
Abstract
Background:
Chronic cough (CC) has a negative effect on patients’ quality of life and everyday activities. Emotional reactions are an important aspect of how patients deal with illness, and CC can lead to feelings of uncertainty, loss of control, helplessness, self-consciousness, embarrassment, worry, fear, frustration, irritability, and anger.
Objectives:
To assess the emotions related to bouts of cough in patients with refractory or unexplained chronic cough (RCC/UCC), using a validated questionnaire.
Design:
This was a multicenter, non-interventional study.
Methods:
Patients with RCC/UCC were recruited from hospital outpatient clinics in Spain. The impact of RCC/UCC on patients’ emotions was assessed using the self-reported Discrete Emotions Questionnaire (DEQ), which assesses eight distinct situationally induced state emotions, scored on a Likert scale from 1 to 7, with higher scores indicating that the emotion is experienced to a greater degree.
Results:
The survey was completed by 190 patients (148 women, 42 men; mean age 58.0 years) of whom 120 had RCC and 70 had UCC (mean cough duration 6.3 years). Highest mean (SD) scores were seen for the anger subscale (3.6 (1.7)) and anxiety subscale (3.3 (1.6), followed by the disgust (2.6 (1.5)), fear (2.6 (1.7)), and sadness (2.5 (1.5)) subscales. The same pattern was seen in subgroups by gender and by diagnosis (RCC or UCC). There were no significant differences in mean scores for any subscale between patients with RCC and those with UCC. Cough severity and the presence of cough-related stress urinary incontinence (SUI) were independently associated with negative emotion subscale scores.
Conclusion:
Among patients with RCC/UCC, bouts of cough triggered negative emotions such as anger, anxiety, disgust, fear, and sadness, as evaluated using a validated questionnaire. Results were similar for RCC and UCC. Increasing cough severity and the presence of SUI were independently associated with higher (worse) scores for negative emotions.
Introduction
Chronic cough, which is defined as a cough that persists for 8 weeks or longer, has a global prevalence of approximately 10%. 1 The management of chronic cough includes avoidance of cough triggers, reduction of hypersensitivity, and treatment of underlying conditions. 2 However, management can be challenging in the subset of patients who have refractory chronic cough (RCC) or unexplained chronic cough (UCC). 3 Population-based studies in Europe suggest that 21–47% of people with chronic cough have UCC4–6 and 17% potentially have RCC. 7 A recent clinic-based study in Poland found that 27%–31% of patients with chronic cough had RCC. 8
Chronic cough has a negative effect on patients’ quality of life (QoL) and everyday activities.9–15 It also has an adverse effect on mood and is associated with increased levels of anxiety and depression.16–20 Emotional reactions are an important aspect of how patients deal with illness, 21 and chronic cough can lead to feelings of uncertainty, loss of control, helplessness, self-consciousness, embarrassment, worry, fear, frustration, irritability, and anger.10,18,22-25
The discrete emotions can be categorized along three dimensions: valence of the emotion (positivity or negativity), arousal (high or low), and motivational direction (approach or avoid). As an example, anger is regarded as a negative, high arousal emotion associated with approach motivational tendency (the person feeling anger in front of a situation is more likely to face it than to avoid or move away from it), while disgust is also regarded as a negative, high arousal emotion, but associated with withdrawal motivational tendency (the person feeling disgust is more likely to move away from what is causing it). On the contrary, happiness is considered a positive emotion associated with approach motivation. 26 To date, the emotional impact of experiencing bouts of cough in patients with chronic cough has not been studied using a validated questionnaire.
