
Abstract
Asthma is a heterogeneous chronic respiratory disease driven by diverse inflammatory pathways that vary across patients. The recognition of distinct molecular endotypes has led to the development of targeted biologic therapies that have transformed the management of moderate-to-severe asthma. However, selecting the most appropriate biologic therapy for each patient remains challenging. Health providers often rely on trial-and-error approaches that may delay disease control, increase costs, and expose patients to unnecessary side effects. Biomarkers are key to precision asthma care, as they provide objective measures of underlying disease mechanisms. Established biomarkers such as blood eosinophil count, fractional exhaled nitric oxide, and serum total immunoglobulin E are important for identifying type 2-high asthma. Sputum biomarkers offer direct insight into airway inflammation, but their use is limited by technical complexity and availability across centers. Emerging biomarkers, including proteomic, transcriptomic, metabolomic, and genomic biomarkers, show promise in further refining biologic therapy selection. In addition, digital biomarkers derived from electronic health records, wearable devices, and artificial intelligence-based algorithms offer new opportunities to capture real-world changes in disease and treatment response. Non-medical drivers of health, particularly socioeconomic factors, are increasingly recognized as modifiers of biologic effectiveness and may also be helpful in selecting biologic therapies. This review summarizes the existing evidence on established and emerging biomarkers used to guide biologic therapy selection in asthma. Integrating multiple biomarkers will be essential to improve biological selection, monitor response, and ultimately achieve the goal of remission in asthma.
Keywords
Introduction
Asthma is a heterogeneous chronic respiratory disease characterized by airway inflammation, hyperresponsiveness, and reversible airflow obstruction. 1 Advances in understanding the pathophysiology of asthma have revealed distinct molecular endotypes, leading to the development of targeted biologic therapies. 2 These therapies focus on modulating key inflammatory pathways, such as those driven by type 2 (T2) inflammation. 3 Identifying biomarkers that accurately capture the various inflammatory types associated with asthma is essential for guiding clinicians in selecting the most effective biologic therapy for each patient. 4 Without suitable biomarkers, clinicians mostly rely on trial-and-error approaches, which can delay effective treatment, increase cost, and expose patients to unnecessary side effects. 5 This review discusses established (Table 1) and emerging biomarkers (Table 2) for guiding biologic therapy in asthma (Figure 1).
