
Abstract
Chronic obstructive pulmonary disease (COPD) refers to a group of lung diseases that are distinct in underlying aetiology but share a common disease course of persistent and progressive airflow restriction. People living with COPD, as well as the people who care for them, frequently have severe and unmet physical and psychosocial needs, including breathlessness, fatigue, cough, anxiety and depression. Early proactive palliative care is well placed to address these needs, yet it is frequently under-utilised in this group. This narrative review aimed to identify core components of palliative care and examine how existing models of care are implemented to better understand which models can best serve the needs of people with COPD. Symptom palliation, advance care planning, and support for caregivers emerged as the common components underpinning both generalist and specialist models of palliative care. Models of proactive palliative care were diverse in terms of where and how care was delivered as well as which health professionals were involved. Five key models of palliative care were identified: (1) multi-disciplinary integrated services, (2) nurse-led care, (3) hospice and residential aged care, (4) home-based care, and (5) telemonitoring and telehealth. Each model describes a diverse set of interventions and many of these share common elements, including the normalisation of palliative principles within routine care and the provision of diverse delivery settings to accommodate individual preferences and needs. Successful palliative care models must be practical, accessible and innovative to respond to individuals’ complex and evolving needs, foster multi-disciplinary collaboration and input and optimally utilise local healthcare resources.
Introduction
Prevalence, symptom burden, and unmet patient and carer needs in advanced chronic obstructive pulmonary disease
Chronic obstructive pulmonary disease (COPD) refers to a group of lung diseases that are distinct in underlying aetiology but share a common disease course of persistent and progressive airflow restriction. 1 The global prevalence of COPD was estimated at 392 million cases in 2019 with three quarters of these occurring in low- or middle-income countries. 2 These numbers are projected to grow to 600 million by 2050 and to disproportionately impact women and people living in low- or middle-income countries. 3
People living with advanced COPD frequently experience severe and distressing symptom burdens, including breathlessness (also called dyspnoea), fatigue, cough, anxiety and depression, social isolation, and overall reduced quality of life. 1 The burden of COPD can also impact the physical and psychological health of people who provide formal or informal care for people with advanced COPD, typically friends or family members.4,5 Optimal disease-directed management of the underlying condition is often insufficient to adequately address the physical, emotional, and psychosocial needs of people with advanced COPD or the people who care for them. 6 Consequently, even amongst those who are able to access timely and high-quality disease-directed care, many will experience severe and prolonged unmet symptom needs.7,8
Palliative care is well placed to address the unmet needs of people living with advanced COPD, as well as the needs of the people who care for them. Despite this, international audits have demonstrated that fewer than 20% of decedents with COPD receive palliative care referrals.9–11 and these are often late in the illness trajectory when the ability for shared decision-making and planning is limited. 12
Professional consensus: current state of international guidelines and recommendations
The benefits of palliative care implemented early in the illness trajectory and integrated with existing generalist or specialist respiratory services are increasingly recognised in international clinical practice guidelines for the management of COPD.13 –17 The Global Strategy for the Diagnosis, Management, and Prevention of COPD (GOLD report) 16 is a regularly updated comprehensive document developed by an international collaboration of clinicians and public health experts that informs all aspects of COPD management. The 2024 GOLD report highlights inequity in palliative care access for people with COPD and details specific palliative approaches which should be considered not only at the immediate end of life but also to support symptom management throughout the illness trajectory. 16
International professional respiratory societies have similarly championed the need for palliative care with their own position statements. The American Thoracic Society (ATS) in partnership with a number of multi-disciplinary societies with interests in palliative care developed a 2022 position statement regarding integration of palliative care early in the care continuum for people with serious respiratory illness and provides a framework to support this goal. 14 The framework developed by ATS and partner organisations spans models of care, holistic symptom management, formalised discussion and documentation of goals of care, consideration of health inequities and carer needs, and responsiveness to crises. 14 The European Respiratory Society (ERS) has also called for consideration of palliative care that is integrated into routine respiratory care to support the physical, psychological, social and existential needs of people with COPD as well as their carers in a 2023 clinical practice guideline. 13 This guideline specifically acknowledged that although the evidence base consistently favoured conditional recommendations for palliative care, it was underpinned by studies that were of low to very low certainty, reflecting the lack of robust studies on the topic. 13 A further clinical practice guideline published in 2024 by the ERS addresses strategies for symptom-directed care for people with non-malignant chronic respiratory disease, including COPD, and recommends referral to multi-component, multi-disciplinary, symptom management services. 15 This recommendation highlights the potential of holistic and integrated care to improve patient outcomes with low associated healthcare expenditure and low risk to patients. 15