The Discrete Emotions Questionnaire (DEQ) is a validated questionnaire that measures eight distinct state emotions, including the basic emotions of anger, disgust, fear, sadness, and happiness, plus the emotions of anxiety, desire, and relaxation, 26 induced by a specific situation. The DEQ has been used to assess emotions linked to different theoretical everyday life situations (including news, images, or scenarios)26,27 and also after experiencing specific situations, such as virtual visits to relatives admitted to Intensive Care Units during COVID-19 pandemic restrictions. 28
However, to the best of our knowledge, the DEQ has never been used to assess in-depth emotions related to specific medical situations. Because patients with chronic cough suffer repeated bouts of cough, often in front of other people or in embarrassing situations, we postulated that suffering bouts of cough may trigger different emotions and was, therefore, worth exploring with the DEQ. In the current paper, we aim to describe the emotions triggered by bouts of cough in patients with RCC/UCC, potential differences between different patient profiles, and the factors associated with such emotions. This assessment was a prespecified objective of a larger study in patients with RCC/UCC seen at hospital outpatient clinics in Spain to understand the burden of RCC/UCC on different aspects of healthcare resource utilization, patients’ physical symptoms, QoL, and everyday life activities, for which different information has already been published.13,29–31
Methods
The current work was part of a larger multicenter study involving a cohort of patients with RCC/UCC recruited from allergy and pulmonology outpatient clinics at hospitals within the Spanish National Healthcare System. The overall objectives of the study were to describe disease characteristics and the management of RCC/UCC in these centers, and to assess the impact of cough on patients. The assessment of the emotional response to cough was a prespecified objective of the study. The authors used the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist in the preparation of this manuscript. 32
Patients
Consecutive adult patients attending outpatient pulmonology or allergy clinics with RCC or UCC were invited to participate in the study. Patients were invited if (1) they were adults (>18 years of age); (2) had, according to physicians’ diagnosis, RCC (defined as cough in a patient with a known underlying disease that was refractory to the correct treatment of the underlying condition) or UCC (cough in a patient that had undergone an appropriate investigation, according to guidelines and the best available evidence, and an underlying condition had not been found); (3) had been seen for chronic cough for the first time more than 1 year before study entry; (4) had cough at the study visit date; and (5) provided signed informed consent. Exclusion criteria included current smoking (or having stopped smoking in the previous 12 months); current treatment with angiotensin-converting enzyme inhibitors; cough related to chronic obstructive pulmonary disease, cancer, active infection, bronchiectasis, interstitial lung disease, cystic fibrosis or Gilles de la Tourette syndrome; current participation in an interventional study; and any conditions judged as incompatible with study participation by the treating physician (e.g., cognitive impairment, major depression, and end-stage disease).
Procedures
After patients signed written informed consent, information on cough characteristics and management was collected retrospectively from hospital clinical charts. Additionally, patients were invited to complete a cross-sectional survey where they provided information about the impact of chronic cough. The content of the survey completed by patients is provided as an Annex. The survey was completed on paper, the day they signed informed consent, without a physician’s overview, placed in an envelope, and sealed. The survey comprised validated questionnaires to measure QoL, ad hoc questions developed to assess the impact of cough on physical problems, patients’ everyday life, and a Visual Analog Scale (VAS) for self-assessment of cough severity; outcomes for these aspects have been reported previously.13,29–31 QoL assessments comprised the EuroQoL 5-Dimension 5-level (EQ-5D-5L) questionnaire and the Leicester Cough Questionnaire (LCQ). The EQ-5D-5L VAS score, the EQ-5D-5L index, and the LCQ total score and LCQ scores for the different domains (physical, psychological, and social) were obtained. The presence of cough-related stress urinary incontinence (SUI) was considered if there was a diagnosis documented in clinical charts or if it was reported as a physical complication reported by patients (considering cough-related SUI if patients responded “frequently” or “mostly/always” to the question “Do you ever have urinary incontinence (loss of urine) due to your cough?”). 31
Emotions related to cough were assessed using a validated questionnaire (the DEQ). The DEQ is a validated questionnaire that allows the measurement of eight distinct situationally induced state emotions. 26 The questionnaire provides a list of 32 items relating to these eight state emotions, which patients self-assess in the presence of an event. They indicate the extent to which they experienced the emotions using a Likert scale with the following seven response options (1 “Not at all”; 2 “Slightly”; 3 “Somewhat”; 4 “Moderately”, 5 “Quite a bit”; 6 “Very much”; and 7 “An extreme amount”). The 32 items are grouped into the following eight subscales reflecting state emotions: Anger (anger, mad, pissed off, rage); Disgust (grossed out, revulsion, sickened, nausea); Fear (terror, scared, fear, panic); Anxiety (worry, anxiety, dread, nervous); Sadness (lonely, grief, sad, empty); Desire (wanting, craving, longing, desire); Relaxation (calm, relaxation, chilled out, easygoing); Happiness (happy, enjoyment, satisfaction, liking). A mean score is provided for each subscale, ranging from 1 to 7, with higher mean scores indicating that the emotion is experienced to a greater degree.
