
Abstract
Palliative care is essential for patients with chronic pulmonary diseases, especially in low- and middle-income countries (LMICs). Chronic respiratory diseases (CRDs), such as chronic obstructive pulmonary disease and interstitial lung diseases, cause significant morbidity and mortality globally, with a heavy burden in LMICs. Despite the need, access to palliative care in LMICs is limited, leading to inadequate symptom management and support. Palliative care benefits include improved quality of life, reduced healthcare costs, and increased patient and family satisfaction. However, barriers in LMICs, including limited resources, infrastructure, and trained providers, as well as cultural and regulatory challenges, hinder care delivery. Early integration of palliative care for patients with CRDs can enhance outcomes and reduce healthcare utilization, yet it remains underutilized in these regions. This review highlights the challenges and impact of palliative care for CRDs in these regions. Addressing these issues requires regulatory reforms, provider education, and investments in healthcare infrastructure. Solutions include national policies, training healthcare professionals, telemedicine, and research collaborations. Understanding and addressing barriers to palliative care in LMICs is crucial for improving care quality and outcomes for patients with CRDs.
Keywords
Introduction
Palliative care is a cornerstone in the management of patients with advanced or terminal diseases, particularly chronic pulmonary diseases. This approach addresses the comprehensive needs of patients, including managing dyspnea, depression, cough, asthenia, sarcopenia, weight loss, anxiety, depression, pain, and physical disability, especially in the terminal stages.1,2 As diseases progress and patients approach the end of life, the demand for palliative care intensifies. Additionally, palliative care for chronic respiratory diseases (CRDs) includes vital components such as social and family support, discussions about care goals, and advanced care planning.3,4
While developed countries often have robust palliative care services, low- and middle-income countries (LMICs) face significant financial and logistical limitations, leaving this vulnerable population undertreated.5,6 This review explores the challenges of palliative care in LMICs, its importance, and its impact on patients with chronic and advanced diseases, particularly pulmonary disorders. Understanding the situation of palliative care in these countries highlights the need for strategies to develop palliative care pathways and underscores the necessity for governmental support.
In this narrative review, we explored the scope and practice of palliative care in LMICs and conducted a comprehensive literature review using PubMed as the primary database. We reviewed specifically the literature that addressed aspects of palliative care delivery, challenges, policy, or outcomes in LMICs. We synthesized the findings qualitatively, highlighting recurring themes, barriers, and innovative approaches relevant to LMIC contexts.
Epidemiology of CRDs
CRDs encompass various conditions affecting the airways and lungs, including chronic obstructive pulmonary disease (COPD), asthma, interstitial lung diseases (ILDs), pneumoconiosis, pulmonary hypertension, and pulmonary sarcoidosis.7,8 CRDs were the third leading cause of mortality globally in 2019, 9 responsible for 8.3 million of years of life lost and 26.2 million of years lived with disabilities in 2021. 10 One in four patients in acute respiratory wards has palliative care needs. 11 COPD is the most prevalent CRD, with a global prevalence of 10.3% among people aged 30–79 years in 2019, and 82.5% of these individuals residing in LMICs. 12 COPD accounted for 79.8 million of disability adjusted life years and 73.6% of total CRD disability adjusted life years in 2021. 13 According to the World Health Organization, COPD is the seventh leading cause of poor health worldwide, with nearly 90% of COPD deaths occurring in patients under 70 years old in LMICs. 14 Despite the need, only 14% of people requiring palliative care received it by 2020. 15 The epidemiology of ILDs varies across the countries, the global incidence increased by 51% in the past 10 years. 16 It remains unclear whether this discrepancy is due to an actual difference between countries that might be related to different exposures and genetic backgrounds or due to underdiagnosis because of variable access to medical care and diagnostic studies. The age-standardized mortality rate increased from 2.34 per 100,000 to 2.72 per 100,000 in men between 1990 and 2019, and from 1.34 per 100,000 to 1.76 per 100,000 in women. 17 Moreover, lung cancer remains the most common cancer worldwide, being the most common malignancy in men and the second most common in women. There were almost 2.5 million new cases of lung cancer diagnosed in 2022 and over 1.8 million deaths worldwide.18,19 The highest incidence rate of lung cancer was observed in Northern America, Eastern Asia, and Northern Europe, with the highest national rate being in Hungary. 19 A 2024 study showed that patients with COPD and idiopathic pulmonary fibrosis (IPF) received outpatient palliative care and opioids less than patients with lung cancer, and they were more likely to receive mechanical ventilation and intensive care in the last 6 months of their lives. 20
Importance of palliative care and its economic value
Palliative care aims to improve the quality of life for patients with life-threatening illnesses and their families by addressing physical, psychological, spiritual, and social challenges.15,21 A prospective observational study indicated that integrating palliative care with post-exacerbation functional rehabilitation for patients with CRDs, particularly COPD, ILD, and bronchiectasis, can reduce healthcare utilization, improve functional capacity, and enhance the management of dyspnea, depression, and anxiety. 22
Although more evidence is needed to assess the long-term cost-effectiveness and outcomes of palliative care, existing data support its benefits. 23 Palliative care has been shown to improve patient outcomes, including better pain management, improved quality of life, higher satisfaction with care, reduced healthcare costs, and increased time spent with family at home. 21 Successful implementation will require investment and commitment from various stakeholders, including governments, international health organizations, healthcare professionals, and empowered patient advocates and families.
