
Abstract
Background:
Nontuberculous mycobacterial pulmonary disease (NTM-PD) is a chronic lung infection associated with persistent respiratory symptoms and diminished health-related quality of life (HRQoL). As with other chronic conditions, increased levels of anxiety and depression can impact prognosis and HRQoL.
Objectives:
To describe the prevalence of anxiety and depression and to identify HRQoL domains that are correlated with mental health in patients with NTM-PD.
Design:
A cross-sectional observational study of adults with self-reported or clinically confirmed NTM-PD.
Methods:
Participants with NTM-PD enrolled in two studies (n = 40 interview + surveys and n = 230 completing electronic surveys only) at four U.S. sites. Inclusion criteria were age >18 years, English-speaking, and U.S. residence. In-person enrolled participants met ATS/IDSA criteria and had symptom documentation in medical records; remotely enrolled participants self-reported NTM-PD and symptoms. Data collected included demographics, GAD-7 and PHQ-8 (anxiety and depression screening, respectively), QOL-B Respiratory Symptoms Scale (RSS), selected PROMIS short forms (Fatigue 7a, Cognitive Function 6a, Sleep Disturbance 4a), and Patient Global Impression of Severity of NTM-PD symptoms (PGIS). Interview-only participants completed the GAD-7, PHQ-8, QOL-B RSS, and were evaluated for cognitive functioning using the computerized Symbol Digit Modalities Test (oral version).
Results:
The study population was predominantly female (57%/91% in the interview/survey studies, respectively) and aged >65 years (50%/77.4%). Overall, 18%/14% screened positive for anxiety and 32%/18% for depression. Participants screening positive for anxiety or depression had significantly lower QOL-B RSS, cognitive function, and sleep scores, and higher fatigue. Fatigue showed the strongest correlation with mental health outcomes, particularly with those screening positive for depression (ρ = 0.644, p < 0.05).
Conclusion:
Mental health symptoms are strongly correlated with worse HRQoL outcomes in NTM-PD. These findings underscore the need for the implementation of routine mental health screening and interventions in NTM-PD care.
Introduction
Nontuberculous mycobacteria (NTM), predominantly Mycobacterium avium complex (MAC), cause chronic, debilitating pulmonary disease (NTM-PD).1–3 Common symptoms include persistent cough, dyspnea, fatigue, night sweats, weight loss, depression, social anxiety, and hemoptysis. Additionally, patients report a significant decline in overall health, decreased physical activity levels, and increased social isolation due to MAC disease. 4 These symptoms can significantly impact the patient’s overall daily functioning, as well as their health-related quality of life (HRQoL) across physical, social, mental, and energy domains.5–9 In addition, the decision to initiate long-term multidrug antimycobacterial treatment is based on many factors, including patient quality of life, desire for therapy, willingness to tolerate potential drug side-effects, and shared decision-making between patients and physicians regarding balancing the risks of long-term treatment with the potential benefits of therapy.
A key component of patient-focused research is the use of patient-reported outcomes (PROs), which are defined as any outcome reported directly by patients themselves, including health status assessment, HRQoL, and symptoms. Given that improvements in daily symptoms and functioning are critical measures of treatment success, a better understanding of how chronic NTM-PD impacts patients is essential.
According to the World Health Organization’s report on mental health, 5% of the general adult population experiences depression, while 4.8% experiences anxiety. 10 These mental health conditions are found to be more prevalent in patients with chronic respiratory disease than those without.11–14 Integrated approaches beyond antibiotic treatment have been emphasized for treating NTM-PD, including improvement of HRQoL by reducing the impact of anxiety and depression in patients with NTM-PD.15,16 There are few published data regarding the prevalence of anxiety and depression in patients with NTM-PD, including factors associated with these mental health symptoms/conditions and their subsequent clinical implications. 17 Therefore, it is important to develop an understanding of the factors that contribute to HRQoL impairment in this population.
For this study, our primary objectives were to describe the prevalence of anxiety and depression by using the Generalized Anxiety Disorder (GAD-7) assessment 18 and Patient Health Questionnaire (PHQ-8) depression scale 19 and to identify HRQoL domains that are correlated with mental health in patients with NTM-PD.
Methods
This study presents data collected from two NTM-PD populations: 40 patients interviewed as part of a qualitative concept elicitation interview study and 230 patients recruited to represent NTM-PD across species (e.g., M. avium complex, M. abscessus) in a psychometric study. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 20 The checklist from STROBE is provided in the Supplemental Material.
Interview study
The concept elicitation study was designed to identify key symptoms and their impact on functioning in people with NTM-PD 21 (results not reported here, manuscript in development). Adults with NTM-PD were recruited from four clinical sites across the United States between April and November 2022: National Jewish Health (Denver, CO), Medical University of South Carolina (Charleston, SC), Oregon Health & Science University (Portland, OR), and University of Texas Health Science Center (Tyler, TX). Eligible patients were at least 18 years of age, English-speaking, and met ATS/IDSA disease criteria for NTM-PD. 1 Based on clinician expert discussions, patients with cystic fibrosis (CF) were excluded due to having a different symptom profile and treatment burden. Recruitment targets were set for less commonly encountered characteristics, including race/ethnicity other than White, male sex, cavitary disease, age <50, infections with M. abscessus species, and without underlying bronchiectasis.