For this study, a translation (from English to Spanish) and back-translation (the result in Spanish to English) of the DEQ were done with the participation of fluent experts in English and Spanish. The DEQ was included in Spanish as part of the paper survey completed by patients. Patients were instructed to complete the DEQ after assessing the intensity of the emotions they felt by responding to the question: “While suffering bouts of cough, to what extent do you experience these emotions?”.
Statistical analysis
The objectives of this study were primarily exploratory, with no hypothesis prespecified. The calculated sample size (196 patients) allowed 95% confidence and 7% precision for an expected prevalence of 50% of any categorical variable. 29 No stratification was required between RCC and UCC groups.
The different items of the DEQ were presented as means with standard deviation (SD) and percentage of patients who indicated higher scores (i.e., score of 5 (Quite a bit), 6 (Very much), or 7 (An extreme amount)). The mean and SD for each of the eight subscales were also summarized. Comparisons across different subgroups were made using the Student t-test or ANOVA. Where appropriate, linear-by-linear tests were used. The correlation between the DEQ subscales and QoL assessments (EQ-5D-5L and LCQ total and domain scores) was assessed by calculating the Spearman’s Rho (ρ) correlation coefficients, where values close to +1 or −1 denote a strong (positive or negative, respectively) relationship, while values close to 0 indicate a weak or no relationship. A linear regression analysis was performed for each subscale to explore variables associated with each emotion. Because there was an imbalance in the percentage of women and men included in the study, and the prevalence of cough-related SUI was much higher in women than in men, we performed a specific analysis in female patients. All analyses were performed using the IBM SPSS 20.0 statistical program.
Results
This study enrolled 196 patients with RCC/UCC between November 2020 and June 2022, 190 of whom completed the survey (148 women and 42 men; mean age 58.0 years). The diagnosis was RCC in 120 patients and UCC in 70. The characteristics of the sample are displayed in Table 1. Cough-related SUI reported by patients or noted in clinical charts was present in 70 patients (65 women (44.2%) and 5 men (11.9%)).
Patient characteristics.

EQ-5D-5L, EuroQoL 5 Dimensions 5 Levels; RCC, Refractory Chronic Cough; SD, Standard Deviation; SUI, Stress Urinary Incontinence; UCC, Unexplained Chronic Cough; VAS, Visual Analog Scale.
Mean (SD) scores and the percentages of patients with high scores (i.e., score of 5 [Quite a bit], 6 [Very much], or 7 [An extreme amount]) for each of the 32 items of the DEQ are shown in Supplemental Table 1. Higher mean scores and higher percentages of patients with high scores, were seen for items related to anger (mean scores 3.0–3.9; percentage of high scorers 24.6%–43.7%) and anxiety (mean scores 3.0–3.7; percentage of high scorers 24.2%–35.3%), followed by items related to disgust, fear, and sadness.
Mean (SD) scores for the eight DEQ subscales are presented for the overall study population and by different variables of interest (age, gender, diagnosis, and cough duration) in Supplemental Table 2(a)–(d). In the overall population, the highest mean scores were seen for the anger and anxiety subscales (3.6 [1.7] and 3.3 [1.6], respectively), followed by disgust (2.6 [1.5]), fear (2.6 [1.7]), and sadness (2.5 [1.5]). Scores for desire, relaxation, or happiness were lower. There were no significant differences in the mean scores between patients above and below the median age, or in patients with RCC and those with UCC, or in patients with different cough duration (all p-values > 0.05, except for desire, which was higher in patients with cough duration above the median, p = 0.024). Mean scores for anger, anxiety, disgust, fear, and sadness were about 0.3–0.4 points higher in women compared with men, but the differences did not reach statistical significance (p-values 0.141, 0.373, 0.219, 0.146, and 0.096, respectively). Mean scores for the relaxation and happiness subscales were low, but men scored higher than women, with the difference achieving statistical significance for the happiness subscale (1.7 [1.1] vs 1.3 [0.7], p = 0.004; Supplemental Table 2(a)).
