
Abstract
Background:
It has been shown that asthma is potentially linked to a higher risk of cardiovascular disease (CVD) and cardiovascular mortality (CVM).
Objectives:
This study aims to systematically review and summarize epidemiological evidence on the relationship between asthma and these cardiovascular outcomes.
Design:
Systematic review and meta-analysis.
Data sources and methods:
This meta-analysis, registered with PROSPERO (CRD 42024576126), utilized data from PubMed, Embase, the Cochrane Library, and references from included studies. The search covered literature from the inception of these databases until July 17, 2024. We included observational studies examining the link between asthma and CVD and CVM. Bias risk was evaluated using the Newcastle–Ottawa Quality Assessment Scale (NOS). We calculated pooled relative risk (RR) with a 95% confidence interval (CI) using a random-effects model.
Results:
A total of 29 studies encompassing 11,380,027 participants were included. The overall risk for CVD in asthma patients was 1.30 (95% CI: 1.20–1.42). Specific CVD risks were elevated for coronary heart disease (CHD, RR 1.35; 95% CI: 1.27–1.42), angina pectoris (AP, RR 1.48; 95% CI: 1.16–1.89), myocardial infarction (MI, RR 1.33; 95% CI: 1.25–1.41), and heart failure (HF, RR 1.53; 95% CI: 1.04–2.23). Asthma was also associated with a higher risk of CVM (RR 1.26; 95% CI: 1.05–1.51).
Conclusion:
Asthma is associated with a higher risk of developing CVD, including specific types such as CHD, AP, MI, and HF. In addition, asthma patients face an increased risk of cardiovascular mortality compared to non-asthmatics.
Plain language summary
Why was the study done? Researchers have noticed that people with asthma might be at a higher risk of developing heart problems and dying from heart-related issues. This study aimed to gather and review existing research to better understand how asthma is connected to these serious health risks. What did the researchers do? The researchers reviewed data from studies that looked at the relationship between asthma and heart disease. They analyzed information from 30 studies, including over 11 million people, to see if having asthma increases the likelihood of developing heart disease or dying from it. They also examined whether factors like gender or smoking habits affect this risk. What did the researchers find?
The study found that people with asthma have a 32% higher risk of developing heart disease compared to those without asthma. This risk is even higher for women, smokers, and those with specific types of heart conditions such as coronary heart disease, angina, heart attacks, heart failure, and atrial fibrillation. Additionally, people with asthma are 26% more likely to die from heart-related issues than those without asthma. What do the findings mean? The findings suggest that having asthma can increase the risk of heart disease and heart-related death. This highlights the importance of monitoring heart health in people with asthma and considering these risks in their overall care and treatment plans.
Introduction
Asthma is a chronic inflammatory disease of the airways, characterized by airway hyperresponsiveness, intermittent airflow obstruction that can become persistent over time, and airway remodeling. 1 With over 300 million individuals affected globally, asthma’s prevalence continues to rise, imposing a significant economic and health burden on societies worldwide.2,3 Despite considerable advancements in understanding its molecular etiology, pathological mechanisms, and therapeutic approaches, asthma control and prognosis remain suboptimal.4 –6 Furthermore, asthma is frequently associated with a range of comorbidities, including diabetes mellitus, hypertension, obesity, chronic kidney disease, depression, and CVD. 7
The prevalence of CVD has been steadily increasing, and this trend is expected to persist in the coming decade, highlighting the growing public health challenge posed by cardiovascular conditions.8,9 CVD often results in severe clinical outcomes, necessitating heightened focus and intervention. 10 Previous studies have identified both pathological and etiological connections between asthma and cardiovascular disease.11,12 Given the implications for clinical practice, understanding cardiovascular risk among asthma patients is crucial. Although existing research suggests an association between asthma and an elevated risk of CVD and CVM, the precise relationship between asthma and specific cardiovascular conditions—such as myocardial infarction, angina, and heart failure—remains inadequately defined.
Hence, we aimed to conduct a systematic review and meta-analysis of observational studies to examine the association between the risk of cardiovascular disease and mortality in individuals with asthma.
Methods
Protocol registration and guidelines
The reporting of this study conforms to the PRISMA statement. 13 The protocol was pre-registered in the International Prospective Register of Systematic Reviews (PROSPERO) platform under the registration number CRD 42024576126.