Established biomarkers for selecting biologic therapies in asthma.

BEC, blood eosinophil count; FeNO, fractional exhaled nitric oxide; IgE, immunoglobulin E; IL, interleukin; TSLP, thymic stromal lymphopoietin.
Emerging biomarkers for selecting biologic therapies in asthma.
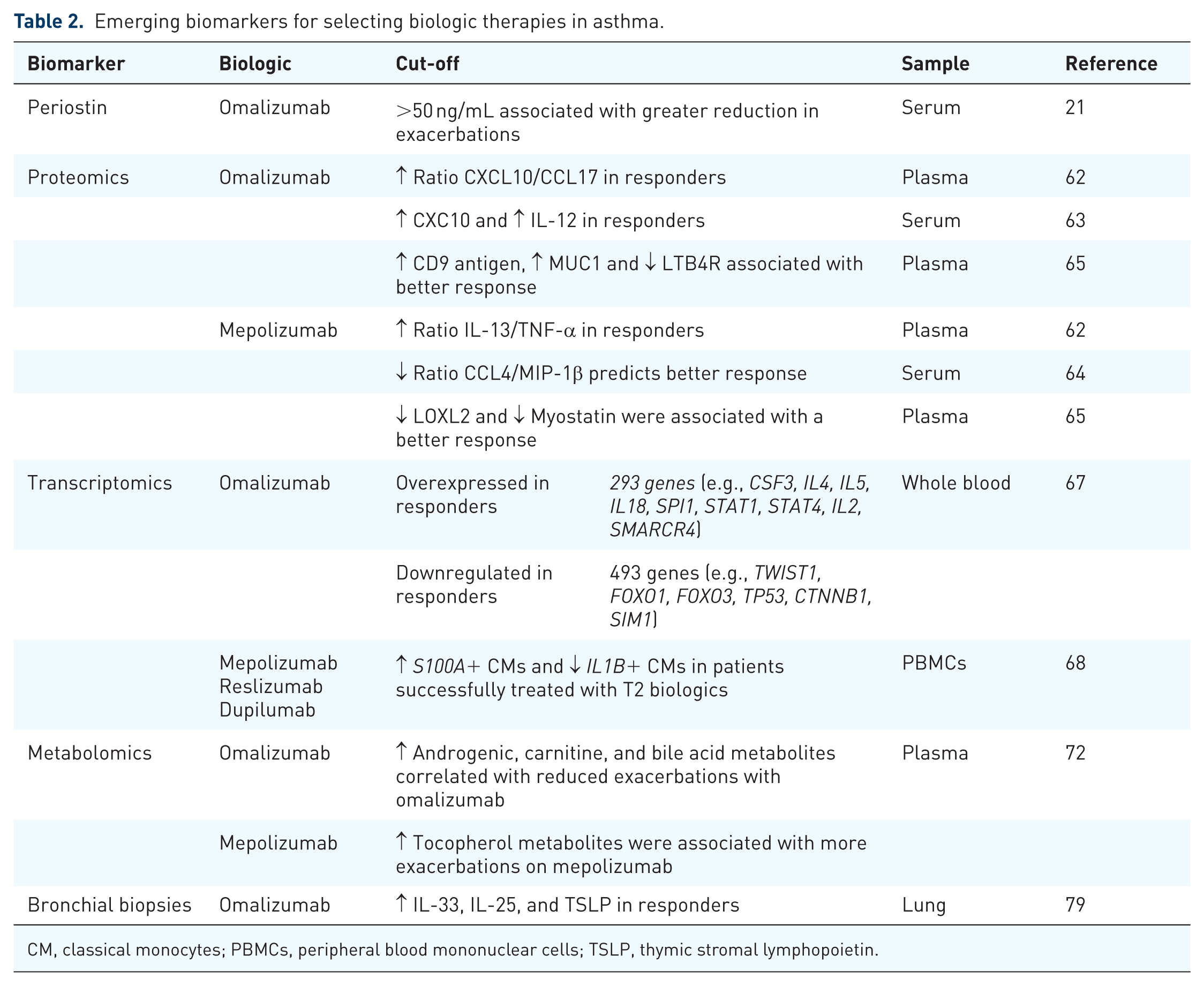
CM, classical monocytes; PBMCs, peripheral blood mononuclear cells; TSLP, thymic stromal lymphopoietin.
Established and emerging biomarkers for guiding biologic treatments in asthma.
Biologics in asthma
There are six biologics currently approved by the Food and Drug Administration for the treatment of asthma: omalizumab, mepolizumab, reslizumab, benralizumab, dupilumab, and tezepelumab. Omalizumab, an anti-immunoglobulin E (IgE) biologic, works by targeting IgE, preventing its binding to receptors on mast cells and basophils, thereby reducing the release of inflammatory mediators triggered by allergens. 6 Anti- interleukin-5 (IL-5) therapies, including mepolizumab, 7 reslizumab, 8 and benralizumab, 9 inhibit IL-5, a key cytokine for eosinophil development, activation, and survival. While mepolizumab and reslizumab block IL-5 itself, benralizumab targets the IL-5 receptor, inducing eosinophil apoptosis through antibody-dependent cellular cytotoxicity. 10 Anti-IL-4/IL-13 therapy, such as dupilumab, blocks the shared receptor subunit for IL-4 and IL-13, cytokines involved in driving IgE production, mucus secretion, airway inflammation, and hyperresponsiveness. 11 Finally, tezepelumab targets thymic stromal lymphopoietin (TSLP), an upstream cytokine that initiates T2 inflammation, thereby preventing the activation of downstream inflammatory pathways involving IL-4, IL-5, and IL-13. 12 In addition to these six FDA-approved biologics, others are currently being investigated in phase II and III clinical trials, including itepekimab (anti-IL-33), astegolimab (anti-ST2 receptor), and lunkesimig, a nanobody that targets both IL-13 and TSLP. 13 Depemokimab, the first ultra-long-acting anti-IL-5 biologic therapy, is also being studied as an alternative to improve patient adherence.14,15 Biomarkers play a crucial role in identifying asthma phenotypes and endotypes, thereby aiding in selecting the most suitable biologic therapy for each patient.