A 2020 meta-analysis found that palliative care consultation within 3 days of hospital admission reduced hospitalization costs, especially for patients with complex illnesses, and those with four or more comorbidities. 24 Furthermore, early palliative care implementation from emergency department presentation also significantly reduced hospital stays lengths and avoided unnecessary admissions to critical care units, further decreasing healthcare costs.25,26 Several cost-effectiveness studies showed that while palliative care alone was not cost-effective, it resulted in cost savings compared to usual care. This led to a 13% reduction in losses to hospitals’ bottom lines, particularly since around 60% of these patients came from intensive care units, freeing up ICU beds and decreasing overall costs.27,28 Additionally, studies in LMICs have shown that low-cost palliative care is feasible, yielding favorable patient outcomes at a lower cost than traditional care. 23
Palliative care state in LMICs
The disparity in palliative care between high-income countries and LMICs is significant.29,30 Despite the critical need for palliative care, it is more accessible in high-income countries, while LMICs faces numerous challenges, as highlighted in a 2020 systematic review. 31 These challenges include the scarcity of national policies, financial resources, infrastructure, technology, skilled workforce, and adequate education and training for healthcare providers. 32 Cultural factors may also hinder the acceptance and implementation of palliative care strategies. 31 A recent analysis revealed little to no increase in palliative care services in European LMICs over the past 14 years. 33 A 2022 health policy review found no published national palliative care plans in Middle Eastern and North African countries. 34 Disparities exist even within the same country. 35
The picture is grimmer when it comes to pain relief. Pain is considered to be the most common as well as the most feared symptom among patients on palliative care. 36 Comprehensive screening, assessment, and management of pain is the cornerstone of palliative care. 37 Half of the global population residing in the poorest countries receives less than 1% of the distributed opioids measured in morphine equivalent. 38 For example, in India, only 5.8% provide uninterrupted access to oral morphine. 39 In the Eastern Mediterranean Region, specialized palliative care services are scarce and access to pain medication is limited. 40 Additionally, access to opioids in LMICs is limited by high costs, stringent regulations, and inadequate training for healthcare providers. 6 Over-regulation inflates prices and restricts availability, while many facilities lack the infrastructure for safe storage and dispensing. A study by Salikhanov et al. illustrated these issues, showing high out-of-pocket expenditures; a lack of mobile palliative care services for home-based care; severe shortages of opioids to prevent pain suffering; poor formal palliative care education; absence of practical skills training for family caregivers; lack of awareness about palliative care in society; lack of state support; and misunderstanding of palliative care among healthcare providers and late referrals. 41 Referral to palliative care services range from 0% to 38% in ILD patients, with barriers including patients’ fear of discussing the future, prognostic uncertainty, and confusion about the roles of palliative care. 42 Unfortunately, all articles reviewed in this systematic review were from west Europe and north America, reflecting the extreme scarcity of research from LMICs on this topic. Moreover, the transition to palliative care in chronic diseases specifically occurs late and is associated with poor understanding, uncertainty, need for support, and poor communication. 43 Insufficient governmental support and misaligned policies further complicate access.