Data sources and searches
A comprehensive search was conducted in three medical databases (PubMed, Cochrane Library, and Embase) for articles published from database inception to July 17th, 2024. The search strategy combined medical subject headings (MeSH) and keywords, without any language restrictions. Details of the search strategy are provided in Table S1. Furthermore, the reference lists of included observational studies and other published meta-analyses were scrutinized to identify additional relevant trials.
Eligibility criteria
The inclusion criteria for the meta-analysis required that the studies employed a cohort study design, with the case group consisting of asthma patients and the control group comprising individuals without asthma. Moreover, the studies were required to focus on endpoints related to the occurrence of CVD and CVM. In addition, eligible studies had to provide hazard ratio (HR), risk ratio (RR), or odds ratio (OR) with a corresponding 95% confidence interval (CI).
Conversely, studies were excluded if the population consisted solely of non-asthmatic individuals, if the design was case–control or cross-sectional, or if the endpoints did not include CVD or CVM. Studies were also excluded if they did not provide HRs, RRs, or ORs, or if such measures could not be calculated. In addition, letters, case reports, and conference abstracts were excluded from the analysis.
Study selection
Two reviewers (JYY and SYZ) independently screened the literature based on the eligibility and exclusion criteria. Duplicate and irrelevant articles were initially excluded based on their titles and abstracts. Subsequently, they categorized the remaining records as either included, excluded, or uncertain. The full texts of potentially eligible articles were then downloaded and reviewed to identify all eligible studies. Any discrepancies were resolved through discussion with the third reviewer (HXQ).
Data extraction
Two reviewers (JYY and SYZ) independently evaluated the eligibility of studies according to predetermined inclusion and exclusion criteria. We extracted key data, including the first author, year of publication, study type, sample size, follow-up duration, age, diagnostic criteria, and adjusted confounders from each included article. For cohort studies, we extracted the hazard ratio (HR), relative risk (RR), or odds ratio (OR) along with their 95% confidence intervals.
Study quality
For cohort studies, the Newcastle–Ottawa Quality Assessment Scale (NOS) was employed to assess the quality of the included studies. 14 We assessed various components of each study, including participant selection, measurement of exposure, comparability, assessment of outcomes, and adequacy of follow-up. For each study, scores were assigned to categories of risk of bias: low (0–3), moderate (4–6), and high (7–9), with a higher number of stars reflecting superior study quality.
Statistical analysis
Summary statistics for RR with a 95% CI are presented. For studies that did not report RR data, OR or HR was converted into RR. The OR data were converted to RR using the formula RR = OR/(1 − p0 + p0 × OR) when the outcome occurred in less than 10% of the sample, with p0 representing the outcome incidence in the entire study population. 15 For outcomes with a frequency greater than 10%, the square root transformation of the OR was applied, as recommended. 16 The HR was transformed into RR using the following formula: RR = (1 − e^(HR×ln(1 − r)))/r, where r represents the event rate for the reference group. 17 We utilized Stata statistical software version 14.0 (Stata Corp, College Station, TX, USA) to calculate the pooled RR with 95% CIs, aiming to evaluate the relationship between asthma and CVD or CVM using a random-effects model. Potential publication bias was assessed through visual evaluation of a funnel plot and verified using Egger’s test. We conducted subgroup analyses based on specific types of CVD, gender, study type, region, and diagnostic criteria for asthma. We also conducted meta-regression analyses to investigate possible causes of heterogeneity across studies.
Results
Search result
The literature search yielded 19,917 relevant records, of which 1244 duplicates were removed. Following the screening of titles and abstracts, 18,607 records were excluded for irrelevance to the topic. Finally, the full texts of 67 records were reviewed, of which 29 studies18 –46 were ultimately included. The study selection process is illustrated in the PRISMA flowchart shown in Figure S1.
Study characteristics
A total of 29 studies, involving 11,380,027 individuals, were included. Of these, 22 studies18 –39 investigated overall and specific types of CVD, with study populations mainly from the Americas (n = 9), Asia (n = 4), Europe (n = 8), and Australia (n = 1). In addition, 10 studies18,20,29,40 –46 focused on CVM, primarily including populations from Asia (n = 2), Europe (n = 7), and Australia (n = 1). Adjusted confounders varied slightly across studies, with age, gender, and race being the most commonly adjusted variables. The study characteristics are summarized in Table 1.