After the interview, a computerized Symbol Digit Modalities Test (SDMT, oral version, available from Western Psychological Services) was administered by a licensed clinical psychologist (ALQ) to 30 out of the 40 participants to assess cognitive functioning, including attention, processing speed, and short-term working memory.22–24 Patients also completed the following PRO measures electronically via REDCap: GAD-7/PHQ-8, QOL-Bronchiectasis with NTM Module (V3.1), and a global impression of NTM or MAC disease severity (PGIS).18,19,25–28 Retrospective chart review was conducted to collect the most recent NTM culture data, comorbidities, and treatment history.
Psychometric study
Separate recruitment for a psychometric study took place between July and September 2024 in-person at the same four sites as the interview study, and remotely via targeted invitations emailed to patients with NTM-PD through the NTM Info & Research (NTMir) listserv. Eligible patients were at least 18 years of age, English-speaking, and living in the United States. Those enrolled in-person also met ATS/IDSA disease criteria 1 for NTM-PD and had symptoms documented in their medical record. Participants who were enrolled remotely self-reported both NTM lung disease and associated symptoms. We did not explicitly exclude those who had previously participated in the interview study, due to the fact that it was completed 2 years prior.
All patients completed self-reported age, gender, education, income, and race/ethnicity, and were screened for anxiety/depression using the GAD-7/PHQ-8 instruments. Patients recruited through NTMir (n = 139) self-reported treatment status (currently on treatment, previously treated, or never treated), chronic obstructive pulmonary disease (COPD), and other diagnoses that impact their daily lives. Due to a database error, NTM species and bronchiectasis were not captured. For those enrolled in-person (n = 91), additional chart review confirmed NTM species, treatment status, COPD, bronchiectasis, and other relevant underlying disease. All patients completed the NTM-SS instrument in addition to GAD-7/PHQ-8, QOL-B, and NTM Symptoms Module, selected patient-reported outcomes measurement information system (PROMIS) scales (SF Fatigue 7a, 29 SF Cognitive Function 6a, 30 Sleep Disturbance 4a 31 ), and PGIS, 28 administered electronically via REDCap.
Surveys conducted
GAD-7: The GAD-7 is a validated, 7-item anxiety screening measure for Generalized Anxiety Disorder (GAD). 18 Total scores range from 0 to 21. A score of 10 or greater represents a positive anxiety screening threshold, with cut points of 5, 10, and 15 interpreted as mild, moderate, and severe levels of anxiety. The seven questions from this self-administered questionnaire are designed to map onto the DSM-5 diagnostic criteria for GAD.
PHQ-8: The PHQ-8 is a validated depression diagnostic and severity tool. 19 An 8-item version of the Patient Health Questionnaire (PHQ) depression scale generates a score ranging from 0 to 24. A score of 10 or greater represents a screening threshold for clinically significant depression, with scores between 0–4, 5–9, 10–14, 15–19, and 20–24, representing none, mild, moderate, moderately severe, and severe depressive symptoms, respectively. It includes eight of the nine symptoms used in the DSM-5 for diagnosing major depressive disorder and is designed to map onto the DSM-5 diagnostic criteria.
QOL-B: The Quality of Life-Bronchiectasis (QOL-B) is a validated PRO measure that assesses symptoms, functioning, and HRQoL, developed for people with bronchiectasis without CF. 26 It includes 37 items on 8 separate scales (Respiratory Symptoms, Physical, Role, Emotional and Social Functioning, Vitality, Health Perceptions, and Treatment Burden). The eight scales are scored separately and standardized on a 0–100-point scale, with higher scores representing fewer symptoms or better functioning and HRQoL.
PGIS: The patient global impression of severity is a single-item patient-reported outcome measure aimed at capturing symptom severity or change. 36 Patients were asked to rate the severity of MAC disease symptoms on a 5-level scale scored 0–4 (0 = none, 1 = mild, 2 = moderate, 3 = severe, 4 = very severe).
PROMIS: The PROMIS item bank and validated measures evaluate and monitor physical, mental, and social health. Three short forms were utilized in the psychometric study: SF Fatigue 7a, 29 SF Cognitive Function 6a, 30 and Sleep Disturbance 4a. 31 The PROMIS Fatigue SF is a 7-item questionnaire that assesses both the experience of fatigue and the interference of fatigue on daily activities over the past week. The PROMIS Cognitive Function SF is a 6-item scale that assesses patient-perceived cognitive deficits. The PROMIS Sleep Disturbance SF is a 4-item questionnaire that evaluates the severity of sleep disturbances over the past 7 days. All PROMIS scores are converted to a T-score metric (mean = 50, SD = 10) with a higher T-score representing more of the concept being measured. For negatively worded concepts such as fatigue, a higher T-score represents greater fatigue, and a lower T-score represents less fatigue. For positively worded concepts such as cognitive function, a higher T-score reflects better cognitive function.
