
Abstract
Objective:
Nonalcoholic fatty liver disease (NAFLD) is considered as the hepatic manifestation of metabolic syndrome, sharing the similar cardiometabolic risk factors with cardiovascular disease (CVD). Whether NAFLD by itself is associated with increased cardiovascular events and death remain an issue to debate. This study aimed to further investigate the association between NAFLD and adverse CVD outcomes.
Methods:
Participants were followed up until the end of 2020 in current analysis. NAFLD is defined using fatty liver index (FLI). Cox proportional hazard model was used to analyze the association between NAFLD and all-cause mortality, major adverse cardiovascular events (MACEs), CVD mortality, fatal/nonfatal acute myocardial infarction (AMI), and fatal/nonfatal stroke. C-index was calculated to evaluate the model enhancement when adding NAFLD factor.
Results:
After screening the data of 502,492 participants in the original cohort, 215,245 eligible participants were included in this study for MACEs outcome. Compared with non-NAFLD participants, the multivariable adjusted hazard ratios of NAFLD group was 1.25 (1.14–1.36) for MACEs; 1.14 (1.08–1.20) for all-cause mortality; 1.61(1.42–1.82) for CVD mortality; 1.58(1.19–2.11) for AMI mortality; and 1.18 (0.85–1.64) for stroke mortality. When adding FLI, C-index of NAFLD model improved for all-cause mortality, MACEs, and CVD mortality compared with that in the traditional CVD risk factor model.
Conclusion:
NAFLD is an independent risk factor for all-cause mortality and adverse CVD outcomes. Based on the traditional CVD risk factor model, additionally screening NAFLD could improve the prediction efficiency for adverse CVD outcomes.
Keywords
Introduction
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disorder affecting approximately 25%–45% of the adult population in Europe and United States.1,2 NAFLD encompasses a histological spectrum ranging from simple steatosis to nonalcoholic steatohepatitis (NASH), and the latter is projected to become the leading indication for liver transplant in the United States by 2020. 3 Over the past decade, it has become increasingly clear that the hazard of NAFLD is not only confined to liver-related morbidity or mortality but also a multisystem disease that affects various extra-hepatic organs, including the cardiovascular system.4–7
NAFLD is generally considered as the hepatic manifestation of metabolic syndrome, sharing common cardiometabolic risk factors with cardiovascular disease (CVD). 8 Increasing studies indicated that NAFLD is an independent risk factor for CVD.9–12 Other studies have demonstrated that NAFLD was associated with subclinical atherosclerosis, 13 subclinical cardiovascular disease (CVD) outcomes, 14 clinically manifesting atherosclerosis, 15 vulnerable atherosclerotic plaque, and adverse outcome.16,17 However, data on whether NAFLD by itself is associated with increased cardiovascular events and death remain an issue to debate. A meta-analysis of 34 studies (164,494 participants, 21 cross-sectional studies, and 13 cohort studies) failed to find that the presence of NAFLD was associated with risk of CVD and overall mortality. 18 By using electronic healthcare databases from European countries, another matched cohort study of 18 million European adults found that the diagnosis of NAFLD or NASH is more weakly associated with any excess risk of AMI and stroke after adjusting for multiple confounding factors. Nevertheless, heterogeneity across studies or databases was the concerning limitation in these studies. 19
Here, a large-scale prospective cohort study with more than 0.5 million population from the UK Biobank was conducted to investigate the association between NAFLD and risk of CVD and all-cause mortality. Whether the detection of NAFLD could further improve the prediction efficiency for adverse CVD outcomes and all cause mortality more than that of traditional cardiovascular risk factors was also evaluated.
Materials and methods
Data resource and participants
The UK Biobank is the world’s largest biomedical database containing extensive epidemiological resource, family and medical history, physical and cognitive measures life-style questionnaires, and biological samples (including genotyping). Between 2006 and 2010, more than 500,000 volunteers aged 40–69 years were recruited in this cohort across the United Kingdom.20,21 Potential participants were identified from the National Health Service patient registers and invited to attend a local assessment center. Starting from recruitment, participants have been followed for health-related outcomes and mortality via electronic linkage with hospital inpatient, death register, and self-reported health problems. The UK Biobank has ethical approval from the North West Multi-center Research Ethics Committee.
