
Abstract
Background:
Chronic cough (CC) affects about 10% of adults, but opioid use in CC is not well understood.
Objectives:
To determine the use of opioid-containing cough suppressant (OCCS) prescriptions in patients with CC using electronic health records.
Design:
Retrospective cohort study.
Methods:
Through retrospective analysis of Midwestern U.S. electronic health records, diagnoses, prescriptions, and natural language processing identified CC – at least three medical encounters with cough, with 56–120 days between first and last encounter – and a ‘non-chronic cohort’. Student’s t-test, Pearson’s chi-square, and zero-inflated Poisson models were used.
Results:
About 20% of 23,210 patients with CC were prescribed OCCS; odds of an OCCS prescription were twice as great in CC. In CC, OCCS drugs were ordered in 38% with Medicaid insurance and 15% with commercial insurance.
Conclusion:
Findings identify an important role for opioids in CC, and opportunity to learn more about the drugs’ effectiveness.
Introduction
Chronic cough (CC), with symptoms of more than 8 weeks, 1 affects about 10% of adults and is one of the most common reasons for ambulatory clinical encounters. 2 Although many patients undergo diagnostic testing, clinicians will commonly treat CC empirically, 3 especially with drugs for gastroesophageal reflux disorder, asthma, or upper airway cough syndrome. 4 Despite an evolving evidence-based approach to diagnosis and treatment, many patients end up trying home remedies or even prescribed cough suppressants, such as opiates. 5 At the start of the twentieth century, the Bayer Company even marketed Heroin for cough caused by a variety of infectious pulmonary diseases. 6 Evidence supporting the efficacy and safety of opiates for treating CC, however, is sparse; only a small number of studies have been conducted, with inconsistent results. 7 Today, the opioid drug crisis is well established. Despite legitimate uses of opioid drugs for pain, cough, and diarrhea, 8 the drugs have fueled substance use disorder and led to numerous overdoses and deaths.9,10 In the United States, the prevalence of past-year opioid use is about 4.7%. 11
Although opioid drugs continue to be used as antitussives, the use of opioids in cohorts of patients with CC is not well understood, especially since identifying such cohorts in administrative data or medical records is difficult. Electronic health records often under-code symptoms such as cough, and CC itself has no diagnostic code. To our knowledge, characteristics of patients with CC who are prescribed with opioid-containing cough suppressants (OCCS) have not been reported. Identifying such characteristics can help in estimating healthcare burden due to opioids in this population, and in developing better treatment strategies. The objective of this study was to use electronic health records to characterize the use of OCCS in a large cohort of patients with CC.
Methods
Study design
Data in this retrospective cohort study came from medical records and a health information exchange established for about 20 years in central Indiana. Part of a regional health information exchange among multiple institutions, the Indiana Network for Patient Care (INPC) contains more than 12 billion data elements, representing over 100 hospitals in 38 health systems, with more than 40,000 providers and 13.5 million patients. In the current study, patients’ INPC encounters were identified from Eskenazi Health and Indiana University Health, representing diverse socioeconomic and clinical backgrounds. Eskenazi Health is a tax-supported health system serving a predominantly urban region of central Indiana; Indiana University Health is a large academic medical institution with sites of clinical care across the state.
Inclusion criteria were all patients of at least 18 and less than 86 years of age at the time of a clinical encounter or medication prescription, who received care at Eskenazi Health or Indiana University Health between October 2005 and September 2015. The upper age limit was chosen because a CC that develops after this age may stem from an atypical cause.12,13 Using an approach previously reported, 14 cough was identified when the natural language processing tool nDepth found evidence of cough, 15 when a diagnostic code (ICD-9 code 786.2 or ICD-10 code R05) indicated cough, or when benzonatate or dextromethorphan was prescribed in the outpatient setting, according to the National Drug Code.
