
Abstract
Objective
A body shape index is a novel indicator for assessing central obesity, but its relationship with cardiovascular disease and mortality remains unclear. This study aimed to assess whether a body shape index-cm, a refined version of a body shape index, improves cardiovascular risk stratification.
Methods
Using data from the National Health and Nutrition Examination Survey from 1999 to 2018, along with follow-up mortality data until 2019, we conducted an observational study to evaluate the performance of a body shape index-cm in identifying cardiovascular disease and predicting mortality. We compared a body shape index-cm with traditional anthropometric indices by employing receiver operating characteristic curve analysis, Cox proportional hazards regression, restricted cubic spline, and Kaplan–Meier survival analysis.
Results
Among 47,668 participants, a body shape index-cm emerged as a superior screening tool for cardiovascular diseases, achieving an area under the curve of 0.701, surpassing those of waist-to-height ratio (0.631), waist circumference (0.624), and body mass index (0.556). A body shape index-cm showed the highest accuracy in identifying coronary heart disease (area under the curve: 0.728). A linear relationship was observed between a body shape index-cm and cardiovascular mortality risk, with each standard deviation increase in a body shape index-cm associated with a 20% increase in mortality risk.
Conclusions
A body shape index-cm outperforms traditional measures in identifying cardiovascular disease and shows a linear correlation with cardiovascular mortality.
Keywords
Introduction
Cardiovascular disease (CVD) is a significant public health challenge worldwide as the leading cause of mortality.1,2 Changes in lifestyle have led to an increasing trend in both the prevalence and mortality rates of CVD. From 1990 to 2019, the global number of individuals affected by CVD nearly doubled, and the number of deaths from CVD significantly increased, highlighting the continuous growth in the burden of CVD and stimulating extensive research into early intervention and prevention strategies. 2 In this context, anthropometric indices have become crucial tools for assessing individual health status and predicting disease risk, playing a vital role in understanding the risks of developing CVD and mortality.
Body mass index (BMI), a widely used indicator to evaluate an individual’s weight relative to their height, has long been employed to assess obesity and related health risks. However, an increasing body of research indicates that BMI does not accurately reflect the distribution of body fat or its metabolic health risks, particularly those concerning central obesity—in which fat accumulates primarily in the abdominal area—which is closely associated with the risk of CVD and metabolic disorders such as diabetes. 3 Waist circumference, a simple yet effective indicator of central obesity, has been extensively validated as strongly correlated with CVD, diabetes, and overall mortality. 4 Moreover, the waist-to-height ratio (WHtR), by incorporating height, further optimizes the assessment of central obesity and related health risks and has proven to be a more effective predictor of CVD risk than BMI. 4 A body shape index (ABSI), an innovative indicator combining information from BMI, waist circumference, and height, aims to more precisely assess central obesity and its impact on health. The uniqueness of ABSI lies in its ability to adjust for the effects of height and weight, thereby more accurately reflecting the distribution and quantity of abdominal fat. Research has shown that ABSI reflects the excess risk associated with increased waist circumference and correlates with premature mortality in the general population. 5 Despite its potential as a comprehensive indicator, the practical utility of ABSI may be constrained by its relatively small numerical values and the complexity of its calculation. These factors could impede its widespread acceptance and understanding among healthcare professionals and the general population, potentially limiting its adoption in clinical and public health settings.
Utilizing the National Health and Nutrition Examination Survey (NHANES) database, we conducted a comprehensive evaluation of BMI, waist circumference, WHtR, and ABSI. We initially optimized the anthropometric index, then employed cross-sectional studies to pinpoint the most effective tools for cardiovascular screening. The identified indicator was further analyzed for its correlation with cardiovascular mortality. This study aimed to provide a scientific basis for developing more accurate and practical models for assessing and predicting cardiovascular disease risk, offering significant support and guidance for the formulation of public health policies and optimization of individual health management strategies.