The preliminary data extraction included 502,492 participants. The exclusion criteria were as follows: (1) Alcohol consumption above threshold (more than once or twice a week), participants who took any alcohol were excluded in sensitivity analysis; (2) event (AMI and stroke) occurrence at baseline; (3) participants lost during the cohort; (4) participants with event or death occurrence less than 5 years after admission time to reduce potential reverse causation; (5) diagnosis of alcohol liver disease, toxic liver disease, and chronic viral hepatitis; and (6) fatty liver index (FLI) could not be calculated and missing data. The ICD-10 code system was applied to define the diagnosis of alcohol liver disease (K70), toxic liver disease (K71), and chronic viral hepatitis (B18). Finally, the number of eligible participants in this study was 226,432 for all-cause outcome and 215,245 for major adverse cardiovascular event (MACEs) outcome (Figure 1).

Flowchart describing initial dataset and exclusions leading to final cohorts.
Exposure and variable definition
NAFLD is defined using FLI, which is calculated from the algorithm developed by Bedogni et al. 22 The algorithm of FLI was composed of BMI, waist circumference, triglycerides, and γ-glutamyl transferase. The algorithm is expressed as follows

FLI was categorized in accordance with Bedogni et al. as follows: low FLI (<30) ruled out fatty liver, intermediate FLI (30–59) ruled in intermediate status, and high FLI (⩾60) ruled in fatty liver. Liver fibrosis was measured by FIB-4 score, a non-invasive score calculated by age, ALT, AST and platelet count. For the subgroup analysis, we used 1.45 as the cut-off of value to rule in liver fibrosis. 23
Other variables included age, sex, ethnic, Townsend deprivation index (TDI), BMI, waist circumference, smoking status, fasting plasma glucose, HbA1c, HDL (high density lipoprotein), LDL (low-density lipoprotein), total cholesterol, triglycerides, systolic and diastolic blood pressure, aspartate aminotransferase (AST), alanine aminotransferase (ALT), direct bilirubin, γ-Glutamyl transpeptidase (γ-GT), creatinine, Statins therapy, C-reactive protein (CRP), hypertension, and diabetes.
Outcome definition
The outcome definition was based on the International Classification of Diseases, 10th revision (ICD-10) code. Primary outcome was MACEs, which was defined as the first occurrence of myocardial infarction (I21, I22, I23, I24, I25, and self-report), stroke (I60, I61, I63, I64, and self-report), or CVD death (I05-I89) after admission. Secondary outcomes were defined as all-cause mortality, CVD mortality (I05-I89), AMI mortality (I21), and stroke mortality (I61, I63, I64).
Statistical analysis
This is a large scale population based prospective cohort study. Baseline characteristics were described as the number (percentage) for categorical variables, the mean (standard deviation) for continuous variables. The clinicopathological features of patients with different levels of FLI and p values for trend were evaluated and compared using Chi-square test and ANOVA. Cox proportional hazard models were fitted for all the outcomes, with the survival time being from admission to the first event of occurrence or death. Survival participants and other competing outcomes were defined as censored data. Hazard ratios (HRs) and 95% confidence interval (CI) were reported. Cause-specific (CS) method was used to build competing-risks models to explore cardiovascular mortality. The CS model is suitable for answering etiological questions, and the regression coefficient reflects the relative effect of covariates on the increased incidence of the main endpoint in the target event-free risk set. When there are competing risk events and the formula used for the CS model was
Results
Baseline characteristics
The information of 502,492 participants were extracted from the UK Biobank database. After exclusion, a total of 215,245 participants were included in exploring the association between NAFLD and MACEs. Overall, 134,183 (62.3%) participants were female, with a mean age of 55.86 years. Patients with NAFLD were observed to have a higher proportion of male and smoking; a higher prevalence of hypertension and diabetes; higher proportion of taking statins; and higher levels of TDI, glucose, HbA1c, LDL, AST, ALT, cholesterol, triglycerides, systolic and diastolic pressure, CRP, and creatinine than those with non-NAFLD. The p values for trend of these variables were significant (p < 0.001, Table 1).
Baseline characteristics.

ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; CRP, C-reactive protein; HDL, high density lipoprotein; LDL, low density lipoprotein; NAFLD, nonalcoholic fatty liver disease.