When an encounter with cough occurred between 1 October 2005 and 30 September 2015, and at least two additional encounters with cough occurred such that the gap between the first and third encounters was 56–120 days, the patient was defined as having CC, and the index date was defined as date of the first encounter. For other participants, with cough but not CC (‘non-CC’), the index date was defined as the first encounter date with cough between 1 October 2005 and 30 September 2015. 14 The use of 120 days as the maximum ‘gap’ between first and third encounter for patients with cough increases the chance that the three cough encounters shared a common etiology. 14 Patients without at least two encounters spanning at least 8 weeks were excluded, as were patients prescribed with angiotensin-converting enzyme inhibitors in the year prior to the index date. A ‘non-chronic cohort’ was defined as having at least one encounter with cough, but not meeting criteria for CC.
Outcomes
Antitussive and opioid drugs are listed in the Supplemental Material Note. Drug prescriptions were captured by name from the dataset. An order is an event of prescribing. OCCS were defined as drugs containing codeine, dihydrocodeine, or hydrocodone. Antitussive drugs were defined as OCCS, or cough suppressants without opioids. Descriptive statistics identified the cohort’s age, gender, race, primary insurance, and prescriptions of opioids. Demographic comparisons were made to the non-CC cohort using Student’s t-test or Pearson’s chi-square test as appropriate. Multivariable modeling of number of prescriptions was conducted using zero-inflated Poisson models. Patients with unknown genders were excluded.
Results
Compared to non-CC (N = 229,538 patients), the CC cohort (N = 23,210) had more women (66% versus 61%) and Medicare insurance (36% versus 24%), and was older (mean age 54 versus 48 years) and more white (72% versus 69%). Numbers of patients in both cohorts increased from ages 18 to 19 (N = 9085) through ages 50 to 59 (N = 49,936), and then decreased (20–29: N = 36,331; 30–39: N = 38,267; 40–49: N = 45,566; 60–69: N = 38,843; 70–79: N = 24,951; 80–85: N = 9769). The CC cohort had 17% African-Americans, 31% commercial insurance, and 19% Medicaid insurance. Characteristics of patients with CC or non-CC are summarized in Supplemental Material Table 1. The median number of encounters for CC patients was 85 (range: 45–151), with a median follow-up period of 2.23 years (range: 1.23–4.25 years). For non-CC patients, the median number of encounters was 39 for the non-CC patients (range: 18–78) over a median follow-up period of 7.70 years (range: 5.04–10.98 years).
Among both cohorts combined, commonly prescribed antitussive or opioid drugs included acetaminophen/hydrocodone (34% of prescriptions), fentanyl (18%), morphine (9.8%), tramadol (4.2%), codeine/guaifenesin (4.1%), and acetaminophen/oxycodone (3.2%). Among prescriptions in the CC cohort, 31% contained hydrocodone; 6.5% of these contained a decongestant, expectorant, or antihistamine (chlorpheniramine, dexchlorpheniramine, diphenhydramine, guaifenesin, phenylephrine, or pseudoephedrine). In the first year after the index date, OCCS prescriptions represented 71% of 18,343 antitussive orders (Supplemental Material Table 2) and 21% of patients (versus 7% of those with non-CC). Among these patients, 34% had at least three OCCS prescriptions. In the CC cohort, OCCS drugs were ordered by 38% with Medicaid insurance, 18% with Medicare insurance, and 15% with commercial insurance. The number of OCCS prescriptions per 100 patients was 56 for CC (total of 15,274) versus 14 for non-CC. Within 1 year after the index date, the median time between first and last prescription of an opioid was 125 days for the non-CC and 175 days for CC (p < 0.001). More than ten OCCS prescriptions were ordered for 125 (0.5%) of the CC patients. Figure 1 shows the number of OCCS prescriptions for the CC cohort, by year.