Characteristics of included studies.

CVD, cardiovascular disease; ICD, International Classification of Diseases; OPCS-4, Surveys Classification of Interventions and Procedures coding systems; UKB, UK Biobank.
Quality assessment
In all, 25 of the 29 studies were rated as high quality, and four were rated as moderate quality according to the NOS criteria. This demonstrates the predominance of high-quality studies in this meta-analysis. The risk of bias scores is provided in Table S2.
Asthma and risk of overall type of CVD
A total of 22 cohorts18 –39 examined the risk of overall type of CVD in asthma patients. The pooled analysis revealed a significantly increased risk of overall type of CVD among asthma patients (RR = 1.30, 95% CI (1.20, 1.42), I² = 97.0%, Figure 1). Given the substantial heterogeneity observed, a sensitivity analysis was conducted to identify potential sources. The sensitivity analysis indicated that none of the individual studies significantly influenced the pooled effect size, confirming the consistency and robustness of the results (Figure S2). The funnel plot suggested the possibility of publication bias (Figure S3). Egger’s test (p = 0.559) revealed no significant publication bias.

Forest plot for the risk of overall type of CVD in asthma.
Asthma and risk of specific types of CVD
A total of 15 studies18,20 –22,24 –30,32 –34,38 evaluated the risk of specific types of CVD in patients with asthma. The pooled analysis revealed a substantially increased risk of CHD (RR = 1.35, 95% CI (1.27, 1.42), I² = 81.2%, Figure 2), AP (RR = 1.48, 95% CI (1.16, 1.89), I² = 77.4%, Figure 3), MI (RR = 1.33, 95% CI (1.25, 1.41), I² = 64.0%, Figure 3), and HF ( RR = 1.53, 95% CI (1.04, 2.23), I² = 99.0%, Figure 3) among individuals with asthma.

Forest plot for the risk of CHD in asthma.

Forest plot for the risk of a specific type of CVD in asthma.
Asthma and risk of CVM