NAFLD and mortality outcomes
In primary outcome analysis, the median time to follow-up was 11.62 years for MACEs. MACEs occurred in 4,080 patients during the follow-up. Among these patients, 1516, 1133, and 1431 events occurred in patients with NAFLD, with intermediate NAFLD, and without NAFLD, respectively. Compared with non-NAFLD, NAFLD is a risk factor for MACEs (HR: 1.25, 95% CI: 1.14–1.36) after adjusting for all covariables. Individuals with intermediate-NAFLD were already in higher risk of MACEs outcome than those without NAFLD (HR 1.16, 95% CI: 1.07–1.26).
The median times to follow-up were 11.62 years for all-cause mortality, 11.61 years for CVD mortality, and 11.59 years for AMI and stroke mortality. NAFLD was a risk factor for all-cause mortality (HR 1.14, 95% CI 1.08–1.20), CVD mortality (HR 1.61, 95% CI 1.42–1.82), and AMI mortality (HR: 1.58, 95% CI: 1.19–2.11) after adjusting for all covariables. Intermediate-NAFLD was also a risk factor for CVD mortality (HR 1.28, 95% CI: 1.14–1.45) and AMI mortality (HR 1.34, 95% CI: 1.01–1.78). However, no significant association was found between NAFLD and stroke mortality (Table 2). Competing risk models showed a similar trend for the association between NAFLD and mortality outcomes (Supplementary Table 1).
Association of NAFLD with cardiovascular disease and all-cause mortality.
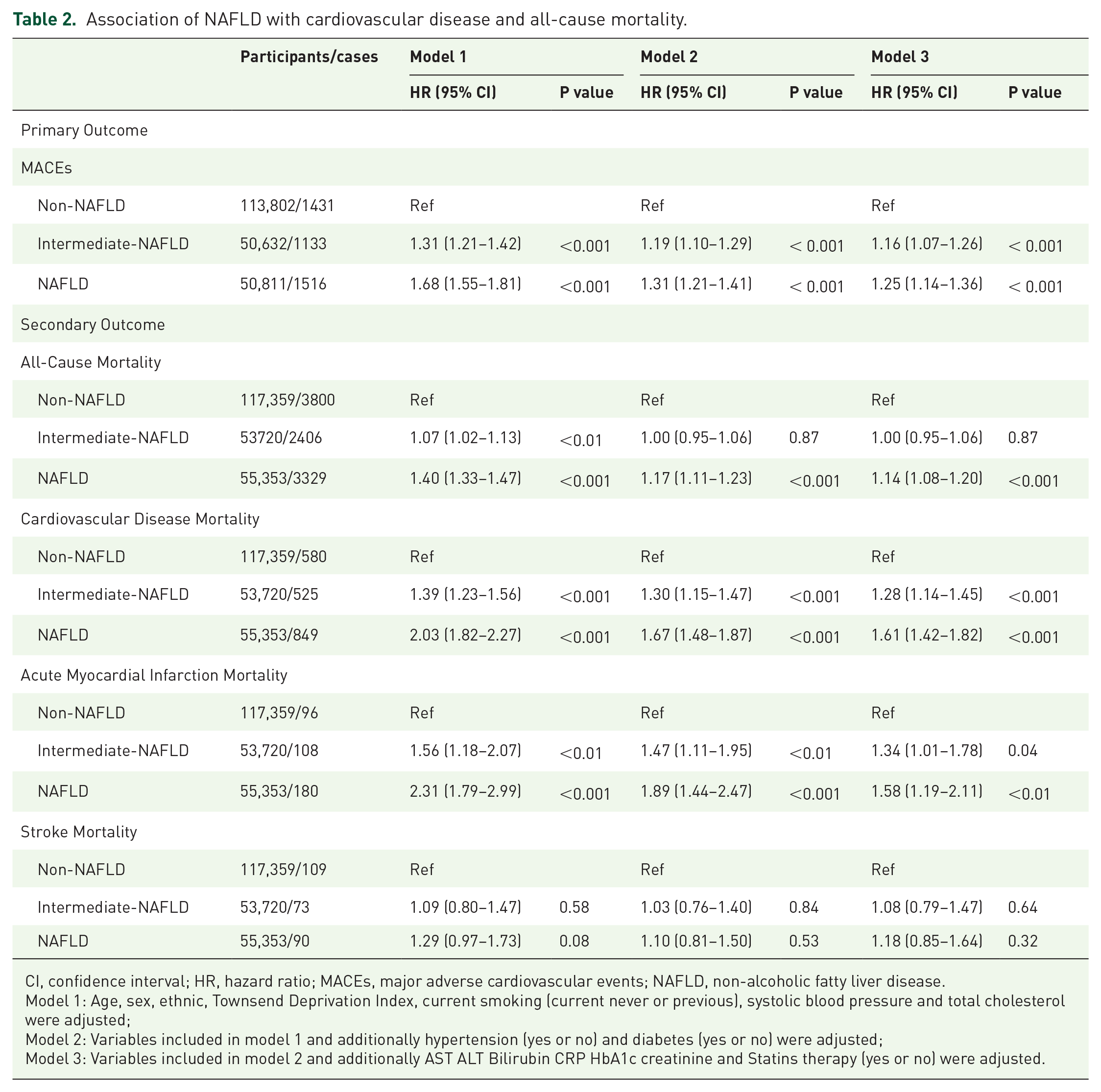
CI, confidence interval; HR, hazard ratio; MACEs, major adverse cardiovascular events; NAFLD, non-alcoholic fatty liver disease.