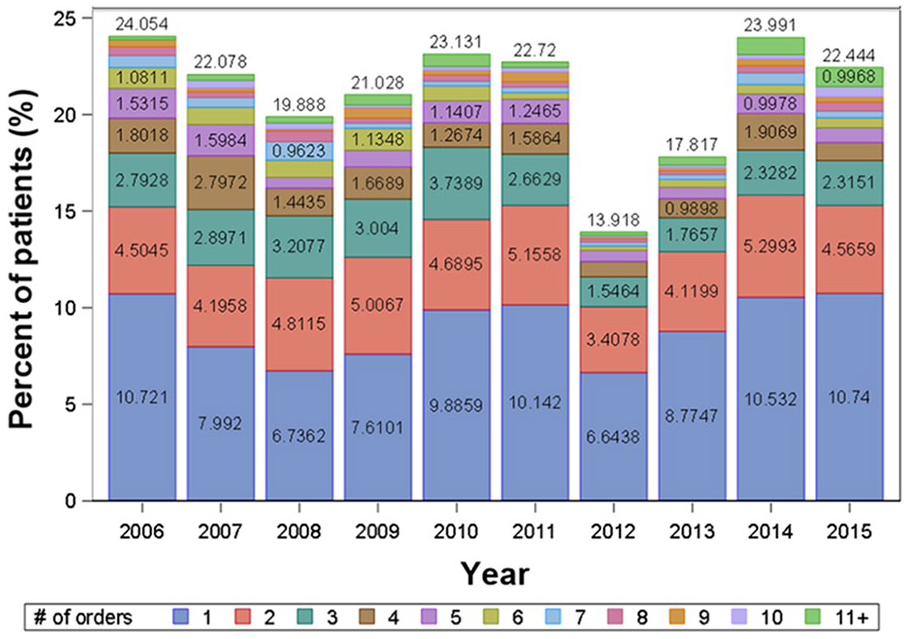
Opioid-containing cough suppressant (OCCS) prescriptions for patients with chronic cough, by year and number of prescription orders. OCCS drugs were prescribed in 21% of patients.
Multivariable modeling of OCCS is shown in Table 1. Adjusting for cohort, age, race, gender, urbanicity, insurance, and year, patients were more likely to have at least one OCCS prescription if they had CC [odds ratio (OR) 2.0 compared to non-CC], were non-white (OR 1.4), lived in an urban area (OR 1.2), or had Medicaid insurance (OR 2.8) or self-pay (OR 1.4, compared to commercial insurance). More OCCS orders occurred in patients with CC (1.8 times more than non-CC), Medicare insurance (1.2 times more), Medicaid insurance (1.6 times more), or self-pay status (1.3 times more).
Multivariable models for opioid-containing cough suppressants.
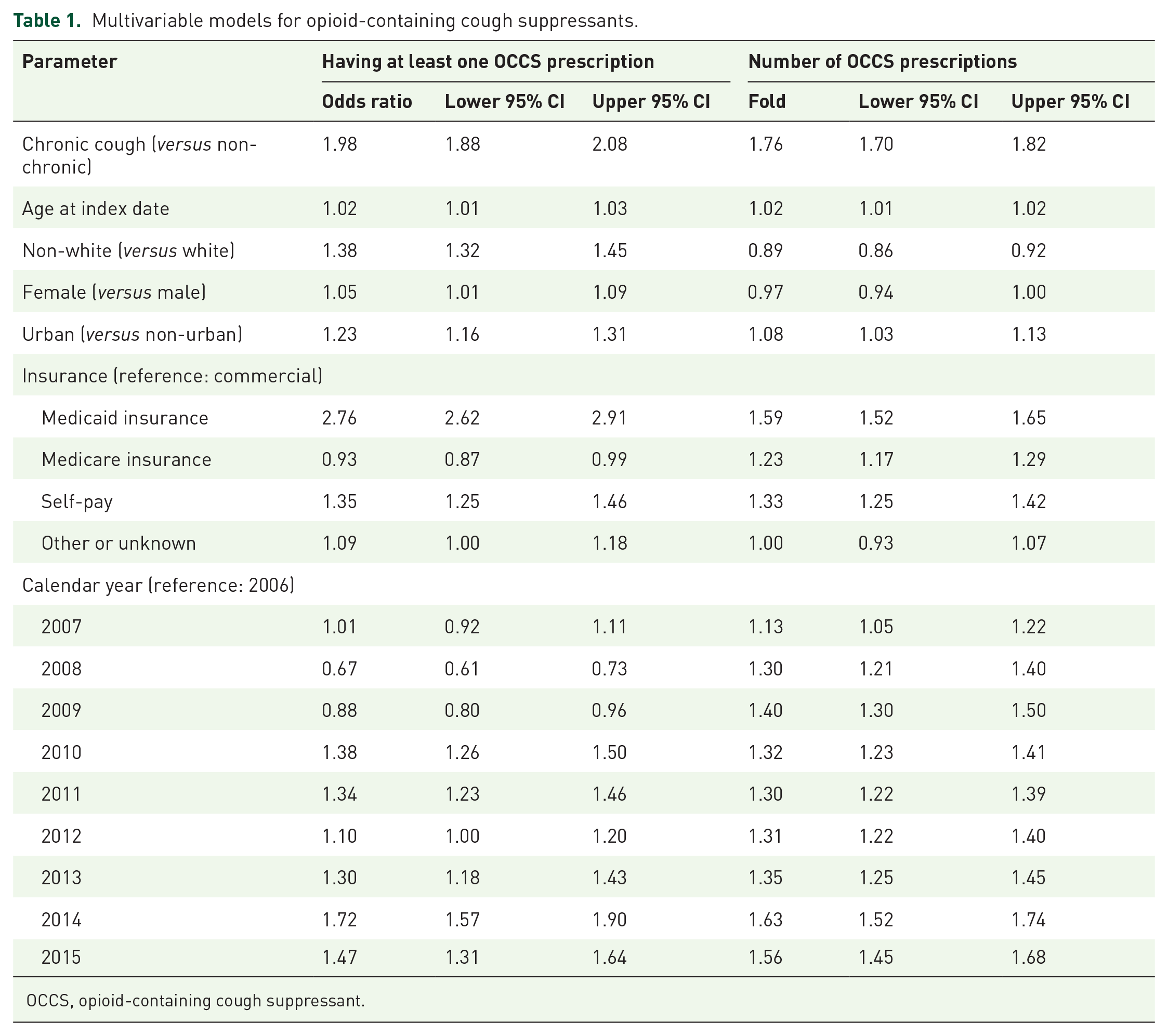
OCCS, opioid-containing cough suppressant.
Discussion
To our knowledge, the current study – one of the largest CC cohorts reported – is the first to characterize a cohort of CC and non-CC regarding OCCS prescriptions. About one in five patients with CC received an OCCS prescription. Although over one-third of these had at least three such prescriptions, more than ten OCCS prescriptions were ordered for just 0.5% of patients with CC, indicating that OCCS is not used as chronic therapy in most cases. As such, opioid abuse among patients with large numbers of prescriptions may occur in a small subset of patients with CC.
Despite a minority of patients with CC receiving OCCS, these drugs played an important role. In adjusted analyses, the odds of an OCCS prescription were twice as high in the CC cohort as compared to those with non-CC. Other opioids have also shown importance for CC elsewhere. In a clinical trial of 27 patients who previously failed antitussive therapy and were then randomized to receive 4 weeks of slow-release morphine sulfate or a placebo, Morice et al. 16 reported that morphine was effective in significantly reducing severity of CC according to daily cough scores. Along with codeine, tramadol has a role in treating neurologic causes of cough including post-viral vagal neuropathy, though CC in most patients receiving OCCS in this study likely had other etiologies.