A total of 10 studies18,23,29,40 –46 evaluated the risk of CVM among asthma patients. Compared with the non-asthmatic group, the risk of subsequent CVM was significantly higher in the asthmatic population (RR = 1.26, 95% CI (1.05, 1.51), I² = 98.5%, Figure 4). The sensitivity analyses in asthma and CVM demonstrated that the pooled results were stable after individually eliminating each study (Figure S4). The funnel plot suggested the possibility of publication bias (Figure S5). Egger’s test (p = 0.841) revealed no significant publication bias.
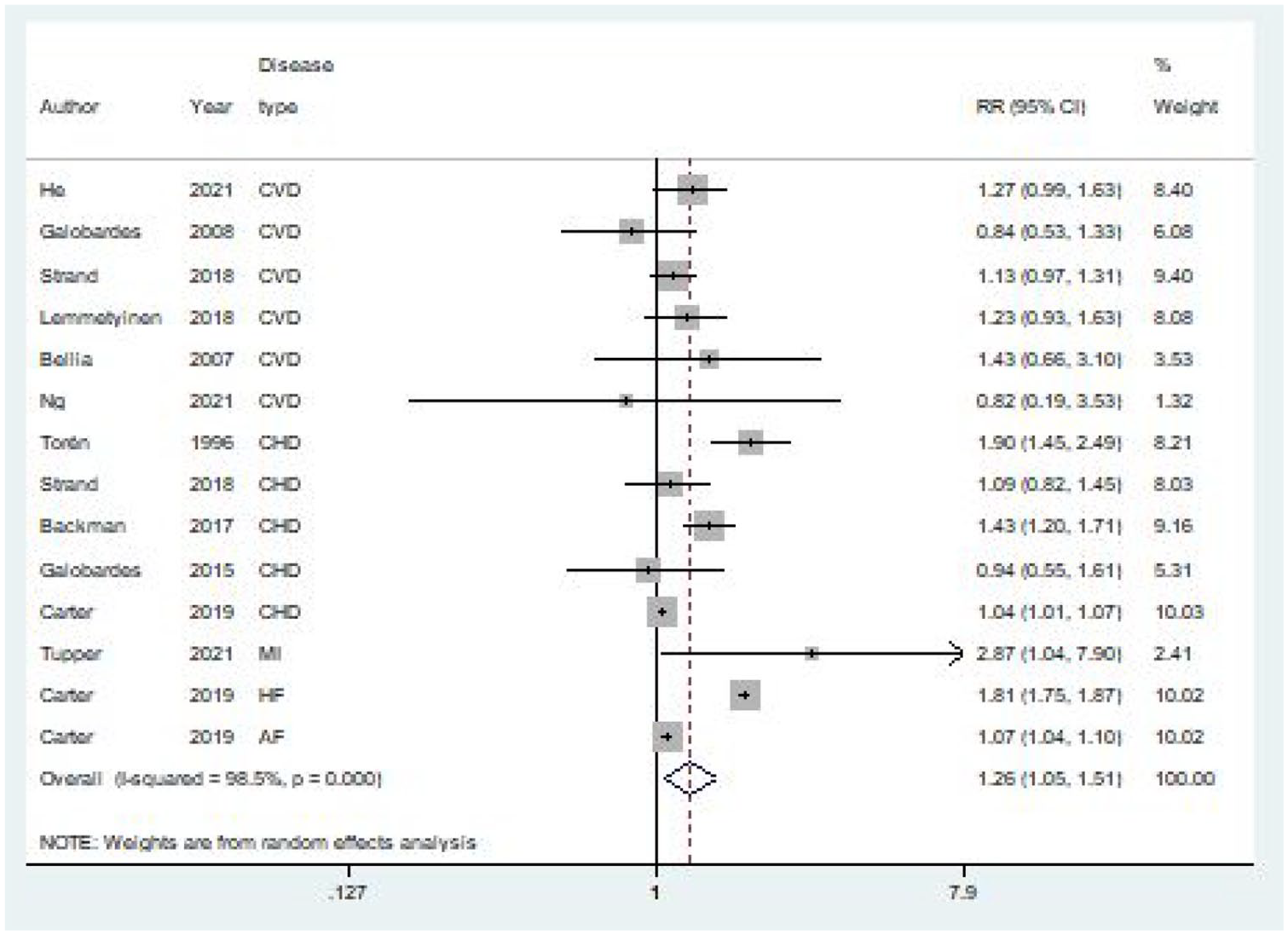
Forest plot for the risk of specific types of CVM in asthma.
Moderators of CVD
Meta-regression analyses were conducted to assess the relationship between individual moderators (predictive factors) and the pooled effect size (risk of CVD). Among the six moderators, the diagnostic criteria for asthma in study participants was identified as a significant risk factor for CVD. The Test of Moderators revealed statistical significance (p < 0.05; Table S3). This indicates that the predictive factor—the diagnostic criteria for asthma—was indeed associated with the effect sizes of the studies.
Subgroup analysis
In the subgroup analysis, females (RR = 1.57, 95% CI (1.24, 1.97), I² = 97.5%, Figure S6), with a history of asthma, exhibit a slightly higher risk of cardiovascular disease (CVD) compared to males (RR = 1.41, 95% CI (1.07, 1.85), I² = 98.1%, Figure S6). In various study designs, the retrospective cohort study (RR = 1.33, 95% CI (1.17, 1.53), I² = 98.2%, Figure S7) and the prospective cohort study (RR = 1.28, 95% CI (1.19, 1.37), I² = 78.5%, Figure S7) yielded similar results, both indicating an increased risk of CVD in asthma. Furthermore, in regional studies, we found that the risk of CVD in asthmatic patients in Asia (RR = 1.45, 95% CI (1.33, 1.58), I² = 90.1%, Figure S8) was higher than in Europe (RR = 1.24, 95% CI (1.10, 1.38), I² = 95.1%, Figure S8) and the Americas (RR = 1.31, 95% CI (1.07, 1.61), I² = 97.2%, Figure S8). In addition, based on the results of meta-regression, we performed a subgroup analysis comparing effect sizes according to the diagnostic criteria for asthma (Figure S9). The pooled RR for studies in which the diagnostic criteria for asthma were based on ICD was 1.40 (95% CI, 1.25, 1.57), while the pooled RR for studies with other diagnostic criteria for asthma was 1.21 (95% CI, 1.13, 1.29; Table 2).