Figures 1 and 2 display the scores for the eight DEQ subscales stratified by tertiles of cough severity VAS score (Figure 1) and by presence/absence of cough-related SUI (Figure 2). Mean scores for the anger, anxiety, disgust, fear, sadness and desire DEQ subscales were significantly higher (linear trend) in patients with more severe cough as assessed by VAS (all p < 0.001; Figure 1), and in patients with cough-related SUI compared with those without SUI (p = 0.001 for desire, p < 0.001 for anger, anxiety, disgust, fear and sadness, Figure 2). There were no associations between the relaxation or happiness subscales and cough severity or cough-related SUI.

Mean (SD) score for each of the eight subscales of the DEQ by cough severity VAS tertiles.
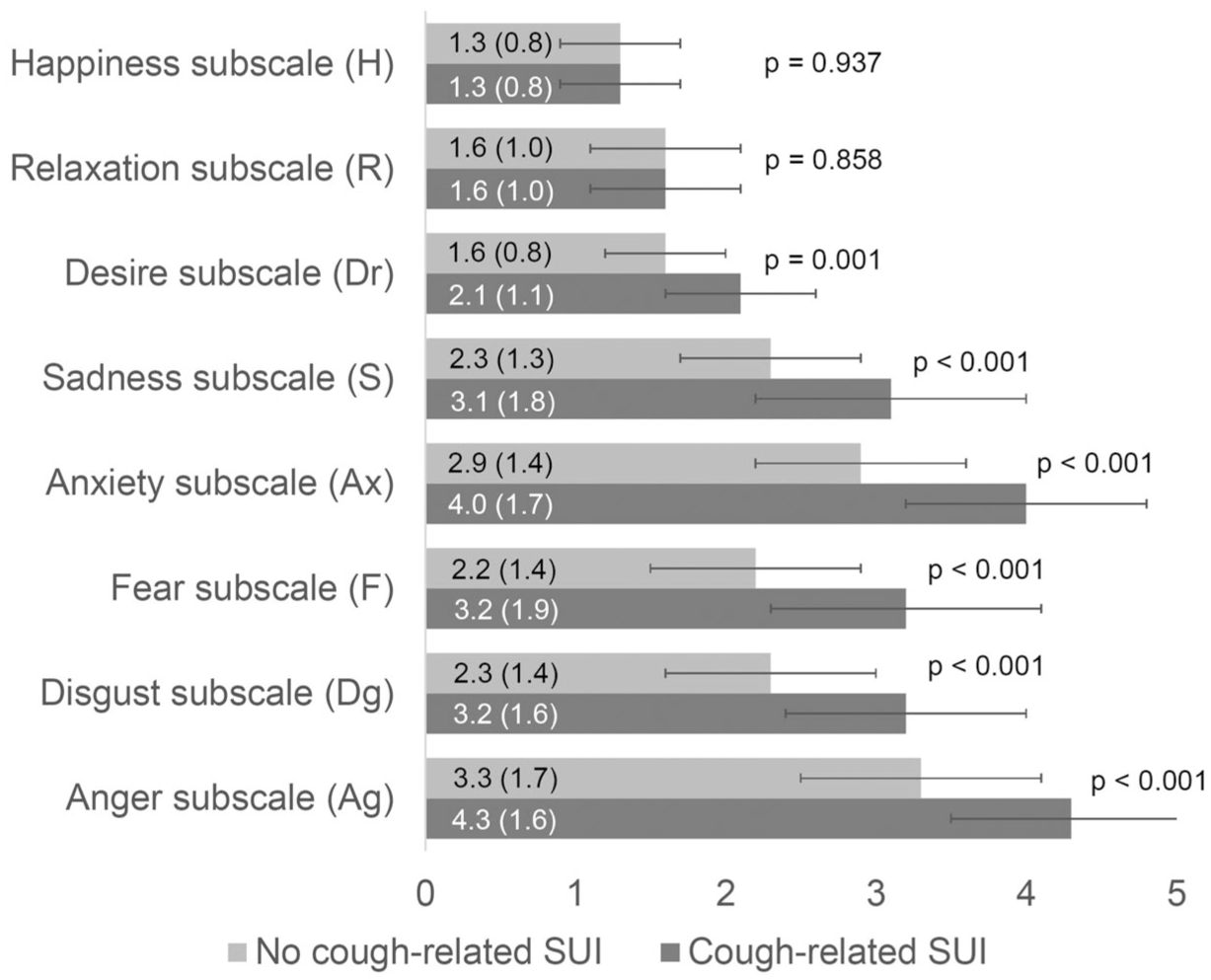
Mean (SD) score for each of the eight subscales of the DEQ by the presence or absence of SUI.