Established biomarkers
Blood eosinophils
Eosinophils are central effector cells in asthma pathogenesis, particularly in the T2-high endotype. 16 Furthermore, elevated eosinophil counts in blood, sputum, and tissue correlate with asthma severity and an increased risk of exacerbation. 17 In clinical practice, a blood eosinophil count (BEC) is commonly used to predict how patients will respond to anti-IgE, anti-IL-5, and anti-IL-4/IL-13 biologic therapies.18–20 Specific BEC cutoffs vary by the type of biologic therapy. Omalizumab demonstrates a greater reduction in exacerbations among patients with a baseline BEC ⩾ 260 cells/µL compared to those with <260 cells/µL. 21 In the case of mepolizumab, secondary analyses of the DREAM and MENSA trials revealed a 52% reduction in exacerbation rates among patients with BEC ⩾ 150 cells/µL, with a greater efficacy observed in those with BEC ⩾ 500 cells/µL. 22 Similarly, patients with uncontrolled asthma treated with reslizumab and a BEC ⩾ 400 cells/µL showed significant improvements in FEV1, FVC, ACG-7 scores, and reduced short-acting beta agonist use compared to those with a BEC cutoff of <400 cells/µL. 23 Although the phase III SIROCCO and CALIMA studies included a BEC cutoff of ⩾300 cells/µL,24,25 benralizumab has also been shown to reduce exacerbations in asthmatics with BECs ⩾ 150 cells/µL. 26 Finally, for dupilumab, the BEC cutoff is ⩾150 cells/µL, but greater efficacy is observed at ⩾300 cells/µL.27,28 In this regard, a recent study using dupilumab for uncontrolled moderate-to-severe asthma evaluated BEC and fractional exhaled nitric oxide (FeNO) as prognostic biomarkers in pediatric patients. Dupilumab showed a more significant effect in subgroups with higher baseline biomarker levels, whereas patients with BEC < 150 cells/μL and FeNO <20 ppb did not experience a significant reduction in exacerbation rates. 19 Tezepelumab is unique among biologics for severe asthma in that it is indicated regardless of baseline BEC. Several studies have shown that tezepelumab reduces the rate of asthma exacerbations and improves lung function in patients with BEC < 150 cells/μL and <300 cells/μL.12,29 In summary, while BEC is the most accessible and used biomarker to select a biologic for asthma, its predictive accuracy is imperfect. Combining BEC with emerging biomarkers may further optimize biologic selection.
Fractional exhaled nitric oxide
In the lungs, nitric oxide (NO) is produced by epithelial cells, vascular endothelial cells, and neurons. 30 Under normal conditions, NO promotes bronchodilation and reduces inflammation. 31 Conversely, T2 inflammation is associated with elevated NO levels, resulting in excess mucus production and bronchial hyperreactivity. The FeNO test quantifies NO levels in exhaled breath and is a surrogate marker for airway inflammation. As a result, the American Thoracic Society recommends using FeNO as an adjunct for diagnosing and managing asthma. 32 FeNO has also been studied as a biomarker for predicting response to biologic therapies in asthma. 33 For omalizumab, patients with baseline FeNO values ⩾19.5 ppb experienced a greater reduction in exacerbations compared to those with FeNO values <19.5 ppb. 21 Interestingly, a study using FeNO testing to screen patients for likely omalizumab response showed that the use of FeNO testing reduced the per-patient cost by almost 50% during the trial and initial treatment periods. 34 Similarly, for dupilumab and tezepelumab, reductions in the frequency of exacerbations have been observed in patients with FeNO values ⩾25 ppb.11,29,35 In contrast, FeNO has proven to be less useful for identifying responders to mepolizumab. 36 In summary, FeNO is a well-established, non-invasive biomarker that helps identify patients with asthma who are likely to benefit from biologic therapies.