Model 1: Age, sex, ethnic, Townsend Deprivation Index, current smoking (current never or previous), systolic blood pressure and total cholesterol were adjusted;
Model 2: Variables included in model 1 and additionally hypertension (yes or no) and diabetes (yes or no) were adjusted;
Model 3: Variables included in model 2 and additionally AST ALT Bilirubin CRP HbA1c creatinine and Statins therapy (yes or no) were adjusted.
RCS analysis between FLI and outcomes
The estimated nonlinear association between FLI and outcomes is shown in Figure 2 and Supplementary Figure 1. Evidence of nonlinearity with all-cause mortality (p nonlinear < 0.001), cardiovascular mortality (p nonlinear = 0.02), and nonfatal myocardial infarction (p nonlinear = 0.01) could be found, while other outcome did not show any nonlinear relationship. Except for fatal/nonfatal stroke, a positive association was found in most outcomes (p overall < 0.001).
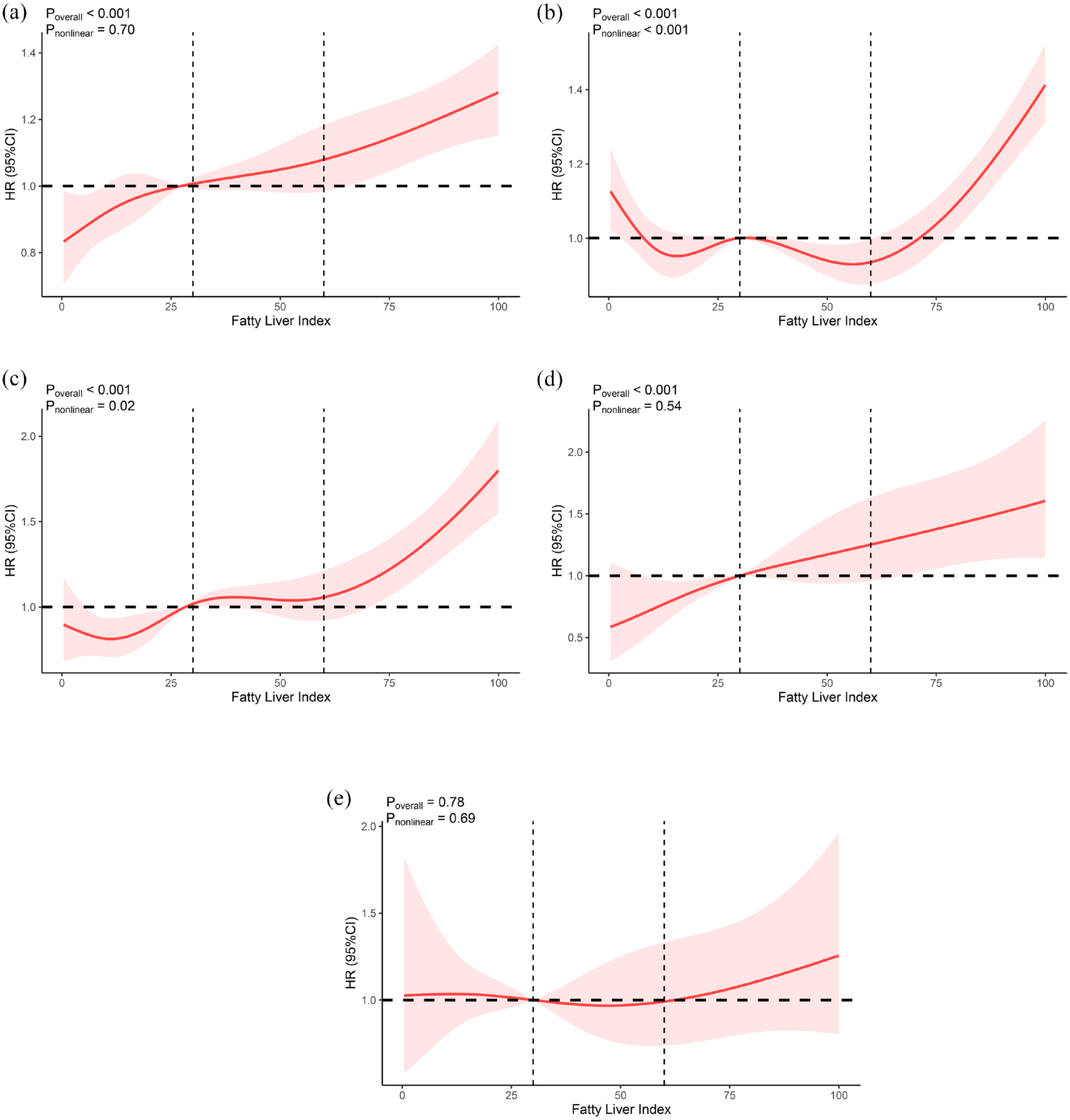
Association of Fatty Liver Index and cardiovascular disease and all-cause mortality. (a) Major Adverse Cardiovascular Events (MACEs), (b) All-Cause Mortality, (c) Cardiovascular Disease Mortality, (d) Acute Myocardial Infarction Mortality, (e) Stroke Mortality.
Subgroup and sensitivity analyses
Stratified analyses were conducted in accordance with the potential risk factors (Figure 3). The associations between NAFLD and the risk of MACEs were stronger among individuals with older age (⩾60 years), no current smoking, BMI < 25 kg/m2, and no hypertension (all p values for interaction < 0.01). Similar results were found in CVD mortality. No current smoking individuals showed higher risk in fatal