Material and methods
Study design and participants
NHANES is a series of surveys conducted by the National Center for Health Statistics (NCHS) to evaluate the health and nutritional status of the civilian, noninstitutionalized US population. NHANES employs a complex, multistage probability sampling design to collect health-related data through interviews and physical examinations. 6 We conducted both cross-sectional and retrospective cohort analyses using NHANES datasets from 1999 to 2018, with mortality follow-up data available until 31 December 2019. Our study population included adults aged ≥20 years. Exclusion criteria comprised pregnancy, incomplete follow-up data, missing anthropometric indices, and unreported health conditions. These criteria resulted in a final analytic cohort of 47,668 participants (Figure 1). The study was conducted in accordance with the Declaration of Helsinki (2024), and the protocol was approved by the NCHS Research Ethics Review Board (NCHS IRB/ERB Protocol Number: Protocol #2005-06, Protocol #2011-17, and Protocol #2018-01). Written informed consent was obtained from all participants. All potentially identifiable information was removed to ensure the confidentiality of participants and their households. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 6

Flow chart of study participants. The final sample of 47,668 participants was selected according to inclusion and exclusion criteria.
Anthropometric indices
Anthropometric indices, including height, weight, and waist circumference, were measured by trained health professionals in accordance with the standardized NHANES protocol.
7
BMI was calculated by dividing an individual’s weight in kilograms by the square of their height in meters.
8
WHtR was calculated by dividing an individual’s waist circumference in centimeters by their height in centimeters.
9
ABSI was calculated using the original formula
5
:

Subsequently, for enhanced interpretability, we applied a simplified version as follows:

To further enhance the analytical utility of tools used for assessing obesity-related health risks, this study introduces an adaptation of the traditional ABSI, designated as ABSI-cm. This modification arises from the recognition that the numerical outputs produced by the standard ABSI formula are characteristically small, which may complicate their direct interpretation and application in clinical and research contexts. The formula for ABSI-cm is defined as follows:

The development of ABSI-cm was motivated by the need to scale the index’s values to a magnitude that is more readily interpretable without compromising its ability to maintain fundamental evaluative relationships and comparisons. This was achieved by converting the ABSI formula parameters to centimeters, thus facilitating an isometric scaling of the index. Such uniform scaling ensures that ABSI-cm preserves the capacity of the original ABSI to provide accurate assessments of health risks associated with body shape and central obesity.
Outcomes
In the cross-sectional analysis, the primary outcome was the prevalence of self-reported cardiovascular events among participants. These events encompassed the onset of congestive heart failure, coronary artery disease, angina, heart attack, and stroke, as directly reported by the participants, leveraging the comprehensive data available in the NHANES datasets. This component focused on identifying the presence of CVD, which is pivotal for assessing the utility of anthropometric indices in CVD screening.
The retrospective cohort analysis was designed to explore the risk of cardiovascular mortality over an extended period. Utilizing follow-up mortality data, this analysis concentrated on cardiovascular mortality as its core outcome, with deaths attributed to cardiovascular causes coded according to the International Classification of Diseases Tenth Revision (ICD-10) codes I00–I09, I11, I13, and I20–I51. 10
Covariates
Covariate data, including demographic information such as age, sex, race/ethnicity, and educational attainment, were collected through standardized questionnaires. Blood pressure measurements were performed by trained health personnel following a standardized protocol. Hypertension was defined by self-reported history, use of blood pressure control medication, or measurements with systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg. 11 Diabetes status was assessed based on self-reported history, diabetes medication use, fasting blood glucose levels ≥7.0 mmol/L (126 mg/dL), or HbA1c ≥6.5%. 12
Statistical analysis
In the description and analysis of baseline characteristics, continuous variables are reported as means ± standard deviations (SD) and were analyzed using t-tests or Mann–Whitney U tests based on the data distribution. Categorical variables were summarized as frequencies and percentages and examined using chi-square tests.
Building on these foundational comparisons, the effectiveness of various anthropometric indices, including BMI, waist circumference, WHtR, and ABSI-cm, as screening tools for CVD was assessed. The area under the receiver operating characteristic curve (AUC) was computed for each index across different cardiovascular conditions. DeLong’s test was employed to compare the AUC values among these indices for each distinct CVD to ascertain the statistical significance of differences in diagnostic accuracy.