NTM Module: A validated PRO measure for patients with pulmonary NTM disease. 27 It generates four domain scores from 0 to 100, with higher scores indicating better functioning, reflecting NTM-specific symptoms (NTM symptoms, Body Image, Digestive Symptoms, and Eating Problems). Responses are measured using a 4-point Likert scale (“a lot,” “a moderate amount,” “a little,” or “not at all”).
Mental health definitions
We defined screening positive using standard cutoffs of 10 for GAD-7 18 and PHQ-8 19 scores, identifying moderate or clinically elevated anxiety or depression, respectively, with follow-up diagnostic evaluation indicated. Each analysis was repeated using a threshold of five to include patients who reported mild symptoms. Examining mild symptoms of anxiety and depression is crucial in evaluating HRQoL, as these symptoms—despite not reaching diagnostic thresholds—often represent the early stages of mental health conditions and, if left unaddressed, have a well-documented32,33 potential to escalate into moderate or severe symptoms. Their inclusion in HRQoL assessments supports early intervention and prevention efforts. For the outcome examining patients who screened positive for both anxiety and depression, two different comparisons were evaluated: patients screening positive for both anxiety and depression versus (1) all other patients (negative for either) and (2) patients negative for both, that is, excluding participants who screened positive for anxiety or depression but not both.
Statistical methods
Descriptive statistics were reported as percentages for categorical variables and as means and standard deviations for quantitative variables. The mean scores (SE) for QOL-B RSS and PROMIS scales were compared by group for each mental health outcome as previously defined. Normality of distributions was evaluated using the Shapiro–Wilks tests, and subgroup comparisons were made using t-tests or the Mann–Whitney test. The strength of association between variables was assessed using Pearson or Spearman rank correlations, as appropriate. All analyses were conducted using SAS version 9.4 software (SAS Institute, Cary, NC, USA).
Results
Interview study
The Open-Ended Patient Interview Study included 40 adult patients with NTM-PD (Table 1). Mean (SD) age of participants was 63.5 (13.3) years, range 21–89, and 58% (n = 23) were female. The majority of participants were non-Hispanic White (n = 31, 78%), followed by Asian (n = 4, 10%), White Hispanic (n = 2, 5%), Black non-Hispanic (n = 2, 5%), and Black Hispanic (n = 1, 3%) individuals. Just over half of the participants (55%; n = 22) were currently receiving treatment for NTM-PD, and 25% (10) did not have underlying bronchiectasis. A total of 30 participants completed the SDMT (oral version). The 10 participants who did not complete the SDMT did so for the following reasons: n = 7 (23%) due to technical difficulties (e.g., interview conducted by phone, loss of internet connection), and n = 3 because they were too ill to complete the oral exam. Among those completing the exam, 12 (38%) had completed some college or less, and 18 (62%) had completed college or professional/graduate degrees. The mean score was 35.6 (SD 10.5), which was −1.5 SD below the expected mean of 54.3 (normed by age group and education). Only 2 (7%) were within −0.5 SD of the mean, and 12 (41%) were at least 2 SD below the mean.
Population and NTM-PD characteristics, n = 40 interview study and n = 230 psychometric study.

Two White Hispanic, one Black Hispanic, one Black non-Hispanic, and four Asian.
Missing 139 observations (n = 91) in psychometric study.
Missing 146 observations (n = 84) in psychometric study.
Four were never treated, and 14 were previously treated for the interview study; 15 were never treated, and 19 were previously treated for the psychometric study.
PRO scores are presented in Table 2 for the n = 38 (95%) subjects who completed surveys. Emotional functioning was very low, with a mean of 29, and the remaining QOL-B domain means ranged from 46 to 55. The NTM Symptoms mean score was 66, with the other 3 domain means ranging from 70 to 75. Scores revealed a large SD and range. Overall, 7 (18%) screened positive for anxiety and 12 (32%) screened positive for depression. Further, when asked about their current health status, 13 (33%) reported they were in good health, 6 (15%) in fair health, 16 (40%) in poor health, and 3 (8%) were “feeling fragile.”
Patient-reported outcome results (n = 38 interview study with surveys complete).

Scores are mean (SD) or n (%).
GAD-7/PHQ-8 score categories: none = 0–4, mild = 5–9, moderate = 10–14, severe = 15+.
QOL-Bronchiectasis (QOL-B) and NTM Module are scaled 0–100, 0 = worst and 100 = best.
Psychometric study
The psychometric study included 230 adult patients with NTM-PD (Table 1). Most patients were 65 years or older (77%) and 91% were female (n = 210). Of the 230 participants, 210 identified as non-Hispanic White (91%). Additionally, 30 (13%) patients reported no college degree, while 200 (87%) had completed at least some college. Of the 139 patients enrolled through NTMir, 84 completed additional questions regarding treatment; more than half of these participants (60%; n = 50) were currently receiving treatment for NTM-PD and only 5% (n = 4) did not have underlying bronchiectasis. Of the 217 patients with GAD-7/PHQ-8 results, 31 (14%) screened positive for anxiety and 41 (19%) screened positive for depression (GAD-7 or PHQ-8 score 10+, respectively, Table 3). QOL-B respiratory symptom scores (RSS) were a mean of 67 (18). More than 80% of patients (189) reported mild or moderate MAC disease symptom severity using the PGIS, with only five patients reporting very severe symptoms.