Although only 6.5% of prescriptions with hydrocodone contained a decongestant, expectorant, or antihistamine, the strong association between CC and OCCS suggests the possibility that additional factors may be involved, such as unmeasured confounders including pain syndromes. Mental health issues have been linked with both pain and cough.17,18 Overuse of opioids can complicate other medical conditions and even lead to cough. For example, asthma and bronchitis, which can cause cough, have been speculated to be occasional complications of opiate use.19,20 Oliver et al. 21 reported, from a primary care database of 275,151 adults with asthma, that higher usage of inhaled corticosteroids or oral prednisolone was seen among those with a history of opioid use disorder. Similarly, Mehta et al. 22 found that prescription of methadone was a smoking-independent predictor of chronic obstructive pulmonary disease and asthma. Including data about a drug’s indication may enhance studies of this kind.
Low-income patients were more likely than others to have OCCS prescriptions in both unadjusted and adjusted analyses. This finding might reflect multiple factors, such as the possibility of a greater burden of pain among low-income patients, 23 as well as insurance plans and drug formularies that cover the bulk of the costs of many prescribed medications, including opioids. Studies of prior authorization for formulary-restricted drugs have drawn links between prescribing patterns and insurance coverage. 24 Complex roles of multimorbidity in the prescribing of OCCS warrant greater attention. The trend of a longitudinal increase in prescribing of OCCS drugs might reflect greater availability of drugs, changes to clinical awareness of diagnosis or treatment, the opioid crisis, or other factors.
This study has limitations inherent to retrospective designs. Some patients with CC may have been missed if they had infrequent medical encounters or were lost-to-follow up, and some details of cough may have been absent from medical records. Available data were limited to the health information exchange, and some medical encounters and prescribing may have occurred outside the institutions represented. Thus, selection bias may limit ascertainment of cases and affect results. Some of the longitudinal changes seen in drug usage may reflect variations in the availability of drug data from year to year, but the available data still provide a basis to understand the floor or minimum volume of drug usage. More recent data might show different results. Different definitions of CC and non-CC may yield different results. The study does not assess the indications for prescribed drugs, or the appropriateness of the drugs and their doses; it also does not attribute any effects to specific causes.
Conclusion
In summary, in a cohort of 23,210 patients with CC, about one in five patients with CC received an OCCS prescription, and the odds of an OCCS prescription were twice as great in CC as compared to non-CC. To our knowledge, this is the first report of characteristics of patients with CC who are prescribed with OCCS. In the face of an ongoing opioid crisis, the magnitude of OCCS prescriptions underscores the need for more effective non-opioid drugs to treat CC, and more effective implementation of diagnostic strategies to determine a cough’s cause. At the same time, the findings identify an important role for opioids in CC, and an opportunity to learn more about the drugs’ effectiveness.
Supplemental Material
sj-docx-1-tar-10.1177_17534666241259373 – Supplemental material for Prescriptions of opioid-containing drugs in patients with chronic cough
Supplemental material, sj-docx-1-tar-10.1177_17534666241259373 for Prescriptions of opioid-containing drugs in patients with chronic cough by Michael Weiner, Ziyue Liu, Jonathan Schelfhout, Paul Dexter, Anna R. Roberts, Ashley Griffith, Vishal Bali and Jessica Weaver in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-2-tar-10.1177_17534666241259373 – Supplemental material for Prescriptions of opioid-containing drugs in patients with chronic cough
Supplemental material, sj-docx-2-tar-10.1177_17534666241259373 for Prescriptions of opioid-containing drugs in patients with chronic cough by Michael Weiner, Ziyue Liu, Jonathan Schelfhout, Paul Dexter, Anna R. Roberts, Ashley Griffith, Vishal Bali and Jessica Weaver in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
We would like to thank Melissa R. Thomas and Steve Becraft for their careful review of the manuscript. Parts of this work were presented at the CHEST Annual Meeting, New Orleans, Louisiana, on 23 October 2019.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.