Subgroup analysis for the risk of CVD in patients with asthma.

CVD, cardiovascular disease.
Discussion
Main findings
This meta-analysis of 29 cohort studies involving 11,380,027 individuals assessed the link between asthma and CVD or CVM. It found a 1.30-fold increase in overall CVD risk among asthma patients, with a 1.41-fold increase in men and a 1.57-fold increase in women. Asthma patients showed a 1.48-fold increased risk of angina pectoris, a 1.33-fold increased risk of myocardial infarction, and a 1.53-fold increased risk of heart failure. The risk of cardiovascular mortality was also notably higher in asthma patients. These findings offer clinicians updated evidence to focus on these specific cardiovascular risks in asthma patients.
Interpretation of findings
Asthma is a widespread chronic inflammatory airway disease that can cause systemic low-grade inflammation, contributing significantly to the development and progression of CVD. The interaction between asthma and CVD can lead to serious consequences. Previous meta-analyses have consistently reported a link between asthma and CVD. For example, Liu et al. 47 found a significant association between asthma and an increased risk of CHD based on seven cohort studies. Hua et al. 48 reported that asthma notably raises the risk of four specific cardiovascular conditions—CAD, AF, HF, and MI—as well as cardiovascular mortality. Zhang et al. 49 highlighted that asthma patients face a higher risk of both all-cause mortality and CVD-related morbidity and mortality. Our analysis confirms and builds upon these findings by incorporating more recent studies and examining various types and subgroups of cardiovascular diseases. We found that asthma patients have a significantly elevated overall risk of CVD and CVM. Furthermore, our analysis shows a markedly increased risk of specific cardiovascular events in asthma patients, with heart failure presenting the highest risk. These results offer clinicians updated evidence to better identify and address these critical cardiovascular events in asthma patients.
The specific mechanisms by which asthma influences CVD remain unclear, though several theories have been proposed. It is well established that airway inflammation is central to asthma’s pathophysiology. Recently, there has been growing recognition of how airway inflammation can spill over into the systemic circulation in asthma. Chronic airway inflammation may lead to systemic inflammation, exposing the vascular system to inflammatory mediators from the lungs. 50 Inflammatory cytokines associated with asthma, such as IL-1, IL-6, and TNF-α, can stimulate the release of matrix metalloproteinases, which degrade elastin and collagen, weakening the elastic fibers in the vascular layers. 51 This degradation contributes to the migration of monocytes and smooth muscle cells to atherosclerotic plaques, creating a vicious cycle that undermines plaque stability and may lead to plaque rupture. Chronic inflammation also increases the expression of osteogenic markers in vascular smooth muscle cells (VSMCs), promoting their differentiation into osteoblasts. VSMCs can absorb phosphate, form bioapatite, and deposit it on the vascular wall, leading to medial vascular calcification and reduced vascular elasticity. 52 Recent studies suggest that anti-inflammatory drugs targeting IL-1 and TNF-α may help address vascular dysfunction and prevent cardiovascular events,53,54 highlighting the crucial role of inflammation in cardiovascular disease development. In addition, damaged airway epithelium in asthma patients leads to the secretion of reactive oxygen species (ROS) by eosinophils, neutrophils, and macrophages. 55 Excessive ROS disrupts the balance between endothelial cell proliferation and apoptosis, inducing endothelial dysfunction. This dysfunction promotes the leakage of low-density lipoprotein (LDL) into the vascular intima, where ROS oxidizes LDL into oxidized LDL (ox-LDL). Ox-LDL induces endothelial cells to produce cell adhesion molecules like VCAM-1 and ICAM-1, 56 facilitating the infiltration of inflammatory cells beneath the endothelial layer. This process releases interleukins and other pro-inflammatory cytokines, enhancing endothelial cell proliferation and migration, increasing lipid deposition on vessel walls, and contributing to atherosclerotic plaque formation, thereby elevating cardiovascular event risk.57,58 Moreover, asthma patients are at increased risk of obesity, reduced physical activity, and poor dietary habits, all of which are additional risk factors for cardiovascular disease.