Patient-reported outcome results (n = 230 psychometric study).

Scores are mean (SD) or n (%).
GAD-7/PHQ-8 score categories: none = 0–4, mild = 5–9, moderate = 10–14, severe = 15+; 13 missing scores (n = 217).
QOL-Bronchiectasis (QOL-B) is scaled 0–100, 0 = worst and 100 = best.
Patient global impression of severity of MAC disease symptoms, 5-level scale scored 0 to 4.
PROMIS t-score (mean 50, SD 10); higher is better for cognitive function (SF6a) and sleep disturbance (SF4a); higher is worse for fatigue (SF7a).
Associations between respiratory symptoms, fatigue, and anxiety
The mean scores for respiratory symptoms (moderate/severe anxiety: 58 vs 69; mild/moderate/severity anxiety: 61 vs 71), cognitive functioning (moderate/severe: 38 vs 50; mild/moderate/severe: 42 vs 53), and sleep disturbance (moderate/severe: 47 vs 56; mild/moderate/severe: 51 vs 57) were significantly worse among those who screened positive for anxiety compared to those who screened negative, regardless of symptom threshold, yet larger mean score group differences were found with moderate/severity anxiety symptoms (Table 4). Similarly, worse mean scores of fatigue were found in the group screening positive for anxiety (moderate/severe: 65 vs 53; mild/moderate/severe: 60 vs 51) compared to those screening negative for anxiety.
Comparison of patient-reported outcome measures by GAD-7 anxiety and PHQ-8 depression screening results (n = 230 psychometric study).
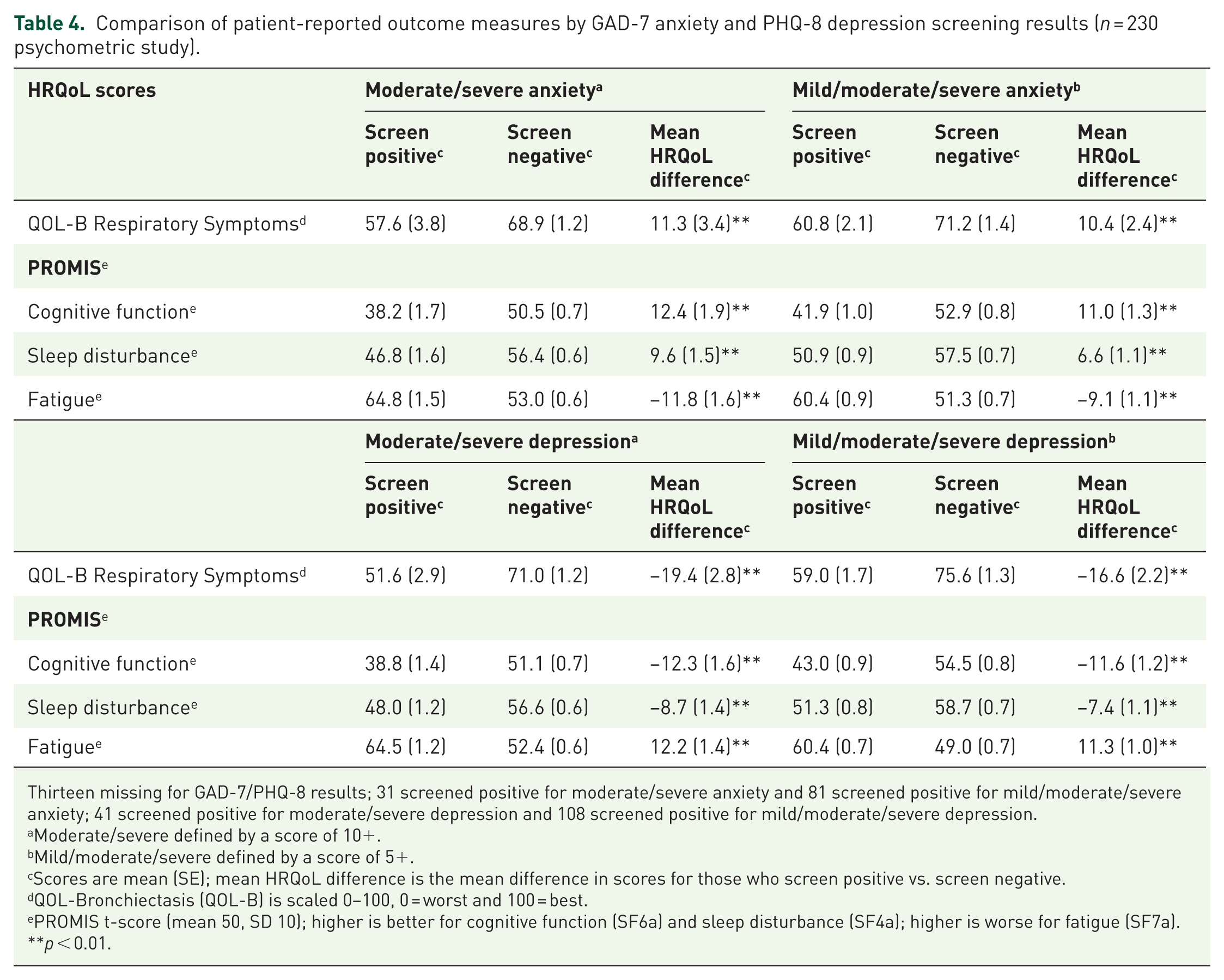
Thirteen missing for GAD-7/PHQ-8 results; 31 screened positive for moderate/severe anxiety and 81 screened positive for mild/moderate/severe anxiety; 41 screened positive for moderate/severe depression and 108 screened positive for mild/moderate/severe depression.
