
Abstract
What we already know
• The prevalence of asthma in Chinese adults increased with age and the older asthma patients frequently exhibit unusual symptoms and have several comorbidities, resulting in higher mortality. • Obesity is a major global public health issue connected with aging and people with BMI of higher than 25 kg/m2 had a 1.51-fold greater risk of developing asthma compared to normal-weight patients.
What this article adds
• This retrospective study focused on the influence of the two major public health problems, obesity and population aging to asthma. The senior Chinese Han asthmatics with overweight/obesity had a lower FeNO level compared to those without obesity. • FeNO level was inversely correlated with PC20 in elderly asthma patients. These findings may aid in understanding and optimizing the management of asthma in the elderly.
Introduction
Asthma, although often seen as a pediatric issue, is increasingly prevalent in the elderly, reaching a peak of 7.4% in those aged 70 and above according to the 2019 China Pulmonary Health (CPH) study. 1 Aging-related changes in immunity and respiratory physiology make elderly asthma patients more prone to erratic symptoms, numerous comorbidities, and increased mortality.2–5 Obesity, another significant concern linked with aging, considerably influences asthma occurrence and manifestations. 6 Globally acknowledged as a distinct asthma phenotype, obesity-linked asthma can increase the patient’s risk by 1.51-fold over normal-weight individuals.7,8 Numerous studies explore obesity’s role in childhood asthma.9,10 Yet, the impact of obesity on elderly asthma remains widely unknown.
Our research delves into this underexplored area, focusing on the presumably non-allergic mechanisms of obesity-induced asthma in the elderly. 11 Evidence suggests that obesity is primarily associated with non-atopic asthma in adults,3,4 and fractional exhaled nitric oxide (FeNO) measurement is an established marker of eosinophilic airway inflammation.12,13 However, the obesity-asthma nexus, via non-eosinophilic airway inflammation in the elderly, is mostly unclear. Hence, our research aims to investigate the influence of overweight/obesity status on airway inflammatory markers and airway responsiveness in elderly asthma patients. This study promises to deepen our understanding of obesity-driven asthma in the aging population by shedding light on its potential mechanisms.
Methods
Study design and participants
This retrospective study was conducted at an academic teaching hospital, the First Affiliated Hospital of Sun Yat-sen University, recruiting Chinese Han patients over 65 years old with asthma from December 2015 to June 2020. This study identified participants based on the following criteria: (1) patient aged ≥65 years old with newly diagnosed bronchial asthma based on the Global Initiative for Asthma definition; 7 (2) patient who underwent bronchial provocation test (BPT) or bronchial dilation test (BDT) and FeNO without any oral or inhaled corticosteroids and bronchodilators in the last 72h and without respiratory tract infection within 8 weeks. (4) nonsmokers or former smokers who have quit smoking. Patients were excluded for congestive heart failure classes III and IV, lung resection history, dementia, immunodeficiency disorders, COPD, lung cancer, bronchiectasis, and interstitial lung disease. COPD was excluded based on the available data; if it was not determined, the patient was also excluded.
The primary objective of this study was assessing the influence of overweight/obesity on lung function and FeNO in newly diagnosed elderly Chinese Han asthma patients. The secondary objective explored the relationship between overweight/obesity and airway responsiveness. The Institutional Research Ethics Committee of the First Affiliated Hospital of Sun Yat-sen University approved the study (Approval number:2021071), and the institutional review board waived informed consent due to the study’s retrospective nature.
Demographics, medical and smoking history, prescription information, pulmonary function test (PFT), and FeNO were extracted from patient files using a standardized form. The technician determined BMI by dividing weight (in kilos) by the square of height (in meters). Overweight and obesity were evaluated according to the Guidelines for Prevention and Control of Overweight and Obesity in Chinese Adults, 14 dividing patients into two groups based on BMI: overweight/obesity (BMI ≥ 24 kg/m2) and non-obesity (BMI < 24 kg/m2).
