-test.
Incidences in the groups were tested for significance with the chi-squared test. A p value of 0.05 was regarded as statistically significant.
Results
As FSO was used starting only from the past year, the mean clinical follow up was significantly longer in Group 2 (Table 3).
Patients characteristics, procedure variables and follow-up.

FSO, FIGULLA septal occluder; ASO, Amplatzer septal occluder; ns, nonsignificant.
No significant differences were noted between Group 1 and Group 2 for immediate success rate, residual intraprosthetic shunt at the end of the procedure, discharge, 1, 6 and 12 months follow up, number of attempts, procedure time, fluoroscopy time or cardiac complication (atrial arrhythmias, device embolism) (Table 3).
The only significant difference between Group 1 and Group 2 resulted from delivery sheath size (11 ± 2 versus 9 ± 1 F) and incidence of local hematoma (30% versus 12%) (Table 3), without any clinical consequence (no need of transfusion or increase in hospital stay).
Residual intraprosthetic or periprosthetic shunt was not significantly different between Group 1 and Group 2 at 1 year (10% and 8%, respectively) (Table 3).
Discussion
ASO is one of the most frequently used devices for ASD and has been proven to be highly effective and safe in the early to long term. Previous reports have confirmed that transcatheter closure of ASD with the ASO not only achieved a comparable efficacy and safety with that of surgical closure but had an additional advantage of causing fewer complications, requiring a shorter hospital stay and avoidance of a permanent skin scarring.
The device handles very well and can be recaptured after deployment of both disks and thus can be repositioned quite easily.
However, there are important differences between the two devices. The ASO is made up of a nitinol wire tube that is clamped in two stainless steel hubs, one on each side of the disk. In contrast, the Occlutech FIGULLA device is individually braided, avoiding a distal clamp. This may be of potential benefit to decrease the chance of a clot formation on the left atrial disk and increases flexibility of the device. Furthermore FSO has significantly less metal and is partly made from titanium which has increased biocompatibility (less nickel content). FSO is available from the manufacturer in two configurations: the double-layer FSO and the single-layer FSO that has no nitinol wire in the left atrial disk that is made of a polyester patch with a nitinol frame. Only the first configuration was used in this study.
As FSO has thicker diameter nitinol wire as compared with ASO, it requires larger delivery sheaths. Although the device sizes were similar in the two groups, delivery catheter sizes were significantly larger in the FSO group in our study. ASO patients (Group 2) conversely showed significantly less incidence of local hematoma in comparison with Group 1.
In spite of no clinically significant hematoma-related consequence among patients of this study, ASO should thus be preferentially employed in patients with hemorrhagic diathesis.
FSO showed high performance in patients with complex septal anatomy and PFO, showing no difference in immediate and follow-up results when compared with ASO in patients without unfavorable anatomic features. Its conformability allowed overcoming any anatomic complexity without an increase of attempts and/or procedural times. Also in cases with HEV with a limited amount of space between fossa ovalis and Eustachian valve, no trapping of this remnant occurred during the release of the right atrial disk and in no case a repositioning of the device was needed.
In this study no thrombotic immediate or late complication were observed neither in FSO nor in ASO patients. However, FSO has the potential to behave as a more biocompatible device owing to the significant amount of titanium used in its construction whose resistance to the body environment is well known. This is mainly due to its protective oxide films which forms naturally in the presence of even trace amounts of any form of oxygen.
The film is highly adherent, insoluble and chemically nontransportable, preventing reaction with tissue. Furthermore, the modulus of elasticity of titanium participates in the favorable mechanical properties of FSO. In our opinion these characteristics make FSO the device of choice in cases of patients with hemorrhagic diathesis and contra-indication to antiplatelet therapy such as the patient number 9 of this series.
Conclusion
FSO shows high performance in patients with PFO and complex septal anatomy when compared with patients with PFO and uncomplicated atrial anatomy treated using ASO. Its favorable behavior is probably related to fabric features such as the total amount of metal and the presence of titanium.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.