Moderate/severe defined by a score of 10+.
Mild/moderate/severe defined by a score of 5+.
Scores are mean (SE); mean HRQoL difference is the mean difference in scores for those who screen positive vs. screen negative.
QOL-Bronchiectasis (QOL-B) is scaled 0–100, 0 = worst and 100 = best.
PROMIS t-score (mean 50, SD 10); higher is better for cognitive function (SF6a) and sleep disturbance (SF4a); higher is worse for fatigue (SF7a).
p < 0.01.
Associations between respiratory symptoms, fatigue, and depression
The mean scores for respiratory symptoms (moderate/severe depression: 52 vs 71; mild/moderate/severe depression: 59 vs 76), cognitive functioning (moderate/severe: 39 vs 51; mild/moderate/severe: 43 vs 54), and sleep disturbance (moderate/severe: 48 vs 57; mild/moderate/severe: 51 vs 59) were significantly worse among those who screened positive for depression compared to those who screened negative, regardless of symptom threshold (Table 4); similar to anxiety, larger mean score group differences were found with moderate/severe depression symptoms. Similarly, worse mean scores of fatigue were found in the group screening positive for depression (moderate/severe: 64 vs 52; mild/moderate/severe: 60 vs 49) compared to those screening negative for depression.
The scores for most HRQoL domains were worse for patients screening positive for both anxiety and depression (Table 5), compared to individual positive screening results in Tables 4 and 5. Excluding participants who screened positive for either depression or anxiety (but not both) increased differences in mean HRQoL scores compared to positive (e.g., those screening negative for both had better HRQoL scores). Furthermore, the PROMIS scores for those screening positive for both tests were 1 SD below the mean for cognitive functioning (moderate/severe: 36; mild/moderate/severe: 41) and between 1 and 2 standard deviations above the mean for fatigue (moderate/severe: 68; mild/moderate/severe: 62).
Comparison of patient-reported outcome measures by positive for both GAD-7 anxiety and PHQ-8 depression with those screening negative (n = 230 psychometric study).
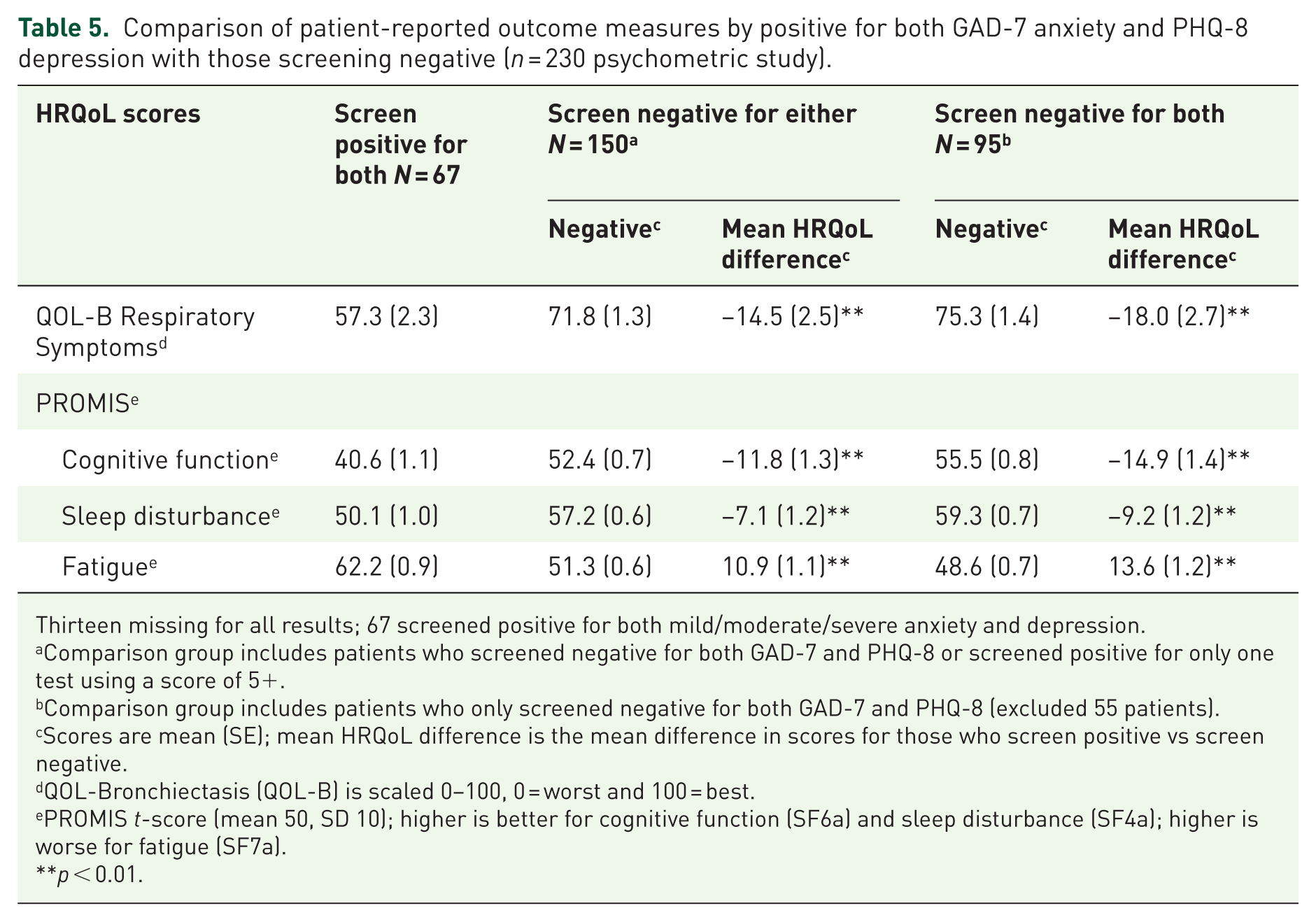
Thirteen missing for all results; 67 screened positive for both mild/moderate/severe anxiety and depression.
Comparison group includes patients who screened negative for both GAD-7 and PHQ-8 or screened positive for only one test using a score of 5+.
Comparison group includes patients who only screened negative for both GAD-7 and PHQ-8 (excluded 55 patients).
Scores are mean (SE); mean HRQoL difference is the mean difference in scores for those who screen positive vs screen negative.
QOL-Bronchiectasis (QOL-B) is scaled 0–100, 0 = worst and 100 = best.