Measurements of pulmonary function and FeNO
PFT was performed using Medisoft and flow–volume curves were obtained in accordance with the 2014 recommendations of the Chinese National Guidelines of Pulmonary Function Test. 15 PFT was performed by trained staff in a reproducible manner. Best scores were selected from each subject’s acceptable tests. Forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), FEV1/FVC, forced expiratory flow at 25%, 50%, and 75% of FVC (MEF25%–75%), peak expiratory flow (PEF), maximum voluntary ventilation (MVV), and vital capacity (VC) were determined.
Patients with a FEV1% ≧70% underwent BPT and those with a FEV1% <70% underwent BDT. BPT was conducted in accordance with internationally standardized guidelines. 16 PFT values were assessed prior to histamine challenge. Airway hyperresponsiveness (AHR) is expressed as the provocative concentration of histamine when FEV1 decreased by 20% from baseline (PC20). In our study, the positive response was defined as PC20 ≦ 8 mg/mL. In order to investigate the relationship between BMI and airway responsiveness, we pre-defined high and low AHR for the BPT patients. Cutoff for high AHR was PC20 ≦ 1 mg/mL, whereas low AHR was PC20 > 1 mg/mL but ≦8 mg/mL. 17 BDT was performed between 15 and 20 min after inhaling 400 μg of salbutamol from a spacer-equipped metered-dose inhaler, and a positive response defined as a FEV1 increase of ≧200 mL and ≧12% improvement. 15 FeNO was measured using an electrochemical analyzer (NIOX MINO Analytical Instruments, Aerocrine AB, Solna, Sweden) before PFT following American Thoracic Society/European Respiratory Society recommendations. 16
Statistical analysis
Jamovi 2.3 was used for statistical analysis.18,19 Continuous variables expression used mean ± standard deviation. Using the Shapiro–Wilk normality test, the normality of all continuous variables was determined. Unmatched pair of tails Student's t-tests were used for regular distributions and the Mann–Whitney U test for others. Categorical data underwent the Chi-square test. 20 After a log10 transformation, FeNO data passed the normality test despite their skewed character. Association between FeNO and age, BMI and PC20 underwent a multiple linear regression model using a log transformation of FeNO. 21 Two-tailed p values of 0.05 were deemed statistically significant. GraphPad Prism 8.4 generated all graphs (GRAPH PAD software Inc, California, USA).
Results
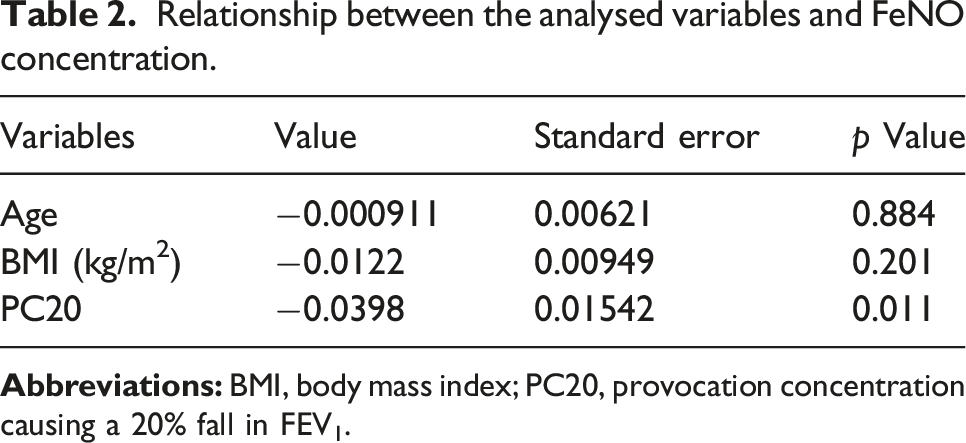
1. This study initially identified 153 newly diagnosed asthma patients who met the inclusion criteria. However, 17 cases were excluded due to missing clinical data, insufficient glucocorticoid withdrawal time, and the presence of exclusionary comorbidities. Consequently, 136 patients were enrolled. The sample comprised 70 males and 66 females, with a mean age of 71.2 ± 5.40 years and a mean BMI of 23.8 ± 3.63. The overall average FeNO concentration was 42.3 ± 38.4 ppb. Table 1 delineates the study population’s clinical characteristics. 2. The study subdivided its population into 66 overweight/obese patients and 70 non-obese patients. There were no significant differences between these two groups regarding age and sex. However, they did differ significantly in terms of height, weight, body surface area, and BMI. Predicted FVC and FEV1 percentages were marginally higher in the overweight/obese group, representing a significant difference. And the mean FeNO value in the overweight/obese group (35.4 ± 31.4 ppb) was significantly lower than that in the non-obese group (48.8 ± 43.1ppb; p < .05) (see Table 1 and Supplemental Figure 1). 