The correlation analysis (Table 2) showed a moderate-to-strong correlation between the scores of the DEQ negative emotions (anger, disgust, fear, anxiety, and sadness) and the LCQ total and domain scores. The strongest correlations were found between these DEQ scores and the LCQ psychological domain and total scores, with Rho correlation coefficients between −0.55 and −0.75, indicating a negative relationship (higher emotion scores (i.e., emotion experienced to a higher degree) with lower LCQ scores (i.e., more impairment in cough-related QoL)). Rho correlation coefficients between negative emotions and LCQ physical and social domains ranged between −0.50 and −0.65. Correlations with EQ-5D-5L were also negative but weaker (−0.35 to −0.50). Correlations of desire, relaxation, and happiness subscales with QoL assessments were weak or very weak (Table 2).
Correlation between each of the eight subscales of the DEQ and quality of life measurements (EQ-5D-5L and Leicester Cough Questionnaire).

Values are Rho Spearman correlation coefficients.
DEQ, Discrete Emotions Questionnaire; EQ-5D-5L, EuroQoL 5 Dimensions 5 Levels; LCQ, Leicester Cough Questionnaire; VAS, Visual Analog Scale.
Multivariate models identified cough severity and cough-related SUI as independent variables associated with the anger, anxiety, disgust, fear, sadness, and desire subscale scores (Table 3). For most associations, DEQ subscale increments of approximately 0.25 to 0.30 were seen for each 10 mm increment in cough severity VAS score, while the presence of cough-related SUI was associated with increments of approximately 0.5 in the sadness and desire subscales, and approximately 0.8 in the anger, disgust, and fear and anxiety subscales. Only the male gender was associated with the happiness subscale score, while no variables were found to be associated with the relaxation subscale score. A specific analysis in women (n = 148) showed similar outcomes in terms of associations between cough severity, VAS, or cough-related SUI and emotions to those seen in the overall population (Supplemental Tables 3 and 4).
Variables associated with the different subscales of the Discrete Emotions Questionnaire in multiple linear regression models.
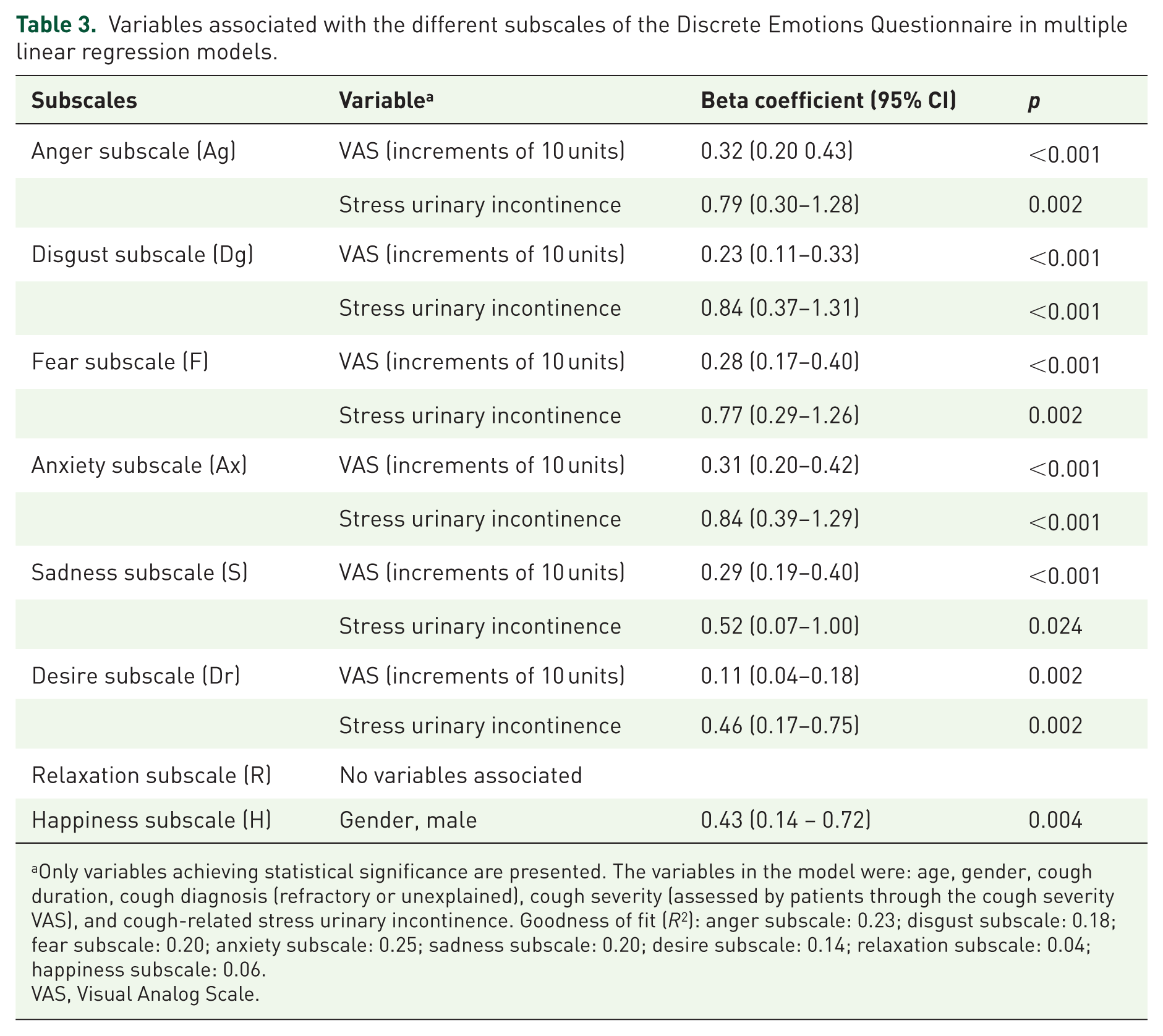