PROMIS t-score (mean 50, SD 10); higher is better for cognitive function (SF6a) and sleep disturbance (SF4a); higher is worse for fatigue (SF7a).
p < 0.01.
Correlations between anxiety and depression screening tests with respiratory symptoms and PROMIS scales (cognitive functioning, fatigue, and sleep disturbance) are presented in Table 6. Significant correlations were found between all HRQoL domains and mental health screening test outcomes for both the moderate/severe symptoms and mild/moderate/severe symptoms thresholds. Stronger correlations were found when utilizing the mild/moderate/severe symptoms threshold. Fatigue showed the highest correlation with most mental health outcomes, in particular screening positive for depression. Overall, screening positive on any or both mental health screeners was significantly correlated with worse QOL-B RSS, worse cognitive function and sleep quality, and worse fatigue.
Correlations between mental health and health-related quality-of-life measures (n = 230 psychometric study).
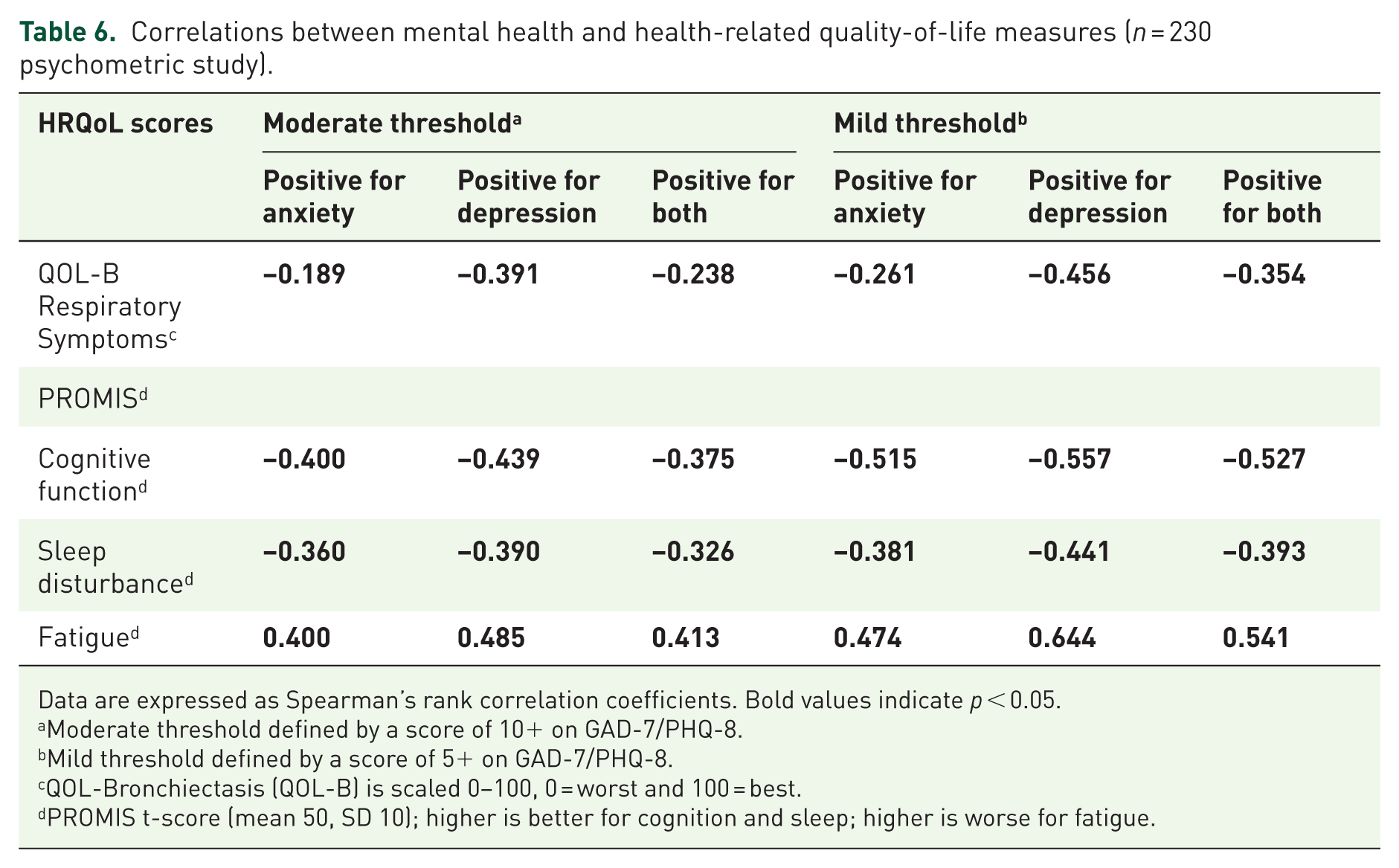
Data are expressed as Spearman’s rank correlation coefficients. Bold values indicate p < 0.05.
Moderate threshold defined by a score of 10+ on GAD-7/PHQ-8.
Mild threshold defined by a score of 5+ on GAD-7/PHQ-8.
QOL-Bronchiectasis (QOL-B) is scaled 0–100, 0 = worst and 100 = best.
PROMIS t-score (mean 50, SD 10); higher is better for cognition and sleep; higher is worse for fatigue.
Significant positive correlations were found between QOL-B respiratory symptoms and both cognitive functioning and sleep disturbance scores, and significant negative correlations are found between fatigue and respiratory symptoms, cognitive functioning, and sleep disturbance scores (Table 7). Accordingly, as fatigue symptoms worsened, all other symptoms were found to decline as well. Further, when stratified by treatment history the mean difference in symptom and HRQoL scores comparing those on with those not on treatment was not statistically significant (Table 8).
Correlations between QOL-B respiratory symptoms and PROMIS cognitive function, fatigue, and sleep disturbance scales (n = 230 psychometric study).

Data are expressed as Pearson’s correlation coefficients. Bold values indicate p < 0.05.
PROMIS t-score (mean 50, SD 10); higher is better for cognition and sleep; higher is worse for fatigue.
QOL-Bronchiectasis (QOL-B) is scaled 0–100, 0 = worst and 100 = best.
Comparison of patient-reported outcome measures by treatment status (n = 84 psychometric study).

One hundred forty-six missing treatment status for psychometric study.
Scores are mean (SE); mean HRQoL difference is the mean difference in scores for those on treatment vs. not on treatment.
15 were never treated and 19 were previously treated for psychometric study.