These recommendations from leading professional societies are also reflected in many government policy documents which name palliative care as a national priority in the management of chronic conditions. In Australia, a 2019 report outlining the national strategic framework for chronic conditions, including COPD, makes mention of palliative care under both the need for active engagement, which focuses on empowering patients to be shared decision makers in their care, as well as the need for accessible health services, which includes alternative models of delivery outside of traditional hospital services. 18 In the United Kingdom and United States, the National Institute for Health and Care Excellence (NICE) and the Department of Defence Veterans Affairs have each published guidelines specific to COPD that recommend multi-disciplinary care, including palliative care specialists.19,20
Generalist or specialist palliative care approach
Palliative care is needed throughout the disease trajectory of COPD and should be accessible early and concurrently with disease-directed therapies.21,22 Palliative care services are now available in both hospital-based and community-based settings, including inpatient consultation or palliative care beds, outpatient specialist clinics, residential and aged care facilities, general practices and patients’ homes.21,23 The Australian Palliative Care Service Development Guidelines stated that all health professionals who care for people with life-limiting diseases should be trained to have basic competencies in palliative care, including symptom management and discussions about prognosis and goals of treatment.21,24 This was also strongly recommended in the ATS statement on palliative care for patients with respiratory diseases in 2008. 22 When palliative care is provided by general practitioners, nurses, allied health professionals or medical specialists in other disciplines, it is referred to as ‘generalist palliative care’, ‘primary palliative care’ or ‘palliative care’.21,25,26
In contrast to ‘generalist’ palliative care, ‘specialist palliative care’ is comprised of a multi-disciplinary and multi-professional team of palliative care physicians, nurses and allied health professionals who have advanced skills, extensive experiences and training in providing palliative care to address more complex needs, issues or conflicts in a wide range of hospital-based and community-based settings.26,27 In addition, they also have roles in providing education, support and consultation to facilitate ‘generalist palliative care’.28,29
With the growing population living with chronic life-limiting illnesses and increasing needs for palliative care, a collaborative approach between specialist and generalist palliative care teams was proposed by Quil and Abernethy to expand the reach of palliative care services and empower clinicians from any medical discipline to proactively practice basic palliative care skills and integrate them into routine practices. 24 There are not enough palliative care specialists to meet the increasing demand for palliative care. Therefore, other medical specialists need to practice basic palliative care skills to make palliative care more accessible for patients and facilitate delivery of generalist palliative care. 24 This collaborative mixed model would encourage bidirectional education opportunities, enhance the interdisciplinary partnership and improve access to palliative care and healthcare costs.30,31
Barriers to accessing palliative care
Despite guidelines recommending early palliative care approaches as routine practice for patients with advanced COPD, access to palliative care services is limited, delayed and fragmented. 32 Several barriers have been identified related to patients, health professionals and systems. The unpredictable disease trajectory and lack of reliable prognostic tools make it challenging to prepare for sudden deterioration and introduce palliative care promptly.33,34 Patients and families receive little education about the disease’s nature and symptom palliation and are often not prepared for end-of-life care. 34 More importantly, this is a particularly vulnerable patient cohort who often experience multiple comorbidities, severe symptom burden, low socioeconomic status, psychosocial isolation and diverse geographical locations, which may prevent them from accessing timely and regular palliative care. 32
With multiple healthcare professionals (general practitioners, specialist physicians, nurses, allied health professionals, etc.) involved in COPD management, there is a lack of clarity in terms of who is responsible for initiating palliative care discussions and coordinating various services and appointments. 35 Unfortunately, without effective communication and coordination amongst health professionals, important aspects of patient-centred care and needs are neglected, compromising efficiency and continuity of care. Time constraints within clinical consultations and lack of training in palliative care for healthcare professionals are also limiting factors that reduce the quality of palliative care delivery and lead to poor therapeutic relationships.32,34,36,37
Furthermore, people with COPD have unique palliative care needs in physical, psychological and social domains, which are different from people with malignancy or other chronic conditions, and therefore may not respond to standard palliative care management. 13 Currently, there is no unified definition of the palliative care approach for COPD, nor are there consistent referral pathways that effectively integrate palliative care into the standard disease-directed management. The provision of palliative care is limited by the funding, resources and expertise available in the local healthcare systems. Therefore, the establishment of proactive integrated palliative care models needs to be innovative and practical to optimise the utilisation of local resources, strengthen team ownership, respond to diverse patients’ and carers’ needs and be readily accessible through flexible locations and modes of care delivery.