Serum total IgE
IgE plays a central role in the pathogenesis of allergic asthma, where allergen-specific IgE, produced during allergic sensitization, binds to mast cells. Upon allergen reexposure, these mast cells degranulate, releasing mediators such as histamine, leukotrienes, and cytokines, which in turn lead to inflammation and airway hyperresponsiveness. 37 A pretreatment total IgE serum level, in conjunction with the patient’s body weight, is used to determine the appropriate dose and dosing frequency of omalizumab for the treatment of allergic asthma. Several studies have also evaluated total IgE serum levels as a predictor of biologic response, particularly in the context of omalizumab use. In one study, which included 25 patients with moderate-to-severe asthma, total IgE serum levels were measured at baseline and 4 weeks after starting omalizumab. A 4-week-to-baseline IgE ratio ⩾2 had a sensitivity and specificity of 100% and 80%, respectively, for predicting treatment response. However, baseline total IgE alone had poor predictive value. 38 Similarly, others found that total IgE serum levels during treatment follow-up, but not at baseline, were associated with the absence of asthma exacerbations during the first year of omalizumab treatment. 39 Overall, these studies suggest that changes in total IgE serum levels after omalizumab initiation may have some predictive value.
Sputum biomarkers
Sputum biomarkers provide a direct measurement of airway inflammation. While sputum biomarkers are well-characterized in research settings, their clinical application remains limited due to technical complexity, a lack of standardization, and restricted availability. However, it remains a valuable tool in expert centers for guiding biologic therapy.
A high sputum eosinophil count (>3% of cells in an induced sputum sample) is a strong predictor of a favorable response for therapies targeting the IL-5/IL-5R pathway, such as mepolizumab and benralizumab. 40 Furthermore, mepolizumab has steroid-sparing effects in patients with sputum eosinophilia and exacerbations despite prednisone treatment.36,41,42 Interestingly, among prednisone-dependent patients with asthma and sputum eosinophils greater than 3%, weight-based reslizumab was superior to mepolizumab in reducing sputum eosinophilia and improving asthma control. 43 Similarly, tezepelumab also showed significant reductions in sputum eosinophils before and after allergen challenge. 44
Sputum neutrophilia is defined as an elevated percentage of neutrophils in sputum. A specific cutoff has not been identified. 45 The presence of sputum neutrophilia has been associated with T2-low asthma, smoking, older age, more severe disease, and corticosteroid resistance.46–48 In addition, sputum neutrophilia identifies patients who are less likely to respond to inhaled corticosteroids and should prompt evaluation for infectious triggers during exacerbations.49,50 Since most biologic therapies target T2 inflammation, they are generally ineffective in this patient group.2,51 Finally, although tezepelumab has shown efficacy in T2-low asthma, its impact on neutrophilic inflammation appears limited. 52
The measurement of sputum cytokines allows the direct identification of the underlying inflammatory endotype. Elevated type 2 cytokines are predictive of response and even remission with anti-IL-5 biologic therapies.40,53 In contrast, persistent elevation of non-T2 cytokines and neutrophil activity in sputum is associated with poor clinical outcomes and biologic treatment failure.51,54
Emerging biomarkers
Periostin
Periostin, encoded by the POSTN gene and regulated by type 2 cytokines such as IL-4 and IL-13, is an extracellular matrix protein belonging to the fasciclin family. 55 Its expression in airway epithelial cells, along with CLCA1 and SERPINB2, distinguishes between T2-low and T2-high asthma.56,57 Since periostin is involved in type 2 inflammation and airway remodeling, 58 it is being studied as a biomarker in the treatment of asthma. For example, in the EXTRA study, patients with high baseline serum periostin levels (>50 ng/mL) showed a 30% decrease in exacerbation rates with omalizumab treatment, compared to 3% in those with low baseline periostin levels (<50 ng/mL). 21 Stratification by periostin level has also been used in clinical trials of lebrikizumab, a humanized monoclonal anti-IL-13 antibody. In one study, the high-periostin subgroup experienced an 8.2% higher increase in FEV1 compared to the placebo group, while the low-periostin subgroup showed a 1.6% increase. 59 However, another study in steroid-naïve asthma patients found no significant FEV1 changes between periostin subgroups. 60 Although periostin has potential as a biomarker for predicting the response to biologic therapy in asthma, additional research is necessary to define its role and standardize its clinical use.