QOL-Bronchiectasis (QOL-B) is scaled 0–100, 0 = worst and 100 = best.
PROMIS t-score (mean 50, SD 10); higher is better for cognitive function (SF6a) and sleep disturbance (SF4a); higher is worse for fatigue (SF7a).
Discussion
The results of this study indicated that the prevalence of depression and anxiety is high in patients with NTM-PD, and PRO measures of HRQoL and symptoms were significantly worse among patients screening positive for anxiety, depression, or both mental health conditions. More than half of patients reported mild or moderate depression symptoms while just under half of the patients reported mild or moderate anxiety symptoms, in both NTM-PD populations examined. The presence of anxiety and depression were correlated with increased fatigue and decreased cognitive functioning and sleep disturbance.
Although estimates vary across countries, approximately 5% of adults experience depression and 4% experience anxiety among the general population. 10 Individuals with other chronic respiratory disease also experience a significantly higher prevalence of depression and anxiety, with rates ranging from 10% to 57% for depression and 7% to 50% for anxiety.14,34–36 Limited prior research has examined the prevalence and impact of depression and anxiety among patients with NTM-PD.37,38 A 2025 study of 543 NTM-PD patients across eight European countries found most patients (82%) reported experiencing increased depression or anxiety due to NTM-PD, with almost half (49%) reporting serious restrictions to their daily life activities. 39 Another study of 124 patients with bronchiectasis and NTM-PD, 20% reported at least mild anxiety using the GAD-7, and 28% reported at least mild depression using the PHQ-9. 37 Similar to findings in patients with COPD, 40 tuberculosis, 41 and CF, 42 the proportion screening positive for anxiety and depressive symptoms in this study were 3–4 times higher than global prevalence estimates, 14% (31/217) and 19% (41/217) for those in the psychometric study and 18% (7/38) and 31% (12/38) for those in the interview study, respectively. Prior research in other chronic lung conditions (i.e., CF) indicate that patients with increased depression and anxiety have worse disease management, including more missed clinic appointments, worse adherence to treatments, and higher health care utilization and costs. 43 In one study of 1000 adults with CF, the 5-year mortality of patients who screened positive for depression was twice that of those who screened negative. 44 Clinical and HRQoL implications of these high rates of psychological symptoms underscore the need for a patient-centered approach to care that goes beyond treating the physical manifestations of the disease to consider the psychological well-being of patients.