Upon establishing ABSI-cm as the index with the greatest diagnostic efficacy, we subsequently assessed its association with cardiovascular mortality risk. Restricted cubic spline models assessed the potential nonlinearity of this association. With linearity confirmed, ABSI-cm was divided into quartiles for risk analysis using the Cox proportional hazards model in a three-tiered adjustment framework: unadjusted (Model I); adjusted for age, sex, and race (Model II); and fully adjusted for a comprehensive set of covariates (Model III). We calculated the hazard ratios for each quartile of ABSI-cm as well as the risk of cardiovascular mortality associated with each SD increase in ABSI-cm and reported the corresponding 95% confidence intervals (CIs) and P-values.
Complementing the Cox analysis, Kaplan–Meier survival curves for each ABSI-cm quartile were constructed to visualize survival probabilities over time, with log-rank tests used to identify significant differences across quartiles. All statistical analyses were performed using R software (version 4.0.3), with statistical significance defined as a P-value of less than 0.05.
Results
Demographic and clinical characteristics
This study included 47,668 participants with a mean age of 49.77 years and a median follow-up duration of 110 months. During the follow-up period, 1829 participants died from CVD. Table 1 presents the baseline differences between participants with CVD (5125) and those without (42,543). Individuals with CVD were significantly older, with an average age of 66.34 years, compared to 47.78 years in the non-CVD group (P < 0.001). Additionally, a higher proportion of males was observed in the CVD group (57.2%) than in the non-CVD group (48.8%), alongside disparities in racial demographics, levels of education, and smoking habits. Anthropometric analysis revealed that the CVD group had greater values in obesity and central adiposity markers, including BMI, waist circumference, WHtR, and ABSI (CVD: 0.0847 ± 0.005 vs. non-CVD: 0.0812 ± 0.005, P < 0.001) and its intuitive form ABSI-cm (CVD: 393.09 ± 22.07 vs. non-CVD: 376.92 ± 22.83, P < 0.001). The CVD group also had a significantly greater prevalence of hypertension and diabetes, underscoring the heavy burden of comorbidities. Mortality statistics revealed a pronounced disparity in cardiovascular-specific mortality, with the CVD group exhibiting a much higher rate (14.7% vs. 2.5%, P < 0.001). Moreover, measures indicative of central obesity—waist circumference, WHtR, ABSI, and ABSI-cm—were significantly elevated in the cardiovascular mortality group, suggesting these as potential markers for increased cardiovascular mortality risk. Conversely, BMI was not significantly different between groups (Supplementary Appendix Table S1). These findings illustrate a strong correlation between CVD and various demographic, lifestyle, and body composition factors, emphasizing the necessity for comprehensive risk evaluation in the fight against CVD.
Comparison of baseline characteristics between individuals with and without cardiovascular diseases.

Continuous variables are presented as mean ± SD; categorical variables are presented as count (percentage).
CVD: cardiovascular disease.
Comparative analysis of anthropometric indices for CVD screening
Building upon our comprehensive analysis, we delved deeper into the comparative effectiveness of BMI, waist circumference, WHtR, and ABSI-cm by conducting a nuanced evaluation of their screening capabilities for various cardiovascular conditions, as illustrated in Figure 2 and Table S2. ABSI-cm emerged as the most effective screening tool for CVD, demonstrating an AUC of 0.701, significantly surpassing WHtR (AUC: 0.631), waist circumference (AUC: 0.624), and BMI (AUC: 0.556), with P-values for differences in AUC all less than 0.001. In the context of coronary heart disease, ABSI-cm achieved an AUC of 0.728, demonstrating superior diagnostic performance compared to BMI (AUC: 0.544), waist circumference (AUC: 0.629), and WHtR (AUC: 0.619), with all comparisons yielding P-values less than 0.001. Similarly, for heart attack risk assessment, the AUC of ABSI-cm (AUC: 0.720) was significantly higher than those of BMI (AUC: 0.546), waist circumference (AUC: 0.627), and WHtR (AUC: 0.622), with P-values indicating statistical significance (P < 0.001) against each metric. This pattern of superiority extended to the diagnosis of heart failure, angina, and stroke, with ABSI-cm consistently achieving the highest AUC values for these conditions (P < 0.001), further confirming its diagnostic advantage over the compared indices.