Proteomic biomarkers
Proteomic profiling is emerging as a powerful tool to predict responses to biologic therapies in asthma. 61 For example, proteomic profiling of plasma samples from patients with asthma identified the ratios of CXCL10/CCL17 and IL-13/TNF-α as predictors of response to omalizumab and mepolizumab, respectively. These ratios were more effective at predicting responses to omalizumab and mepolizumab compared to established biomarkers, such as BEC and IgE. 62 Similarly, others have shown that high baseline serum CXCL10 and IL-12 levels predict responsiveness to omalizumab in severe asthma, 63 while a low baseline serum CCL4/MIP-1β level predicts a good response to mepolizumab in severe eosinophilic asthma. 64 An additional study using aptamer-based proteomic profiling showed that lower levels of lysyl oxidase-like protein-2 (LOXL2) and myostatin were associated with better response to mepolizumab. In addition, higher levels of CD9 antigen and MUC1 were associated with a better response to omalizumab, while higher levels of leukotriene B4 receptor 1 (LTB4R) predicted a worse outcome. 65
Transcriptomic biomarkers
Transcriptomic profiling also shows promise as a tool for predicting the response to biologic therapies in asthma. 66 For example, one study analyzed whole blood transcriptomes of patients with moderate-to-severe asthma treated with omalizumab. 67 Responders exhibited sustained changes in gene expression, shifting their profiles closer to those of healthy controls, whereas non-responders retained a pro-inflammatory signature, particularly with persistent upregulation of genes related to neutrophils and eosinophils. 67 In responders, 293 genes were overexpressed, including those linked to Th2 (CSF3, IL4, IL5, IL18, SPI1) and Th1 (STAT1, STAT4, IL2, SMARCR4) responses. Meanwhile, 493 genes were downregulated, including those associated with inflammation (TWIST1, FOXO1, FOXO3, TP53, CTNNB1, SIM1). 67 A separate study using single-cell RNA sequencing of peripheral blood mononuclear cells (PBMCs) from severe asthma patients before and after treatment with mepolizumab, reslizumab, or dupilumab found changes in classical monocyte (CM) composition. 68 Specifically, there was a reduction in IL1B+ CMs and an increase in S100A+ CMs. There was also significant suppression of the NF-kB pathway across multiple immune cells, including T, B, NK, and myeloid cells. 68 Additional studies are needed to determine the scientific significance and clinical utility of these biomarkers in the selection of treatment and in assessing response.