and nonfatal AMI outcomes, and no hypertensive participants exhibited a higher risk in the latter outcome (Supplementary Figure 2). Sensitivity analysis showed that the risk of nonfatal myocardial infarction and CIHD mortality was higher in participants with NAFLD, similar to the result of MACEs (Supplementary Table 2). Moreover, when participants who had a habit of drinking alcohol were excluded, the HRs for all the outcomes had no substantial change (Supplementary Table 3). Finally, sensitivity analysis with full database (database without excluding participants with event or death occurrence less than 5 years after admission time and drinking alcohol) was also conducted and the similar results were showed (Supplementary Table 4).

Forest plot for risks of all-cause and major adverse cardiovascular events associated with NAFLD stratified by potential risk factors. (a) Major Adverse Cardiovascular Events (MACEs), (b) All-Cause Mortality, (c) Cardiovascular Disease Mortality, (d) Acute Myocardial Infarction Mortality, (e) Stroke Mortality.
Risk prediction efficiency of FLI and NAFLD
When FLI was combined with other CVD risk factors (age, sex, ethnicity, total cholesterol, diabetes, hypertension, and smoking status), a significant improvement was observed in the discriminatory power of the prediction for primary and secondary outcomes (C index: 0.753 versus 0.754, p < 0.001 for all-cause outcome; 0.766 versus 0.768, p < 0.001 for MACEs; 0.803 versus 0.809, p < 0.001 for CVD mortality; 0.804 versus 0.811, p < 0.01 for AMI mortality; and 0.833 versus 0.838, p = 0.03 for CIHD mortality) (Table 3).
C-index for traditional risk model and NAFLD model.