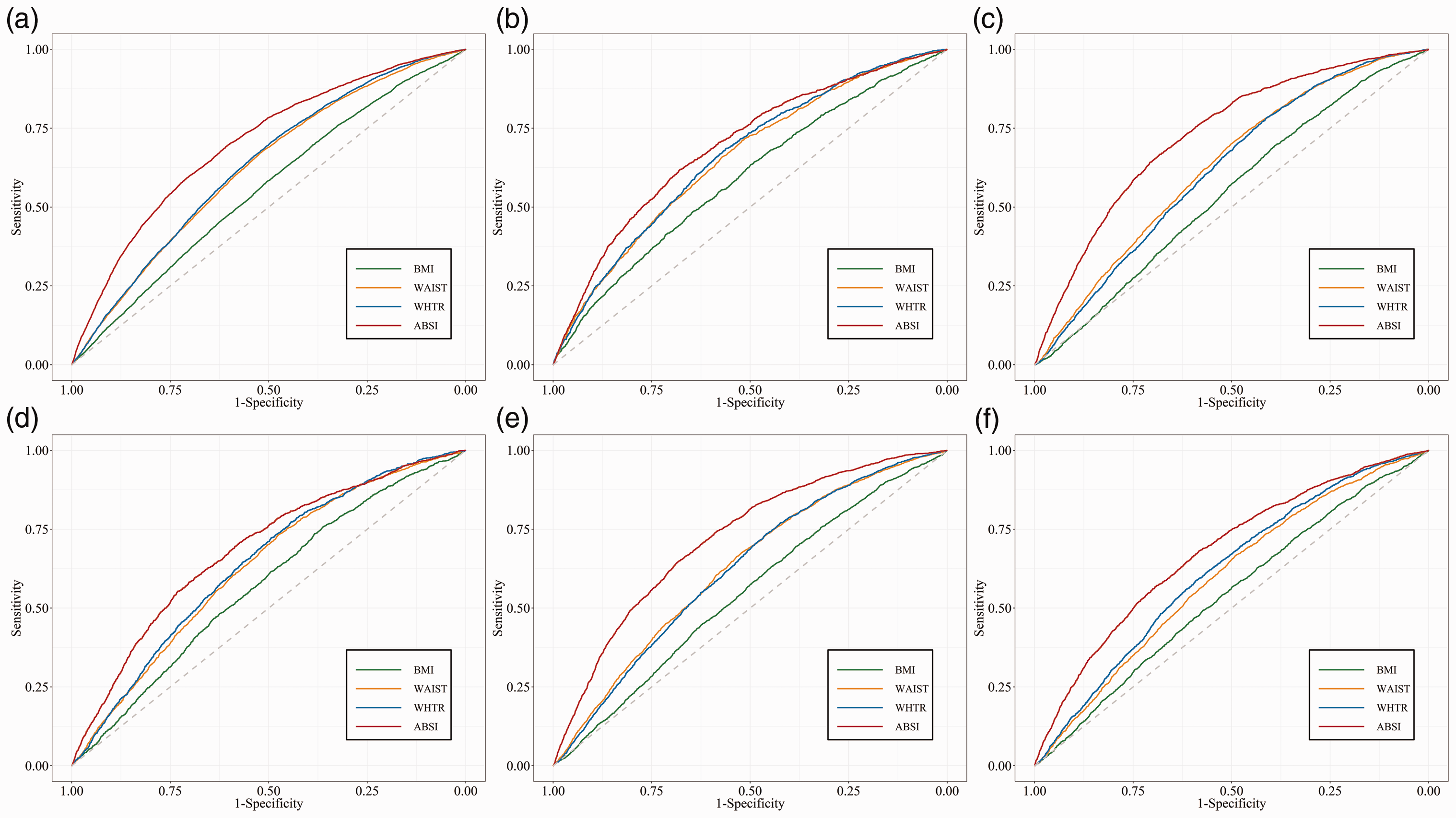
ROC curves for anthropometric indices during screening for cardiovascular-related diseases.