Metabolomic biomarkers
Metabolomics biomarkers can also identify distinct asthma phenotypes and endotypes, thereby aiding in the selection of the optimal biologic therapy. 69 For example, untargeted metabolomic profiling identified five distinct metabolic endotypes within a Costa Rican asthma cohort, with cholesterol esters, triglycerides, and fatty acids emerging as the most significant drivers of these metabolic endotypes. 70 Another study using metabolic profiling identified 17 steroid metabolites significantly reduced in asthma patients, particularly those using inhaled corticosteroids (ICS), suggesting potential adrenal suppression. 71 These patients with ICS-induced adrenal suppression might benefit from more targeted therapy using biologics. Also, metabolomic analysis has identified biomarkers predictive of response to omalizumab and mepolizumab. 72 Nopsopon et al. 72 found that elevated levels of androgenic, carnitine, and bile acid metabolites correlated with reduced exacerbations on omalizumab, while tocopherol metabolites were associated with increased exacerbations on mepolizumab. Similarly, plasma lipid biomarkers have been linked to a ⩾50% reduction in exacerbations with omalizumab in other studies. 73
Digital biomarkers
Digital biomarkers, derived from data collected through electronic health records (EHRs), wearable devices, sensors, and artificial intelligence (AI)–based algorithms, represent a novel category of biomarkers that extend beyond traditional molecular measures.74–76 Unlike blood-based or tissue biomarkers, digital biomarkers capture dynamic, real-world physiological and behavioral patterns, offering unique insights into disease heterogeneity and treatment response. For example, natural language processing (NLP) enables the extraction of clinically relevant data from unstructured EHRs.76,77 In our prior work, we demonstrated that distinct subgroups of asthma can be identified using multiple NLP algorithms based on different asthma criteria. These subgroups exhibited markedly different clinical and immunological profiles, suggesting that algorithmically derived phenotypes may function as “digital biomarkers” for biologic therapy response.56,76 Similarly, wearable technologies and remote monitoring tools can capture longitudinal data on respiratory rate, nocturnal cough, activity levels, and medication adherence, which may serve as early predictors of the effectiveness of biologic therapy or loss of response. 75 By integrating multi-modal data streams, including clinical, molecular, and environmental exposures, digital biomarkers can provide a holistic view of asthma pathophysiology and therapeutic response. While these technologies are still in the early stages of validation, their incorporation into precision medicine frameworks has the potential to transform the selection and monitoring of biologic therapies in asthma care.
Other biomarkers
Other biomarkers are being considered for predicting the response to biologic therapy in asthma, including bronchial biopsies. Bronchial biopsies can provide a direct assessment not only of airway inflammation, but also of epithelial remodeling. 78 Bronchial biopsies of omalizumab responders show decreased IL-33, IL-25, and TSLP. 79 Anti-IL-5 therapy is associated with decreased airway eosinophils, sub-basement membrane thickness, and smooth muscle cell area.80–83 In contrast, there is persistence of endobronchial eosinophils in patients treated with dupilumab. 78 Finally, tezepelumab therapy is associated with a decrease in bronchial eosinophils and mast cells. 84
Several studies are exploring single-nucleotide polymorphisms (SNPs) as genomic biomarkers for selecting biologic therapies. In this regard, a study involving patients with uncontrolled eosinophilic asthma found that reduced exacerbations with mepolizumab were linked to ZNF415 rs1054485-T, while reductions with benralizumab were associated with ZNF415 rs1054485-T and FCER1B rs569108-AA. 85 Additionally, microRNAs (miRNAs), small non-coding RNA molecules, have also been investigated in this context. MiRNAs such as the let-7 family, miR-193b, miR-375, miR-21, miR-223, miR-146a, miR-142-5p, miR-142-3p, miR-146b, and miR-155 play critical roles in asthma pathogenesis and are associated with disease phenotypes and severity, suggesting their potential as biomarkers for treatment response. 86
In addition to molecular markers, non-medical drivers of health (NMDOH) are increasingly recognized as critical determinants of asthma outcomes.87,88 Socioeconomic status (SES) is a well-established NMDOH that significantly impacts asthma outcomes. Lower SES has been consistently associated with increased asthma prevalence, greater disease severity, poorer symptom control, higher healthcare utilization, and reduced access to guideline-based care, including biologic therapies.89–92 Although evidence directly connecting SES to biologic therapy response remains limited, several mechanisms suggest SES may influence treatment effectiveness. Patients with lower SES often experience greater environmental exposures (e.g., allergens, pollutants, and infections) and reduced adherence to controller medications, which may affect biologic treatment response.93–96 Barriers such as fragmented follow-up, insurance coverage, and medication access disproportionately affect low-SES populations, potentially leading to interrupted biologic use and suboptimal outcomes. Despite its recognized importance, SES is often difficult to measure accurately and consistently in clinical and research settings. Traditional measures, such as income or education, are frequently unavailable or imprecise.