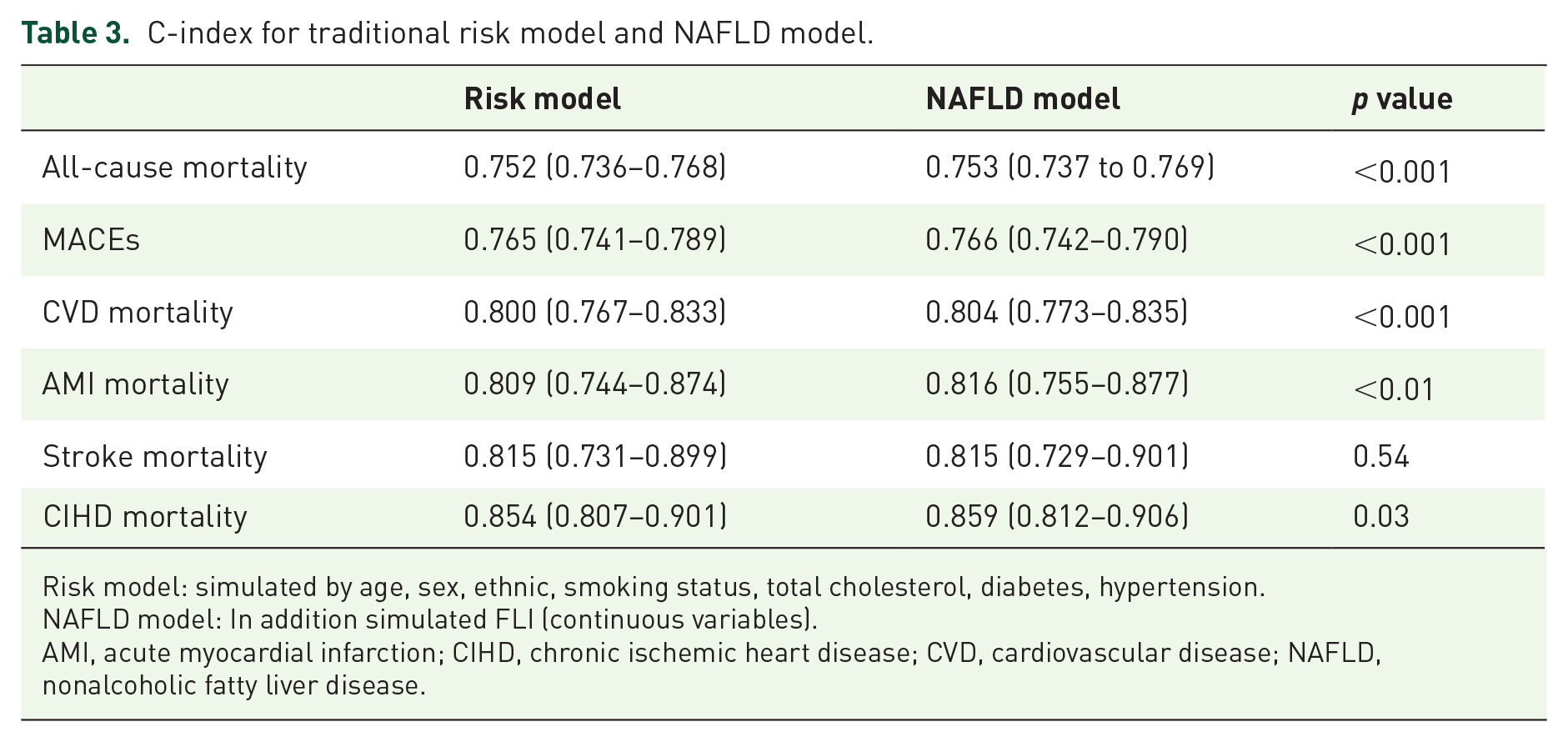
Risk model: simulated by age, sex, ethnic, smoking status, total cholesterol, diabetes, hypertension.
NAFLD model: In addition simulated FLI (continuous variables).
AMI, acute myocardial infarction; CIHD, chronic ischemic heart disease; CVD, cardiovascular disease; NAFLD, nonalcoholic fatty liver disease.
Discussion
In this large prospective cohort study from the United Kingdom, NAFLD was observed to be a risk factor for MACEs, all-cause mortality, CVD mortality, and nonfatal AMI. An increased risk was observed even in patients with intermediate NAFLD, independent with demographic characteristics, traditional cardiometabolic risks, hepatic function, and renal function. Detection of NAFLD could improve the risk prediction efficiency of CVD based on traditional risk factors.