Association of ABSI-cm with cardiovascular mortality risk
To further understand the impact of ABSI-cm on cardiovascular mortality risk, we first employed a nonlinear regression model for evaluation. As shown in Figure 3(a), after adjusting for covariates including age, sex, race, systolic blood pressure, diastolic blood pressure, educational level, smoking status, BMI, diabetes, and hypertension (Model III), no significant nonlinear trend was observed between ABSI-cm and cardiovascular mortality risk (P = 0.475).

Association of ABSI-cm with cardiovascular mortality risk and survival probability. (a) Restricted cubic spline analysis showing the association between ABSI-cm and cardiovascular mortality risk. The model was adjusted for age, sex, race, systolic and diastolic blood pressure, education level, smoking status, BMI, diabetes, and hypertension. The histogram indicates the distribution of ABSI-cm in the study population and (b) Kaplan–Meier survival curves stratified by ABSI-cm quartiles (Q1–Q4), illustrating differences in survival probabilities during follow-up. ABSI-cm: refined version of a body shape index; BMI: body mass index; CI: confidence interval; HR: hazard ratio.
After stratifying ABSI-cm into quartiles, Cox proportional hazards model analyses (see Table 2) revealed a significantly increased risk of cardiovascular mortality for the highest quartile (Q4) compared to the lowest quartile (Q1). In the unadjusted Model I, the hazard ratio (HR) for Q4 was 9.67 (95% CI: 8.12–11.51, P < 0.001). In Model II, which adjusted for age, sex, and race, the HR was slightly reduced but still significant (HR = 1.67, 95% CI: 1.38–2.02, P < 0.001). In Model III, fully adjusted for all covariates, the HR for Q4 compared to Q1 increased by 49% (HR = 1.49, 95% CI: 1.22–1.81, P < 0.001), and for each standard deviation increase in ABSI-cm, the risk of cardiovascular mortality increased by 20% (HR = 1.20, 95% CI: 1.13–1.27, P < 0.001).