Over the last decade, addressing mental health conditions has become a priority for the CF community and has changed clinical practice. 42 Specifically, care pathways and provision of high-quality care for depression and anxiety have followed the implementation of a screening program. Furthermore, the PHQ-9 and GAD-7 screening measures have been recommended and adopted by most national healthcare guidelines committees because they are brief, map onto the DSM-V criteria, are sensitive to the presence of elevated symptoms of depression and anxiety, are free, and have been translated into all major languages. 38 Given the high rates of anxiety and depression found in the NTM-PD population and overlapping symptom profiles with the CF community, similar guidelines and multidisciplinary care systems should be developed for the NTM community. The national implementation of mental health screening and treatment into CF care has demonstrated that depression and anxiety can be efficiently evaluated and treated in a complex, chronic lung disease. 45
In our study, even mild anxiety or depression was associated with worse respiratory symptoms, fatigue, cognitive functioning, and sleep disturbance. Chronic NTM-PD is a complex lung disease that can be challenging to treat in part due to significant adverse side effects of long-term, multidrug therapies. 46 Patients and clinicians weigh risk and benefit trade-offs when deciding to initiate treatment for NTM-PD. In our study, similar to the findings of Niknafs et al., 37 we did not find any significant differences in PROs between those on treatment and those not currently on treatment. This finding provides support for the idea that the high fatigue, poor cognition, and poor sleep quality reported by patients in this study are more likely related to their NTM-PD rather than their treatment and may also be associated with the anxiety and depression they are experiencing. While treatment is poorly tolerated by some and may contribute to anxiety and depression, it does not appear to explain the results identified here.
A key strength of the study was evaluating mental health and HRQoL in a large, heterogeneous, typical population of symptomatic people living with NTM-PD. However, the study had several limitations. While 230 patients were recruited for the psychometric study, the various recruitment methods (in-person with detailed chart review vs remote) resulted in some with missing disease characteristics (i.e., cavitary disease, NTM species), limiting statistical power to evaluate differences. Second, the psychometric study sample was almost entirely composed of older White non-Hispanic females, which reflects the demographic typically impacted by NTM-PD, but limits the generalizability of our findings. Cultural perceptions, access to care, and socio-economic status are known to influence the presentation and management of mental health disorders and HRQoL; thus, the homogeneity in participant demographics precludes us from making inferences about other populations. While sex differences in HRQoL domains and mental health symptoms among the NTM-PD population are limited, findings among chronic lung disease populations suggest females with chronic lung diseases report higher rates of anxiety and depression and worse quality of life despite similar or better lung function.47,48 Specifically, Laurin et al. found that females with COPD experienced more than 1.5 times the rate of anxiety disorders and were more than 2 to 3 times more likely to report mood disorders, compared to men with COPD. 47 Third, the topic of mental health may result in social desirability bias and the possibility of under-reporting their symptoms of depression and anxiety. This could potentially lead to results that are underestimates of the true burden of mental health in NTM-PD populations. Additionally, the PHQ-8 was used to assess depressive symptoms, and while a validated diagnostic tool, it excludes the ninth item related to suicidal ideation included in the PHQ-9. As a result, we are unable to comment on rates of suicidality in this population. Lastly, the study used a cross-sectional design, which prevents the ability to examine causal relationships between psychological symptoms and PROs, for example, whether anxiety and depression cause poorer HRQoL and worse symptoms or vice-versa.
Conclusion
This study found that nearly 1 in 5 (19%) people living with NTM-PD, a chronic pulmonary condition affecting older adults, screened positive for depression and 1 in 6 (14%) screened positive for anxiety (Table 3). Screening positive for anxiety and/or depression was significantly correlated with worse HRQoL across multiple PRO measures. Furthermore, longitudinal studies examining relationships among mental health symptoms, treatment adherence, and burden, and HRQoL is a key future direction for research. These results strongly support the implementation of routine mental health screening for people living with NTM-PD, using a model for intervention that follows the approach developed for CF patients, which is now fully integrated into every CF center and clinic in the United States. 39
Supplemental Material
sj-docx-1-tar-10.1177_17534666251396240 – Supplemental material for The association between mental health, cognitive functioning, and health-related quality of life in adults with chronic nontuberculous mycobacterial pulmonary disease
Supplemental material, sj-docx-1-tar-10.1177_17534666251396240 for The association between mental health, cognitive functioning, and health-related quality of life in adults with chronic nontuberculous mycobacterial pulmonary disease by Madysen Schreiber, Alexandra L. Quittner and Emily Henkle in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.