Basically, FLI and the exclusion of alcohol consumption were main criteria to diagnose NAFLD in our study. Several indexes have been developed to predict the presence of fatty liver. Fatty liver index has been proposed and validated in general population. Highly accuracy has been proven in detecting fatty liver (accuracy of 0.84 and specificity > 0.86 for an FLI > 60). 22 FLI has also been validated using magnetic resonance spectroscopy 25 and other study using biopsy 26 reported that FLI could differentiate between moderate and mild steatosis, and showed a linear trend across the steatosis grades. In order to further discuss the relationship between NAFLD-related fibrosis and CVD outcomes, FIB-4 score was used in subgroup analysis. However, the risk of CVD and all cause mortality was not significantly higher in high FIB-4 score subgroup. Other study also reported that surrogate risk scores for NAFLD-related fibrosis, such as FIB-4 do not add information in assessing the CVD events in patients with CAD proven by angiography. 27
CVD is one of the leading causes of death among patients with NAFLD.28,29 However, as NAFLD shares most of the components of metabolic-related factors with CVD, whether NAFLD is a risk factor for CVD on its own or mediated by co-existing cardiometabolic risk factors has been a controversial issue. Previous studies yielded inconsistent results.18,19,30–33 These differences were possibly caused by the great heterogeneity of pooled study 18 and the NAFLD criteria. 30 A recently published matched cohort study based on four large European electronic primary care databases reported that NAFLD was not associated with the risks of AMI or stroke after adjustment for established cardiovascular risk factors. 19 While that study had a very large sample size (data from 18 million), the prevalence of a recorded diagnosis of NAFLD (2.0%) was much lower than expected (approximately 22% as the median proportion in the present study), indicating that a large proportion of patients with NAFLD was undetected and thus included in the control group, which could bias the risk for CVD toward the null. A Mendelian randomization study from Denmark used a genetic variant in the gene encoding the protein patatin-like phospholipase domain containing 3 protein (PNPLA3) and I148M (rs738409) to investigate the causality between NAFLD and coronary heart disease (CHD), and did not find any association. 31 However, that study was limited by the use of only one variant as a genetic instrument for NAFLD. PNPLA3 is also involved in lipid droplet remodeling and very low-density lipoprotein production, which may explain the negative relationship of the variant with CHD. If genetic variants are pleiotropic (e.g. PNPLA3 for lipid metabolism and NAFLD), Mendelian randomization studies may be biased. 32 In another recently published Mendelian randomization study, the entire set of 12 NAFLD susceptibility genes was not associated with CHD. However, after the genes with an effect on lipid metabolism were excluded, the remaining genetic variants showed a positive relationship with CHD. 33
Although still with controversies, some studies aimed to demonstrate the fundamental mechanisms linking NAFLD to CVD. First, dyslipidemia in patients with NAFLD induces hepatic fat accumulation. This accumulation of visceral fat helps activate inflammatory pathways as well as releasing fat-derived toxic metabolites, ultimately leading to the development of CVD, possibly via mechanisms beyond overweight and obesity.34–36 Second, apart from fat accumulation in the liver, adipose tissue accumulating inside and surround myocardial tissue, play a central role in the pathogenetic association between NAFLD and CVD. Third, hepatic/peripheral insulin resistance, which is frequently in parallel with NAFLD, affecting various processes associated with development of CVD, such as atherogenesis, atherosclerotic lesions progression, and vulnerable plaque rupture.37–39 Finally, gene alterations 31 and gut microbiota dysbiosis are increasingly considered as contributory factors for the development of cardiometabolic diseases associated with NAFLD. 40
Besides, insulin resistance (IR) possibly plays a crucial role connecting NAFLD and cardiovascular diseases. IR is the most relevant pathogenetic features for NAFLD and causes an increase in hepatic lipogenesis and a lack of suppression of adipose tissue lipolysis, with an evaluated flow of free fatty acids (FFAs) in liver.41,42 Once accumulated in the liver, FFAs induce insulin signaling pathway alteration, leading to the development of the systematic state of IR. 43 Therefore, bidirectional relationship was showed between IR and NAFLD. 44 The findings from the researches of chronic hepatitis C virus (HCV) infection strengthen the evidence of bidirectional relationship between IR and NAFLD. NAFLD has been reported with high prevalence (ranging from 40% to 86%) in chronic hepatitis C virus (HCV) infection. 45 Other researches also found that the risk of developing type 2 diabetes mellitus is 11 times higher in patients with HCV infection, and that insulin resistance (IR) is the link between HCV infection and diabetes.46,47 Furthermore, HCV clearance by direct-acting antiviral (DAAs) treatments reverses insulin resistance 48 and allows a significant reduction of MACEs in the prediabetic population. 49 Therefore, the improvement of IR degree could help reduce NAFLD progression and considered to be a potential therapeutic target for NAFLD and NAFLD-related CVD outcomes.