Multivariate Cox regression analysis of the association between ABSI-cm and cardiovascular mortality.
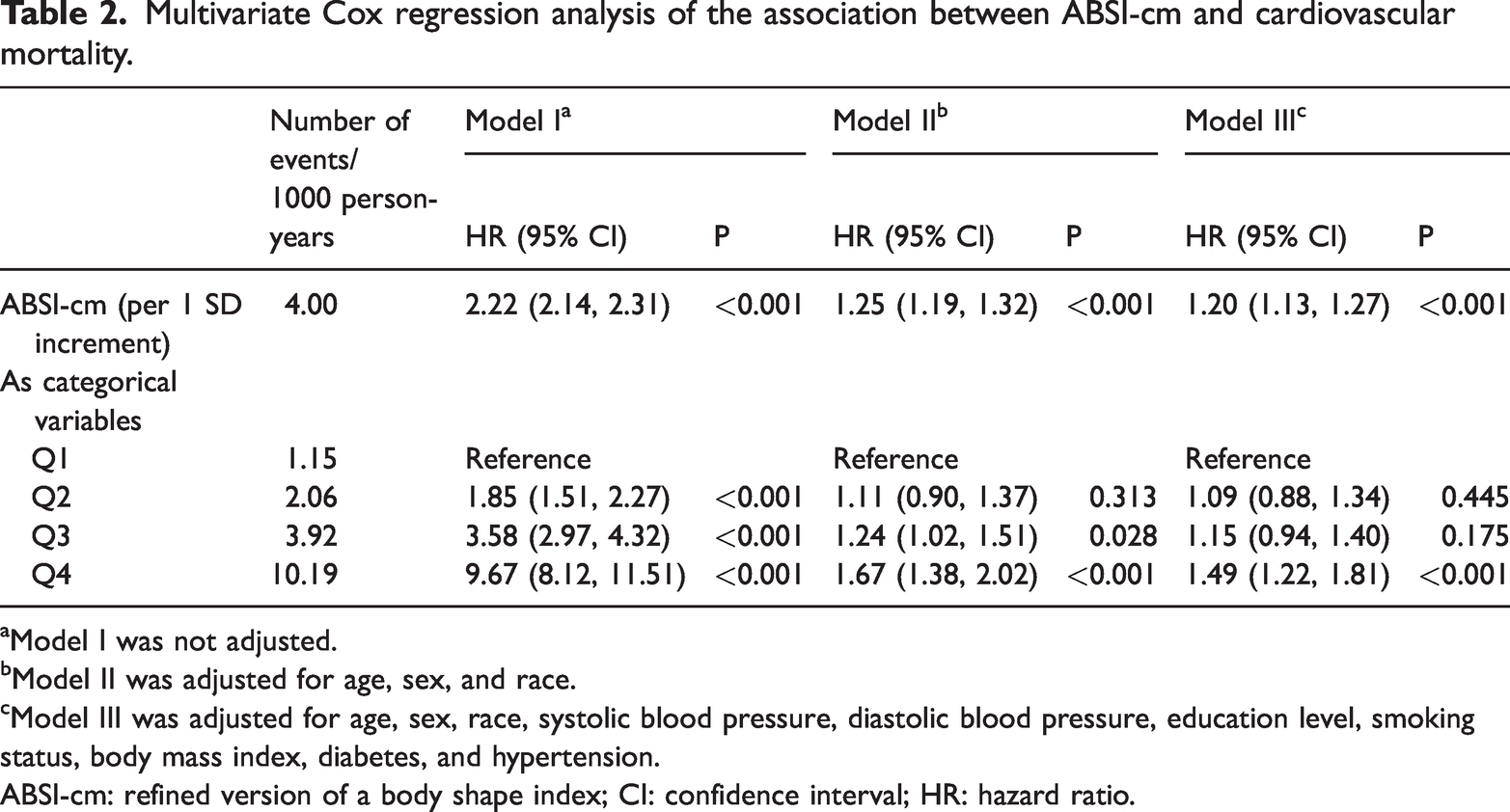
Model I was not adjusted.
Model II was adjusted for age, sex, and race.
Model III was adjusted for age, sex, race, systolic blood pressure, diastolic blood pressure, education level, smoking status, body mass index, diabetes, and hypertension.
ABSI-cm: refined version of a body shape index; CI: confidence interval; HR: hazard ratio.
As depicted in Figure 3(b), the Kaplan–Meier survival curves clearly show the differences in survival probability between the different ABSI-cm quartiles. With increasing ABSI-cm quartiles, the survival probability of cardiovascular mortality significantly decreased, a trend that reached statistical significance in the log-rank test (P < 0.001), further validating the efficacy of ABSI-cm as a predictor of cardiovascular mortality.
Discussion
Through optimizing ABSI to develop ABSI-cm, this study substantially enhances its applicability. It reveals that ABSI-cm, compared to conventional anthropometric indices such as BMI, waist circumference, and WHtR, demonstrates superior utility in identifying CVD risk and predicting cardiovascular mortality. The results illustrate that ABSI-cm, by integrating body shape with central obesity measures, offers a more accurate reflection of cardiovascular health risks. The significance of these findings is heightened by the escalating global burden of CVD,2,13,14 underscoring the necessity for more refined and effective tools for early detection and risk stratification.