In the subgroup analysis, both male and female asthma patients show a significantly increased risk of CVD. However, females with asthma have a slightly higher CVD risk compared to their male counterparts. Estrogen, known for its immune-enhancing properties, can amplify the type 2 inflammatory response by stimulating the release of T2 cytokines such as IL-4, IL-5, and IL-13.59,60 This increased systemic inflammation may partially explain the elevated CVD risk in females with asthma. In addition, we observed that asthmatic patients in Asia face a higher risk of cardiovascular disease (CVD) compared to their counterparts in Europe and the Americas. This discrepancy may be closely associated with factors such as unhealthy lifestyles, imbalanced diets, an aging population, and environmental pollution prevalent among the Asian population. 61 Asthmatic patients in Asia generally exhibit lower levels of control compared to their European and American counterparts,62 –64 which may also be associated with the heightened risk of CVD. 21 It is recommended that asthmatic patients in Asia place greater emphasis on asthma management and adopt healthier lifestyle practices. Following a meta-regression analysis, we identified that the diagnostic criteria for asthma could be a significant source of heterogeneity. Various studies utilized differing diagnostic criteria, which could significantly impact the effect size of the findings. Future research should aim to adopt standardized, unified diagnostic criteria to minimize the variability in results caused by discrepancies in diagnostic practices.
Strengths and limitations
In comparison to previous studies, this meta-analysis provides an updated integration of recent literature, demonstrating that asthma constitutes a significant risk factor for both overall and specific types of CVD and CVM. Meanwhile, the limited number of studies integrated into previous meta-analyses constrains the potential for comprehensive exploration. This report encompasses 29 studies identified through a systematic literature search, thereby enabling the provision of a more comprehensive summary estimate of the association between asthma, CVD, and CVM. The findings underscore the necessity for enhanced monitoring of CVD and CVM risk in patients with asthma. In addition, most of the included studies were of high quality, ensuring the reliability of the findings. However, limitations exist. First, substantial heterogeneity was identified, potentially due to differences in population characteristics across studies. For example, most studies focused on adults, whereas only one involved adolescents. Second, most studies have adjusted for different variables, but few have assessed or adjusted for the same factors. Consequently, the pooled results may be influenced by varying confounding factors across studies, thereby limiting the ability to draw reliable conclusions from the pooled data. Despite this, sensitivity analyses yielded consistent results, and random effects models were used to address the effects of heterogeneity. Nevertheless, a possible association between study heterogeneity and pooled effects cannot be disregarded. Third, it is important to recognize that variations in the definitions and assessment criteria of asthma and cardiovascular events across studies may complicate the interpretation of their relationship. Moreover, interrater agreement was not conducted for the screening process, only a pilot test of the screening was performed between raters.
Conclusion
In this systematic review and meta-analysis, asthma was identified as a significant risk factor for increased cardiovascular morbidity and mortality, including angina, myocardial infarction, and heart failure. This finding highlights the critical need for clinicians to remain vigilant about the elevated CVD and CVM risk in asthma patients and underscores the importance of early screening during clinical evaluations. In addition, further research is essential to strengthen these associations and elucidate the underlying etiologic mechanisms.
Supplemental Material
sj-doc-1-tar-10.1177_17534666251333965 – Supplemental material for Asthma and the risk of cardiovascular diseases and mortality: a meta-analysis of cohort studies
Supplemental material, sj-doc-1-tar-10.1177_17534666251333965 for Asthma and the risk of cardiovascular diseases and mortality: a meta-analysis of cohort studies by Yuyue Jiang, Xuqing Huang, Dongwei Yu, Changqing Xu, Yan Wang, Xi Wang and Yuezhong Shen in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-1-tar-10.1177_17534666251333965 – Supplemental material for Asthma and the risk of cardiovascular diseases and mortality: a meta-analysis of cohort studies
Supplemental material, sj-docx-1-tar-10.1177_17534666251333965 for Asthma and the risk of cardiovascular diseases and mortality: a meta-analysis of cohort studies by Yuyue Jiang, Xuqing Huang, Dongwei Yu, Changqing Xu, Yan Wang, Xi Wang and Yuezhong Shen in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.