Barriers also include lack of research on palliative care from LMICs and a lack of basic training in palliative care in some areas. For instance, nursing students at Al Quds University in Palestine showed significantly low knowledge in palliative care despite positive attitude toward end-of-life care. 44
The barriers also extend to the end-of-life care in LMICs, as they rank as the lowest in the quality of death index. A report from the Economist Intelligence Unit, which measures the current environment for end-of life care service with 24 indicators, including basic end-of-life healthcare environment, availability, cost and quality of end-of-life care, and public awareness, highlighted this issue. 45 Palliative care needs are expected to grow with the aging population, even in LMICs. 46 Addressing these issues requires regulatory reforms, improved provider education, and investments in healthcare infrastructure. 5
Chronic obstructive pulmonary disease and palliative care
COPD is a life-limiting illness, that is progressive over time, characterized by accelerated lung function decline and exacerbations leading to distressing symptoms, deconditioning, frequent hospitalizations, and high resource utilizations. It is associated with significant long-term disabilities requiring palliative care and imposes a substantial physical, psychological, social, and economic burden on patients. Data on the economic burden of COPD in LMICs are very scarce, 96% of the manuscripts in a systematic reviewed were from Europe and North America, suggesting that direct and indirect costs are surely underestimated. 47
Breathlessness is a particularly distressing symptom in all advanced COPD patients and is often poorly addressed. 48 Low dose opiates, 49 handheld fans, self-management interventions, breathing exercises, and psychological support are all helpful interventions for refractory breathlessness on top of optimal medical management.50–52 Although noninvasive ventilation is usually initiated as life-sustaining measure, it can be used for palliation after shared decision making. 53 Symptoms extend beyond dyspnea to include limited physical ability, cough, weight loss, sleep disturbances, depression, and anxiety, all contributing to poor health outcomes, reduced quality of life, social isolation, and frequent hospital admissions (Table 1).
Common symptoms in chronic respiratory diseases patients and suggested palliative interventions.

CBT, cognitive behavioral therapy.
Exacerbations mark a rapid decline in health status, with high in-hospital mortality rates reaching 25% during acute exacerbations and a substantial risk of death within 1 year after hospital discharge in 25%–50% of cases, as well as a 25% risk of readmission.54,55 Hence, advanced care planning should start preferably early in the disease and necessarily with evidence of severe advanced disease such as low Forced Expiratory Volume FEV1 <30%, more than two hospitalizations in 1 year, cachexia, and the need for long term oxygen therapy among others. 56 Advanced care planning can help reduce unwanted hospital admissions and futile interventions, allowing optimal use of resources in already resource-constrained areas. It should be tailored to the local culture, spiritual, and religious needs of the patient. However, the uptake of palliative care for COPD is still low even in high-income countries. 57
A study conducted in London revealed that patients with COPD who died had received inadequate primary and secondary palliative care in their last year of life, 58 highlighting significant gaps in the healthcare system’s ability to provide appropriate and timely interventions for COPD patients, particularly as they approach the end of life. The ability of physicians to address all aspects of COPD care, especially at the end of life, has been scrutinized in various studies. One study focusing on patient–physician communication at the end of life, based on patient ratings, found that primary physicians poorly addressed critical areas such as prognosis, death, religion, and spirituality. 59 Moreover, discussions with family and caregivers about the end of life, prognosis, the course of the illness, and death were also found to be unsatisfactory. 60
An 8-year observational study from Turkey showed that 77% of patients with COPD died in the hospital in acute wards. 61 A retrospective study conducted in California showed that the rate of hospital readmission per 6 months decreased from 1.15 to 0.7 per patient after consultation of inpatient palliative care team. 62 Another analysis on inpatient use of palliative care services from Taiwan showed persistently low use of these services in hospitalized patients with COPD. 63 One of the most common reasons behind the lack of palliative care in patients with COPD is that these needs are underrecognized by primary physicians. This was highlighted by a study done by Meffert et al., which showed that palliative care needs were identified by the primary physician upon discharge in only 9.1% of patients admitted for COPD. 64 Additionally, around half of these patients had an underlying malignancy, which was the primary reason for the palliative care referral. The trajectories of the end-of-life care are similar between cancer and COPD; nevertheless, palliative care is offered more frequently to patients with cancer. 65 The ProPal-COPD tool, designed to aid in identifying patients with COPD who may benefit from proactive palliative care, is based on seven key predictors: the “surprise question” (i.e., “Would you be surprised if this patient died in the next year?”), five markers of COPD severity, and the presence of specific comorbidities known to increase post-hospital mortality. 66 The five markers of COPD used in this tool are the Medical Research Council (MRC) dyspnea questionnaire, Clinical COPD Questionnaire, FEV1% of predicted value, body mass index, and previous hospitalizations for acute exacerbation of COPD. These predictors help healthcare providers make informed decisions about the need for early palliative care interventions in patients with advanced COPD.