Considering the high prevalence of NAFLD and the global epidemic of CVD, this study found important novel findings for guiding clinical practice. Nowadays, the academic guidelines’ recommendations on screening for NAFLD are inconsistent. The 2018 American Association for the Study of Liver Diseases (AASLD) guideline does not recommend routine screening for NAFLD even in high-risk patients, mainly due to limited treatment options. 50 By contrast, the 2016 European Association for the Study of the Liver recommends screening for NAFLD in patients with obesity, metabolic syndrome, and high CVD risk. 51 The CardioMetabolic Heath Alliance advocated for more comprehensive screening in the community to improve the prevention of metabolic syndrome. 52 The data in the present study showed that NAFLD was associated with increased risk of CVD. More importantly, screening NAFLD could provide further incremental value for CVD prediction based on the established cardiovascular risk factors.
Subgroup analysis interestingly showed that NAFLD had a greater impact on all-cause mortality and CVD-related mortality in older participants (⩾60 years), nonsmokers, participants without obesity, and those without hypertension. The exact pathophysiological mechanisms for these differences among subgroups are still not totally explored. A debate on whether patients with NAFLD with or without obesity have worse clinical outcomes exists. A strong effect of NAFLD was found among participants without obesity in some studies53–55 and the present study. The data in the present study also suggested that females were exposed to higher risk of all-cause and stroke mortality than males. Some studies supported this result.56,57 Since the data focused on middle to old participants (40–69 years), the gender difference was possibly related to the levels of estrogens and faster loss of subcutaneous adipose tissue in aging women than in men.56,58
Our study also found that NAFLD gained higher hazard in nonsmokers. This result was not contradicted with other researches which found that cigarette smoking was independently associated with the onset of NAFLD 59 and advanced liver fibrosis among NAFLD patients, 60 since the subgroup analysis in present study compared smoker and nonsmoker separately and then the interaction effect, rather than compared smoker with nonsmoker directly. This is possibly because cigarette smoking and NAFLD both involved with the systemic inflammation and tissue hypoxemia, oxidative stress, and insulin resistance, which are the common mechanism or overlapping conditions to induce cardiovascular diseases. 61 However, more researches are needed to investigate the causal association among cigarette smoking NAFLD and adverse CVD outcomes.
Strengths and limitations
This study has several strengths. First, the UK Biobank dataset is a national prospective population-based cohort, which reflects a real-world setting situation. Second, it included half a million of individuals and more than 10-year follow-up period, which provided adequate sample size to explore the outcomes related to NAFLD. Third, integrated and comprehensive demographic and clinical information enabled the application of sensitivity analyses which could help minimize confounding factors. Finally, participants within 5 years after admission were excluded, and the detection of dose-response relationship between FLI and outcomes helped enhance the level of evidence on the cause-effect relationship.
Several limitations are important to consider. First, the participants with NAFLD were identified using FLI, which is not the gold standard (liver biopsy) in the evaluation of NAFLD status. Second, nearly 92% participants were white, these data may not be representative of more ethnically diverse populations. Third, alcohol consumption above threshold (more than once or twice a week) is not an exact amount for excluding alcoholic fatty liver. However, we conducted sensitivity analysis excluded participants who had a habit of drinking alcohol, the result for all the outcomes had no substantial change.
Conclusion
NAFLD is an independent risk for all-cause mortality and adverse cardiovascular outcomes. Even in participants with intermediate NAFLD, a higher risk for adverse cardiovascular outcomes was revealed. The detection of NAFLD enhanced the prediction power for all-cause mortality and adverse CVD outcomes. Therefore, screening and management of NAFLD is conducive to the prevention and precaution of CVD.
Supplemental Material
sj-docx-1-taj-10.1177_20406223221122478 – Supplemental material for Association of NAFLD with cardiovascular disease and all-cause mortality: a large-scale prospective cohort study based on UK Biobank
Supplemental material, sj-docx-1-taj-10.1177_20406223221122478 for Association of NAFLD with cardiovascular disease and all-cause mortality: a large-scale prospective cohort study based on UK Biobank by Wen Ma, Wentao Wu, Weixing Wen, Fengshuo Xu, Didi Han, Jun Lyu and Yuli Huang in Therapeutic Advances in Chronic Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.