The traditional use of BMI and waist circumference for anthropometric assessments in clinical settings is increasingly questioned due to their inadequacy in accurately reflecting the metabolic and cardiovascular risks of obesity. Specifically, the inability of BMI to differentiate between fat and muscle mass and its inability to account for fat distribution severely limits its predictive power for cardiovascular risk. This is particularly problematic considering the strong link between central adiposity and increased risk of CVD, suggesting that BMI alone might not offer a true reflection of an individual’s cardiovascular health.15,16 Similarly, although waist circumference is a better marker of central adiposity than BMI, its failure to account for variations in body size, particularly height, could result in misclassification of cardiovascular risk among diverse populations. This issue is compounded by the absence of standardized measurement techniques, which introduces further variability and potential inaccuracies in cardiovascular risk assessment, thereby undermining the reliability of waist circumference as a sole metric.15,17
WHtR emerges as a superior metric over BMI and waist circumference for evaluating cardiovascular risks, due to its ability to provide a more accurate assessment of central adiposity across varied populations. However, WHtR is not devoid of limitations. Its simplicity, while beneficial for widespread use, may overlook the intricate dynamics of fat distribution and the distinct health implications of various fat types. Moreover, the application of a universal WHtR threshold fails to account for individual differences in body composition, namely the nuanced variations across ethnicities, ages, and sexes. Such oversights highlight the need for more sophisticated and individualized health metrics that can capture the multifaceted nature of obesity and its impact on cardiovascular health more accurately.4,18 This critical evaluation of WHtR, BMI, and waist circumference underscores the urgent need for more advanced and nuanced health assessment tools.
To address the limitations of BMI and waist circumference, the development of ABSI and its novel adaptation, ABSI-cm, represents a significant advancement in the field of anthropometric assessments. By incorporating BMI, waist circumference, and height, ABSI-cm offers a more nuanced measure of body fat distribution and its associated health risks. Our findings, utilizing the large-scale NHANES cohort, further demonstrate that ABSI exhibits superior diagnostic performance across various CVD conditions, with higher AUC values in predictive models, highlighting its potential to more accurately identify individuals at increased risk for cardiovascular morbidity and mortality. Importantly, ABSI has been associated with various metabolic diseases, supporting the metric’s broad applicability and reliability.19–21 The innovation of ABSI-cm addresses critical gaps in traditional metrics by adjusting for variations in body size, thus providing a more accurate assessment of visceral fat—a key factor in cardiovascular health. Moreover, the introduction of ABSI-cm as a standardized metric enhances its applicability and interpretability in clinical practice, promoting early intervention and personalized care strategies.
As an observational study, this work has certain limitations. The analysis is primarily based on NHANES data, and the generalizability of our findings may be restricted due to the dataset’s specific demographic characteristics. Additionally, although adjustments were made for known confounders, the possibility of residual confounding cannot be ruled out. The use of ABSI-cm, although innovative, requires further validation in comparison with traditional measures across diverse groups. Despite these considerations, this study adds to the literature on advanced anthropometric measures in cardiovascular health, emphasizing the potential of ABSI-cm for enhanced risk stratification and calling for continued development in CVD risk management approaches.
Conclusion
Compared with traditional indices such as BMI and waist circumference, ABSI-cm exhibits an enhanced capability for screening CVD and improved predictive accuracy for CVD mortality. This finding underscores the critical role of sophisticated anthropometric indices in refining cardiovascular health assessments and informing public health policy development. Consequently, this study contributes significantly to improving CVD risk stratification and management, advocating for the inclusion of advanced tools such as ABSI-cm into clinical and public health protocols.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605251343018 - Supplemental material for An optimized anthropometric index—a body shape index-cm—demonstrates superior performance in cardiovascular risk stratification
Supplemental material, sj-pdf-1-imr-10.1177_03000605251343018 for An optimized anthropometric index—a body shape index-cm—demonstrates superior performance in cardiovascular risk stratification by Jiayu Tian, Xuejie Wang, Xiaoqin Wen and Bo Gao in Journal of International Medical Research
Footnotes
Acknowledgments
We thank the participants and staff of the NHANES for making this study possible.
Author contributions
Conceptualization, Bo Gao; methodology, Xuejie Wang; software, Jiayu Tian; validation, Xuejie Wang; formal analysis, Jiayu Tian; data curation, Xiaoqin Wen; writing—original draft, Jiayu Tian; writing—review and editing, Xuejie Wang, Xiaoqin Wen, and Bo Gao; visualization, Jiayu Tian and Xiaoqin Wen; supervision, Bo Gao; project administration, Bo Gao. All authors have read and agreed to the published version of the manuscript.
Data availability statement
Declaration of conflicting interests
The authors report no conflicts of interest related to this work.
Funding
None.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.