ILDs and palliative care
ILD encompasses a group of lung disorders, primarily categorized into IPF and non-IPF, characterized by varying degrees of inflammation and fibrosis of the lung parenchyma. These diseases lead to significant morbidity and mortality due to the decline in lung function. Patients with progressive fibrotic ILD face a high disease-associated symptom burden, including breathlessness, cough, fatigue, poor health-related quality of life, depression, and anxiety. 67 They often experience exacerbations that necessitate increased use of emergency care, hospitalizations, and supplementary oxygen support. As the disease progresses, patients require assistance with daily activities and the active engagement of caregivers, highlighting high palliative care needs. 68 Although the disease course can now be modified by antifibrotic medication, access to these medications also might be limited in some areas in LMICs leading to faster disease progression and higher symptom burden. 68
The primary goal of palliative care for patients with ILD is to comprehensively enhance and maintain their quality of life. 69 Palliative interventions address all aspects of patient care, recognizing the unpredictable nature of fibrotic ILDs. The disease course can be unpredictable, and survival rates may be similar to or worse than many oncological conditions. In addition to chronic breathlessness, patients and caregivers are distressed by the unpredictability of disease progression, lack of information, and lack of psychological support. 70 Continuous assessment of patient needs is crucial throughout the disease trajectory. 69 However, there remains a practice bias toward incorporating palliative care measures only at the terminal stage or near the end of life. When consulted, palliative care services are involved late in the course of the disease. 71 A retrospective study showed that most of the patients referred to palliative care are already in the last stages of their nonmalignant lung disease, with 89.4% of them had an MRC class 4–5 dyspnea with a significant underutilization of opioids by nonpalliative care providers. 72 Even in high-income countries, a recent review showed that patients with ILD mostly die in the hospital with high burden of investigations and life prolonging treatment, adding to the strain on resources in all countries, disproportionally affecting LMICs. 73
The Danish Respiratory Society (DRS) published a position paper on palliative care in advanced CRDs, emphasizing specific features in ILD that necessitate palliative care attention. These include recurrent hospitalizations, peripheral oxygen saturation <88%, forced vital capacity (FVC) <50% predicted or a decline in predicted FVC of more than 10%, decline in predicted diffusion capacity of more than 15%, reduced 6-min walk distance less than 212 m, and the presence of pulmonary hypertension or other progressive or severe comorbidities. 74 A Danish survey conducted after the DRS guidelines publication found that despite a generally positive attitude toward palliative care, and widespread knowledge of palliative care guidelines, 60% of physicians reported barriers to palliative care discussions, including a lack of time (63%), absence of multidisciplinary meetings (52%), unpredictable prognosis (63%), and insufficient knowledge about the patient’s culture, spirituality, or religion (20%). 75
A Japanese study evaluated pulmonologists’ practice regarding palliative and end-of-life care, finding greater difficulty in providing palliative care for IPF than for lung cancer due to barriers such as lack of established treatments, difficulty predicting prognosis, discrepancies in care goals among patients, families, and medical staff, and inadequate communication about the goals of care. 76 A study by Koyauchi et al. 77 compared the quality of dying and death in patients with ILD to those with lung cancer from the perspective of bereaved families using the Good Death Inventory (GDI) score. 76 It is found that ILD patients had lower GDI scores, particularly in “physical and psychological distress relief and prognosis awareness and participation in decision making.” Additionally, patients with ILD were less likely to receive specialized palliative care services and opioids and had lower participation rates in end-of-life discussions compared to lung cancer patients. A multidisciplinary meeting between ILD specialists, the palliative care team, and psychology is a promising strategy to optimize care of ILD patients. 78 The positive impact of palliative care, although not consistent in all trials, led to the recommendation of early palliative care integration by international societies.79,80
Lung cancer and palliative care