Only variables achieving statistical significance are presented. The variables in the model were: age, gender, cough duration, cough diagnosis (refractory or unexplained), cough severity (assessed by patients through the cough severity VAS), and cough-related stress urinary incontinence. Goodness of fit (R2): anger subscale: 0.23; disgust subscale: 0.18; fear subscale: 0.20; anxiety subscale: 0.25; sadness subscale: 0.20; desire subscale: 0.14; relaxation subscale: 0.04; happiness subscale: 0.06.
VAS, Visual Analog Scale.
Discussion
To the best of our knowledge, this is the first study that has used the DEQ to assess the emotions triggered by bouts of cough in a population with RCC/UCC. The results provide important insights about the impact that chronic cough has on patients. Scores were higher in the negative emotion subscales (anger, anxiety, disgust, fear, and sadness).
The DEQ is intended to measure state emotions, and, in a nonemotional situation, responses to the negative emotion subscales should be close to the lowest scores possible. The high scores for these subscales seen in our study suggest that, in patients with RCC/UCC, bouts of cough have a negative effect on their emotional status. This adds further burden to patients, in addition to the already well-described adverse effect of chronic cough on QoL and everyday activities.10,13,16,25
RCC/UCC has been shown to impair global health-related QoL 14 and cough-specific QoL across physical, psychological, and social domains.11,12,15,33,34 Previous reports from our study have highlighted the impairment of patients’ QoL, as described by low LCQ total, psychological, social, and physical scores (lower scores indicate worse QoL). 13
Therefore, it is not surprising that chronic cough affects patients’ mood and emotions. Qualitative analyses indicate that patients with RCC/UCC report feelings of anger, guilt, sadness, anxiety, worry, pessimism, embarrassment, frustration, helplessness, and loss of motivation.11,12 We have previously described that 41.9% of patients reported that the greatest cough-related impact on everyday life was on mood/emotions. 13 Therefore, the results of the present DEQ evaluation expand on the emotional impact of RCC/UCC by using a validated questionnaire that allows quantification of the different emotions.