3. In this study, 96 patients underwent the BPT test. Among those in the overweight/obesity group, 19 patients had a PC20 ≤ 1 mg/mL and 36 had a PC20 > 1 mg/mL but ≦8 mg/mL. For the non-obesity group, 14 patients had a PC20 ≤ 1 mg/mL and 27 had a PC20 > 1 mg/mL but ≦8 mg/mL. The comparison of high AHR and low AHR proportions between the overweight/obesity and non-obesity groups revealed no statistically significant difference via the chi-square test (p > .05) (see Supplemental Figure 2). 4. Multiple linear regression analysis further examined the correlation between log transformation of FeNO and age, BMI and PC20. The model provided an R of 0.289 with a p value of 0.045. This model affirmed significant relationships between log transformation of FeNO level with PC20 (p < .05) (see Table 2 and Figure 1). However, age and BMI did not significantly relate to the FeNO level (p > .05). Clinical characteristics of elderly patients with asthma. ap value by chi-square test. bp value by unpaired two-tailed Student’s t-tests. cp value by Mann–Whitney U test. Relationship between the analysed variables and FeNO concentration. Scatter plot of age(a), BMI(b), PC20(c) and log transformation of FeNO. Abbreviations: BMI, body mass index; PC20, provocation concentration causing a 20% fall in FEV1; FeNO, fractional exhaled nitric oxide; ppb, parts per billion.


Discussion
Obesity and population aging, as generally accepted, represent significant public health challenges in the contemporary era. Nonetheless, the research exploring the association between obesity and asthma in the aging populace remains limited. We conducted this study to further our understanding of the implications of overweight and obesity on the alterations of pulmonary function and airway inflammation in elderly asthmatics, specifically focusing on lung function, FeNO, and airway hyperresponsiveness.
Epidemiological data suggest a higher prevalence of adult asthma among women. This notion is supported by recent findings from Shah R et al 22 and Park S et al, 23 which indicate a higher incidence of obesity-induced asthma in elderly women. In contrast, our experiment, which primarily focused on the Chinese Han population, found no significant differences between the non-obese and overweight/obese cohorts. This discrepancy could be attributed to differences in sample population and the inclusion of overweight and obese patients in our study.
It is observable that significant fat accumulation in the thoracic and abdominal cavities could potentially compress lungs, thereby reducing lung volume. 24 A prevalent theory among experts suggests that adult obesity leads to diminished lung function. This is further corroborated by earlier studies highlighting decreased functional residual capacity (FRC) and expiratory reserve volume (ERV) in obese patients.25–27 However, our results displayed no significant differences in PEF, MEF, MEF25, MEF50, MEF75, MVV, and VC between non-obese and overweight/obese subjects. Notably, our study found slight increases in FVC and FEV1 in the overweight/obese group. We attribute these intriguing deviations to the inclusion of overweight individuals in the sample and the potentially attenuated impact of obesity on lung function. Regrettably, due to the undesirable scarcity of instances assessing FRC and ERV, our research could not evaluate these vital indices.