Lung cancer is the leading cause of cancer-related deaths worldwide, often diagnosed at advanced stages when treatment options are limited. 81 Patients suffer from a wide range of physical and emotional symptoms that impair their quality of life. Despite advancements in treatment, those with advanced disease still experience significant symptom burdens and unmet needs, most commonly dyspnea, fatigue, and cough. 82 Palliative surgical treatments, such as management of airway obstruction, hemoptysis, and pleural exudates, are often used in advanced diseases to improve symptoms and quality of life. 83 Chemotherapy and radiotherapy are also used in palliative care to ameliorate symptoms, including cough, pain, and prolong survival. 83
A substantial body of evidence now supports the use of palliative care for lung cancer patients. Early integration of palliative care with standard oncologic care for advanced disease patients has been proven to improve patients’ quality of life, reduce depression, decrease aggressive end-of-life care, and improve overall survival. 84 The ENABLE III (Educate, Nurture, Advise, Before life ends) trial, which investigated the effect early versus delayed palliative care on quality of life, symptom control, 1-year survival, mood, and resource use, has demonstrated that early initiation of palliative care improves overall survival by a 3-month difference compared to late initiation. 85 Additionally, family caregivers had lower rates of depression and stress burden. 86 A randomized controlled trial found that early palliative care initiation in patients with nonmetastatic lung cancer improved psychological well-being and reduced symptom burden, including pain, nausea, anxiety, and depression. 87 A 2024 study showed that palliative care consultation reduces hospital stay length and total hospital charges, benefiting both healthcare costs and symptom burden. 88
Palliative care access for patients with lung cancer and other malignancies in LMICs remains significantly limited due to various barriers. Key obstacles include inadequate knowledge and skills among healthcare providers, poor coordination of care, and restricted availability of pain medications—particularly opioids, which are often underutilized due to a lack of knowledge or concerns regarding side effects. 89 Additionally, insufficient training for physicians and caregivers hinders effective palliative care provision. 89 Other contributing factors include limited physical infrastructure, the absence of comprehensive national plans for palliative care implementation in lung cancer treatment, and a general lack of education among healthcare providers, caregivers, and patients regarding palliative care’s importance and scope.31,90
Despite the increased use of hospice care, 91 there has been a substantial increase in aggressive care at the end of life, leading to more ICU admissions, invasive procedures, and hospital deaths.83,92 Addressing these issues requires better integration of palliative care services throughout the disease trajectory and improved communication between healthcare providers, patients, and families to align treatment goals with patient preferences and improve overall care quality.
Areas of potential improvement
Providing high-quality palliative care and improving the quality of life and death of patients suffering from CRDs is an achievable goal even in resource-constrained settings.93,94 A recent 2024 study showed that biweekly palliative care conferences following traditional tumor boards facilitated multidisciplinary case discussions, resulting in better pain management and other cancer-related symptoms. 95 To identify unmet patient needs, improve quality of life and outcomes, and address care gaps, implementing patient-reported outcomes (PROs), patient-reported experience measures, and patient-reported outcome measures is recommended. A study has shown that these tools are effective in evaluating the performance of healthcare systems worldwide, specifically in IPF. 96 In lung cancer, the implementation of electronic PROs enhances patient reporting of symptoms, enables timely management, and helps screen patients who would benefit from palliative care services. 97 The needs assessment tool progressive diseases-ILD has been validated to assess palliative care needs in ILD patients. 98
The European Respiratory Society (ERS) task force issued 2023 dedicated guidelines for COPD and ILD patients, making a weak recommendation for integrating palliative care into routine care alongside active disease management. 99 They advise providing accessible, multidisciplinary assessments of physical, psychological, social, and spiritual needs, and embedding specialist palliative care support within an extended team. Continuity of care through trusted healthcare relationships and the careful initiation of advance care planning conversations is essential. The recommendation also included active needs assessment by asking the patients or their informal caregiver, the ERS also suggest that surrogate markers of disease severity and/or health service utilization may help identify those likely to have needs. Multidisciplinary services should also prioritize training, clarify responsibilities, and ensure timely advance care planning, with preferences updated as circumstances change.