The highest mean scores reported in our study (indicating that the emotion was experienced to a higher degree) were seen for anger and anxiety, both in the overall population and in subgroups based on gender and diagnosis (RCC or UCC). The next highest scores were seen for the disgust, fear, and sadness subscales. Of interest, while anxiety is frequently described as part of the burden associated with chronic cough,17,18,23,24 anger is not generally described nor detected at the clinic. The reason for this lack of awareness of anger might be related to how the emotions are evaluated with the DEQ. The DEQ assesses emotions related to a specific event, and for this study, we asked patients to assess their emotions in relation to the event “suffering bouts of cough,” by responding to the question “While suffering bouts of cough, to what extent do you experience these emotions?”. In the clinic, patients likely focus more on “chronic emotional states” like anxiety or depression, and not on the experiences they might be suffering (like anger) when they have bouts of cough, which are acute events. This is interesting and complementary information that can be missed at the clinic, and being aware of it might help clinicians to treat RCC/UCC patients more holistically. As bouts of cough and subsequent triggered emotions can frequently occur in front of others or in embarrassing situations (like at work, or in crowded places), patients might need psychological, social, or behavioral support to cope with their condition and minimize the emotional impact. The correlation found between these negative emotions and QoL assessments (especially with the LCQ psychological domain) supports this approach. Mean scores for the desire, relaxation, and happiness subscales were low (i.e., not experienced as much). There was a non-significant trend toward higher scores for negative emotions in women compared with men. Men had significantly higher mean scores than women for the relaxation and happiness subscales; however, the scores were all low. These findings are consistent with the results of the QoL evaluation for the study, which found that women reported poorer cough-related QoL than men (assessed using the LCQ). 13 The specific analysis on women showed similar associations as for the overall population.
The DEQ measures emotions as reported by patients, assessing eight subscales that are sensitive to situational changes in emotional states, and which encompass a range of basic and important discrete emotions. 26 Other measures of self-reported emotions that focus on discrete emotions (rather than broad dimensions) are available, such as the Profile of Mood States and the Multiple Affect Adjective Checklist; however, they focus specifically on maladaptive affect rather than covering the full range of emotional experience, and they lack subscales for some basic emotions such as disgust. 26 Therefore, the DEQ was chosen for the current study. However, the DEQ has not been used before in the context of a medical condition as the trigger of emotions. Previous research has been done in healthy populations who were exposed to different situations, such as reading about specific news or scenarios, or seeing specific images, 26 on subjects who made virtual visits to relatives admitted to Intensive Care Units during the COVID-19 pandemic, 28 and on surfers exposed to a series of images from the International Affective Picture System who, besides, underwent brain functional magnetic resonance imaging. 27 In these studies, mean values for the different emotions assessed were not provided. The DEQ has previously been used in a short study of 10 patients with chronic cough associated with a neurological disorder (cerebellar ataxia with neuropathy and bilateral vestibular areflexia [CANVAS] syndrome). 35 In that study, the DEQ domains most affected by chronic cough were anxiety and anger, with main scores of 3.2 and 2.9, a finding that is consistent with the results of the current study in patients with RCC/UC.
Increasing cough severity and the presence of cough-related SUI (overall population and female subgroup) were independently associated with higher scores for negative emotions (anger, anxiety, disgust, fear, and sadness) and for the desire subscale, while male gender was associated with higher happiness subscale scores. This is consistent with a previous analysis of the study, which found that increasing cough severity was associated with poorer cough-related QoL. 30 It is also consistent with a subgroup analysis of female participants, which found that the presence of cough-related SUI was associated with lower QoL. 31 Of note, the presence of SUI was more frequent in women and showed a strong and consistent association with negative emotional responses, equivalent to increments of 20–40 mm in cough severity VAS in the multivariate analysis. This finding may indicate a meaningful pathway linking physical impairment with emotional distress, particularly in women. We did not find an impact of age, gender, or cough duration on negative emotional responses, suggesting that cough severity and its physical consequence of SUI are the main drivers for emotional impairment.