The correlation between FeNO levels and elderly asthmatics remains a topic of contention. Our findings showed elevated FeNO levels (42.3 ± 38.4 ppb) in elderly asthma patients, congruent with the findings from Hiroyuki Sano’s study reporting the FeNO concentration as 40.0 ± 38.8 ppb. 28 Contrarily, Smith AM et al. found no increased FeNO levels in elderly asthmatics with only 20 ppb, but half of their cohort receiving treatment with inhaled corticosteroids. 29 FeNO, a notable indicator of eosinophilic airway inflammation, correlates with asthma’s inflammatory severity. Although a plethora of inflammatory phenotypes exist in asthma, some studies have identified a connection between FeNO and the Th2 immune response. Our analysis suggested FeNO levels in overweight/obese senior asthmatic patients were elevated, but lower than that in non-obese elderly asthmatic patients, which indicated that eosinophilic airway inflammation might not predominate in these patients. This aligns with findings from Scott HA’s study, which portrayed a profile of obese patients with neutrophilic airway inflammation. 30
Our study found a comparable prevalence of high AHR among patients in both the overweight/obesity and non-obesity groups, suggesting that overweight/obesity may have negligible influence on AHR. Previous studies reporting on the relationship between BMI and hyperresponsiveness have presented varied findings, with some noting no relationship and others indicating a potential association. 31 However, a large-scale prospective longitudinal cohort study by Litonjua AA et al., encompassing more than 7000 adults, demonstrated an increased risk of AHR with escalating BMI and identified weight gain as a risk factor for AHR development. 32 In our investigation, we observed an inverse correlation between the log-transformed measures of FeNO and PC20. But age and BMI did not significantly relate to the FeNO level., which might indicate that the level of FeNO was influenced majorly by the AHR but not the age or BMI. AHR in older patients may likely be modulated by a non-Th2 immune response. Concurrently, animal studies disclosed that several adipose-originating inflammation-inducing molecules like Tumor Necrosis Factor-alpha (TNF-α), leptin, and adiponectin can trigger AHR, potentially contributing to obesity-related asthma development. 33 This suggests that obesity-induced AHR could be modulated through non-allergic mechanisms in a mouse model. 11
Based on the comprehensive review by Dunn RM, 34 two phenotypes of asthma exist in the elderly: late-onset and persistent asthma, each showcasing distinct immunological responses. Moreover, the age-dependent alterations in eosinophil quantity and function in elderly asthmatics remain poorly understood, adding complexity to their mechanisms and signaling the need for further exploration.
This study, being retrospective in nature, is not exempt from inherent limitations. Primarily, given its single-center frame and limited patients included, there exists a potential for collection bias. Furthermore, access to limited data prevented us from exploring various lung function indices. As previously mentioned, two distinct phenotypes are recognized based on the age of onset. However, our retrospective study design hindered precise phenotype identification in our patients. Despite these constraints, our study, to our knowledge, is the inaugural exploration of the association between obesity and asthma within the elderly Chinese Han population. Consequently, this research may help spotlight this phenotypic category and advance our understanding of obese asthma in the aging populace.
Conclusion
In conclusion, our study reveals that overweight or obese elderly Han Chinese individuals with asthma exhibit lower FeNO levels compared to those without obesity. Additionally, we observed an inverse correlation between FeNO levels and PC20 in elderly asthma patients. These significant findings contribute to a better understanding of asthma management in the elderly population and offer insights for optimizing their treatment strategies.
Supplemental Material
Supplemental Material - Effect of overweight/obesity on relationship between fractional exhaled nitric oxide and airway hyperresponsiveness in Chinese elderly patients with asthma
Supplemental Material for Effect of overweight/obesity on relationship between fractional exhaled nitric oxide and airway hyperresponsiveness in Chinese elderly patients with asthma by Fengjia Chen, Yangli Liu, Long-hua Sun, Zhimin Zeng, and Xinyan Huang in International Journal of Immunopathology and Pharmacology
Footnotes
Author contributions
FJC and YLL: collected data and wrote of the original draft. ZMZ: edited the draft and statistical analysis. LHS: discussed and reviewed the draft. XYH: reviewed and edited the draft.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Guangdong Provincial Medical Science and Technology Research Fund project(C2023044), National Natural Science Foundation of China (82200029), National Natural Science Foundation of China (82100054), National Natural Science Foundation of China (82300027) and National Natural Science Foundation of Jiangxi province (20202BAB206043).
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.