Another ERS task force clinical practice guideline addressed symptom management in patients with serious respiratory illness. 100 It weakly recommends using multicomponent services, breathing exercises, and graded exercise therapy to reduce symptoms and fatigue. They also recommended increasing airflow through fans or non-oxygen-enriched compressed air directed at the cheeks, nasal mucosa, and mouth to help decrease breathlessness, though the evidence for this is of very low certainty. 100 They also advised against the use of opioids for the treatment of breathlessness and found the evidence for applying oxygen to relieve breathlessness to be indeterminate and weak.
While tertiary palliative care (specialized palliative care provided by specialists with palliative care training) is desired, it might not be achievable widely, emphasizing the need to support primary and secondary palliative care. Secondary palliative care in this case is provided by respiratory disease specialist physicians, while primary palliative care is basic symptom management provided by all healthcare professionals, physicians, and nurses. In a policy statement, the American Thoracic Society, American Academy of Hospice and Palliative Medicine, Hospice and Palliative Nurses Association, and Social Work Hospice and Palliative Care Network recommended early assessment of symptoms and needs in each encounter with patients with serious respiratory illness and primary palliative care by pulmonary physicians with referral to specialized care according to needs. 101 They also emphasize the importance of primary palliative care training for pulmonary and critical care physicians.
There are no standardized outcome measures to assess palliative care interventions, leading to inconsistent evaluations across studies that typically use generic measures. 102 Implementing standardized outcomes is crucial for consistent and accurate assessment. The ERS task force recommended in their guidelines that clinicians, patients, and caregivers should be involved in the co-design and evaluation of needs assessment tools. 100 They also encouraged the development and evaluation of new tools that focus on the unmet needs of patients throughout their illness, not just at the end of life.
The FRESH-AIR systematic review and meta-analysis evaluated lung health interventions in LMICs, emphasizing understanding local needs, ensuring interventions are compatible with local contexts such as religion, culture, and infrastructure, and engaging individuals in implementing new interventions while providing adequate information, knowledge, and resources. 103 Nurse-led program have been proven to be feasible and effective in some countries, specifically in COPD but unfortunately all the interventions in a systematic review came from high income countries. 104 A new randomized controlled trial evaluated stepped care, where palliative care visits occur only at key points in patients’ cancer trajectories using decrements in quality of life as triggers. This approach has been found to be an effective and more scalable means to deliver palliative care, significantly improving the quality of life for advanced lung cancer patients, resulting in fewer days in hospice.105,106
When it comes to education, multiple initiatives were tried in LMIC setting including online courses, 107 and short interactive workshops. 108 They were shown to be effective in supporting healthcare workers in providing palliative care services. 109 E-learning has been proven beneficial for physicians taking care of dying patients with COVID 19. 110 Different forms of courses were also suggested including basic courses and advanced diploma to mitigate the shortage of specialists, though not specific to CRDs.111,112 The CAPACITY program in Canada also improved self-assessed palliative care identification and primary care provider confidence in core competencies. 113 The program demonstrated potential for building palliative care capacity in primary care teams. Experience from Jamaica in cancer patients shows that building capacity and provider training through adapted curricula and academic partnerships are feasible goals with measurable metrics. 114 Another layer of education is public and community education, one suggested initiative is Last Aid course to educate the public on palliative care and support at end of life. 115 This project is now initiated in 18 countries including countries from South America.
On the other hand, telemedicine is a promising tool for provision of palliative care services combined with rehabilitation online programs, especially in rural areas, though it comes with its own challenges.116,117 In a recent systematic review, digital health interventions to provide palliative care in LMICs were described with promising results including benefit to patient and caregivers with reduced comfort and travel time but also to health care providers. 118
A roadmap should include national policies with clarification and support from legal aspect of palliative care services, focused training of pulmonary physicians, primary care physicians and nursing team, leveraging telemedicine for wider outreach, substudies on palliative care services, easier access to pain relief medications including opiates, and strategies to improve public and community awareness. The paucity of research can be overcome by creating research networks and collaboration, pairing with institutions from high-income countries for joint or comparative research and more grant dedication by international organizations. Table 2 summarizes the challenges facing palliative care in CRDs and the possible areas of improvement.
Challenges facing palliative care for chronic respiratory diseases and possible intervention.