The study has several limitations, including those inherent to observational studies, such as potential selection bias, lack of a control group, and incomplete/missing data. Patients were recruited from hospital outpatient clinics, which may have meant they had more severe symptoms and thus do not reflect the wider RCC/UCC patient population. Different pieces of information were collected directly from patients and did not undergo source verification, which may affect data integrity; however, it means that the results directly reflect patients’ perceptions of their condition and the emotions they experience. Some diagnoses, such as RCC/UCC or SUI, relied on already available diagnostic tests and clinical judgment; there were no additional diagnostic tests performed for this study for confirmation. Results of comparisons between subgroups should be interpreted with caution as the sample size was selected based on describing the overall population rather than subgroups, and there was an imbalance in the number of men and women, and in the number included with RCC and UCC. One additional limitation is that, to date, there has been limited use of the DEQ to assess the emotional impact of situations related to medical conditions, and no cut-off scores or minimal clinically important differences have been established. Additional studies involving interventions for cough would be needed to establish these values.
Conclusion
In patients with RCC/UCC, bouts of cough were found to trigger negative emotions such as anger, anxiety, disgust, fear, and sadness, as evaluated using a validated questionnaire. Results were similar for RCC and UCC. Increasing cough severity and the presence of SUI were independently associated with higher (worse) scores for negative emotions.
Supplemental Material
sj-docx-1-tar-10.1177_17534666251374853 – Supplemental material for Emotions in patients with refractory or unexplained chronic cough: a multicenter, non-interventional study
Supplemental material, sj-docx-1-tar-10.1177_17534666251374853 for Emotions in patients with refractory or unexplained chronic cough: a multicenter, non-interventional study by Ebymar Arismendi, Luis Puente-Maestu, Christian Domingo, Ignacio Dávila, Santiago Quirce, Marta Sánchez-Jareño and Luis Cea-Calvo in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-2-tar-10.1177_17534666251374853 – Supplemental material for Emotions in patients with refractory or unexplained chronic cough: a multicenter, non-interventional study
Supplemental material, sj-docx-2-tar-10.1177_17534666251374853 for Emotions in patients with refractory or unexplained chronic cough: a multicenter, non-interventional study by Ebymar Arismendi, Luis Puente-Maestu, Christian Domingo, Ignacio Dávila, Santiago Quirce, Marta Sánchez-Jareño and Luis Cea-Calvo in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-3-tar-10.1177_17534666251374853 – Supplemental material for Emotions in patients with refractory or unexplained chronic cough: a multicenter, non-interventional study
Supplemental material, sj-docx-3-tar-10.1177_17534666251374853 for Emotions in patients with refractory or unexplained chronic cough: a multicenter, non-interventional study by Ebymar Arismendi, Luis Puente-Maestu, Christian Domingo, Ignacio Dávila, Santiago Quirce, Marta Sánchez-Jareño and Luis Cea-Calvo in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-4-tar-10.1177_17534666251374853 – Supplemental material for Emotions in patients with refractory or unexplained chronic cough: a multicenter, non-interventional study
Supplemental material, sj-docx-4-tar-10.1177_17534666251374853 for Emotions in patients with refractory or unexplained chronic cough: a multicenter, non-interventional study by Ebymar Arismendi, Luis Puente-Maestu, Christian Domingo, Ignacio Dávila, Santiago Quirce, Marta Sánchez-Jareño and Luis Cea-Calvo in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
The Discrete Emotions Questionnaire was developed by C. Harmon-Jones, B. Bastian, and E. Harmon-Jones from the University of New South Wales, Sydney, and the University of Melbourne, Australia. We thank the authors for providing consent to use the questionnaire for this study. Professional medical writing assistance was provided by Kathy Croom and David P. Figgitt, PhD, CMPP™, on behalf of Content Ed Net (Madrid, Spain) with funding from MSD Spain.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.