The HOUsing-based SocioEconomic Status (HOUSES) index is a novel, validated, individual-level SES measure derived from publicly available housing property data linked to patient addresses.97,98 Unlike traditional SES measures that rely on self-reported income or area-level data, the HOUSES index provides a scalable and objective proxy for household-level SES. Studies have demonstrated its strong association with a wide range of health outcomes, including asthma prevalence and control.89,92,99 The HOUSES index, by providing an objective, scalable, individual-level SES measure, could serve as a practical tool to identify patients at risk of poor biologic therapy response due to these contextual factors. While a specific HOUSES threshold would not currently dictate initiation of a biologic therapy, incorporating HOUSES alongside clinical and molecular biomarkers may allow clinicians to anticipate challenges with treatment adherence, identify subgroups requiring additional care coordination, and design interventions to optimize medication effectiveness. Future studies explicitly evaluating SES, including HOUSES, as a predictor or effect modifier of biologic response will be essential to determine its clinical utility in precision asthma care.
Finally, radiomic analysis shows promise for asthma phenotyping but is not currently used to guide biologic therapy selection in clinical practice. Imaging-derived biomarkers, including airway dimensions, mucus burden, and the extent of air trapping, are increasingly incorporated as endpoints in clinical trials. 100 Further validation is needed to determine whether radiomic approaches provide additional value over other strategies for selecting biologic therapies.
Challenges and limitations
Biomarker overlap among T2-targeting therapies poses challenges for patient selection, as markers such as BEC and FeNO are elevated across multiple T2 asthma endotypes, thereby reducing their specificity. Several studies included in this review do not identify biomarkers that directly predict response to specific biologic therapies; rather, they inform treatment decisions by characterizing disease severity, treatment-related risks, or relevant comorbid conditions. Moreover, biomarker levels are dynamic and can fluctuate due to disease activity, comorbidities, and corticosteroid use, underscoring the need for enhanced biomarkers that enable longitudinal monitoring and precise characterization of disease phenotypes. In this regard, AI tools will play a key role in integrating multiple biomarkers over time. As the role of biologics in inducing asthma remission expands, future studies should also focus on identifying biomarkers to determine when to stop or resume a specific biologic therapy. 101 Another significant unmet need exists for validated biomarkers in T2-low asthma, with ongoing efforts to elucidate underlying mechanisms and identify specific therapeutic targets. 102 Furthermore, the cost and accessibility of biomarker assays limit their widespread adoption, underscoring the importance of simplifying testing protocols and reducing costs to ensure better access.
Conclusion
Biomarkers play an important role in selecting biologic therapies for asthma by identifying patients most likely to benefit and minimizing unnecessary treatment. While established biomarkers, such as BEC, FeNO, and IgE, have revolutionized the management of T2-high asthma, emerging biomarkers offer exciting opportunities to further refine patient stratification. Addressing the challenges posed by biomarker variability, accessibility, and T2-low asthma will be critical to advancing precision medicine in asthma care. As research advances, integrating a comprehensive panel of biomarkers, including traditional biomarkers, multi-omics data, digital biomarkers, and bioimaging, will improve biologic selection and enable asthma treatment plans tailored to individual pathobiology. This strategy aligns with the principles of precision medicine in asthma and is essential for achieving sustained disease control and, ultimately, remission.