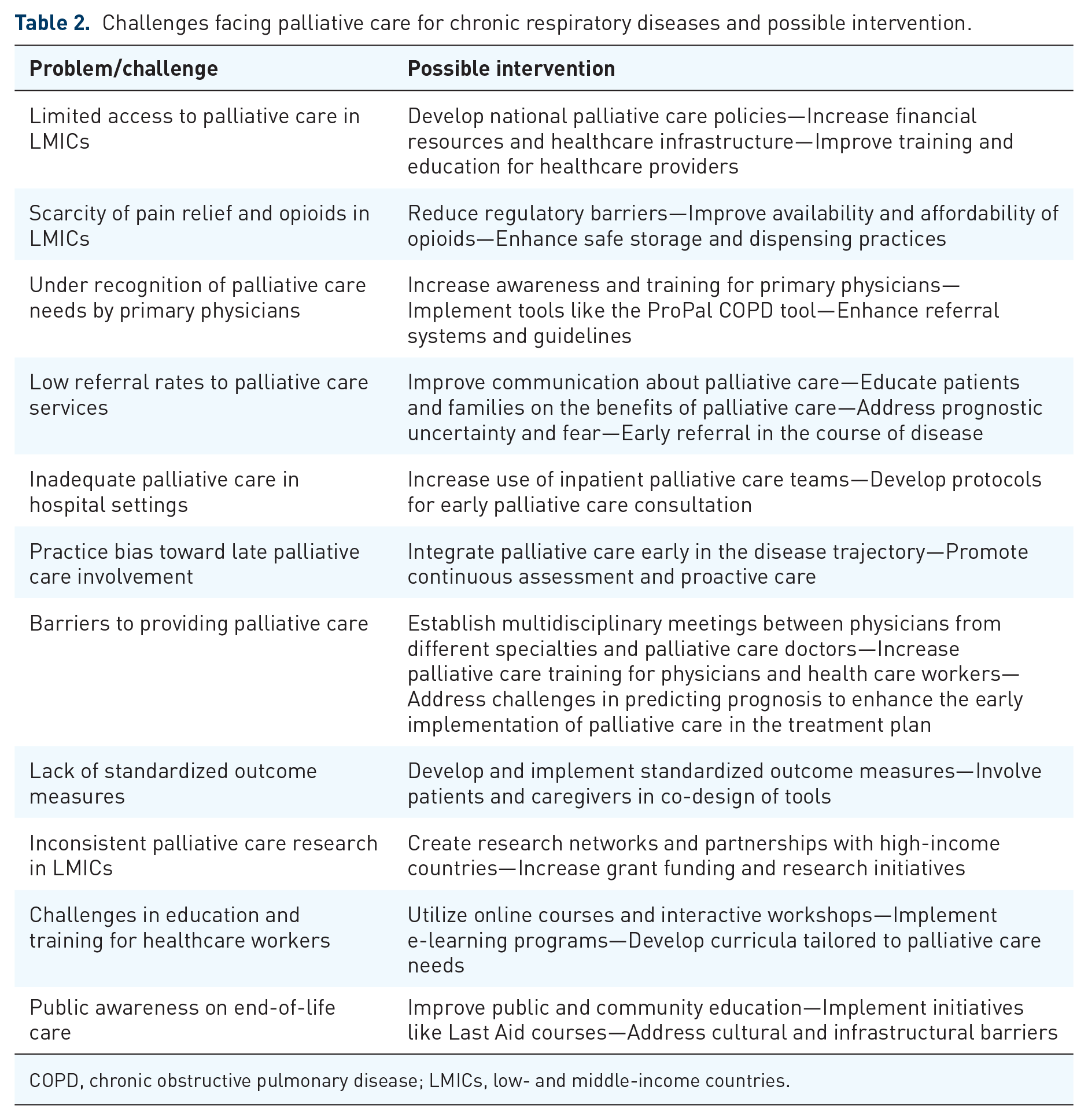
COPD, chronic obstructive pulmonary disease; LMICs, low- and middle-income countries.
Conclusion
Palliative care is an essential pillar in the management of CRDs, and the need for interventions increases with disease progression. However, implementation in LMICs remains in its early stages and faces significant challenges, such as limitations in financial and human resources, a paucity of national policies, and variable buy-in from different stakeholders. Despite these hurdles, various initiatives across different areas have demonstrated success. Potential solutions to enhance palliative care in LMICs include developing national policies, providing primary care palliative care training for healthcare professionals, leveraging telemedicine, and creating research networks.