Aims and rationale
The evidence documenting palliative care needs amongst this group is well-established. What remains to be understood is how best to deliver palliative care to extend the reach of existing limited specialist resources, improve the understanding and acceptability of palliative care as a mode of supportive care that is not restricted to immediate end-of-life, and ultimately improve access to high-quality symptom-supportive care throughout the illness trajectory for people with COPD and the people who care for them. This review aims to examine core components of palliative care and existing models of proactive and integrated palliative care which leverage both specialist and generalist skillsets to better understand which models can best serve the needs of people with COPD.
Methods
This narrative review sought an overview of the relevant literature by searching MEDLINE for English-language original research reports, narrative reviews, and systematic reviews related to palliative care for people with COPD and multi-disciplinary models of care that integrated palliative care components. We only reviewed models of care that delivered palliative care management. In addition, we sought relevant clinical practice guidelines from international professional societies to describe current expert consensus on the topic. Thematic headings were developed from a broad reading of the literature with key reports described under each heading. References from reports of interest were also considered.
Proactive palliative care approaches
This section will describe the common goals of proactive palliative care that are frequently described in models of care for people with COPD (Figure 1).

Goals of proactive palliative care for people with COPD.
Advance care planning
Advance care planning (ACP) is an integral part of palliative care and should be introduced early into routine practice. Discussion and documentation of advanced care planning encourages people to share their ‘personal values, life goals, and preferences regarding future medical care’ with health professionals and trusted ones and ensures that the medical care they receive aligns with their wishes. 38 Important topics for consideration during ACP include the progressive nature of COPD, treatment preferences during hospital admissions (e.g. specifically wishes regarding receiving non-invasive ventilation, invasive ventilation or resuscitation), patient’s and carers’ understanding and preferences, and what end-of-life care might look like (particularly place of preferred death). 39 Importantly ACP is an iterative process, not only because it is difficult to cover everything in one discussion, but people’s preferences and views often evolve over time and may completely reverse. 40 Thus offering repeated opportunities to discuss ACP is critical. Effective ACP can avoid unnecessary, aggressive, life-sustaining treatment and hospitalisation, allow early palliative care planning and improve quality of end-of-life care with higher patient satisfaction and less surprises.41,42 More importantly, ACP eases anxiety, guilt and conflict amongst caregivers to make rushed decisions at the time of sudden deterioration.39,43,44
However, the initiation of ACP conversations can be challenging and are often delayed and poorly communicated. Several barriers have been identified, including unpredictable prognostication, time constraints to discuss ACP during a busy clinic consultation, lack of care coordination and continuity, limited training of healthcare professionals in ACP discussion and/or communication skills, and cultural and spiritual factors.36,40,45 Importantly, patients often report having a limited understanding of COPD and express a desire for open and honest conversations with clinicians in order to make individualised and informed decisions. 37 Unfortunately, many ACP discussions are initiated during acute exacerbations in hospitals with unfamiliar doctors in a chaotic environment. 46 This may add unnecessary distress to patients and carers and affect timely communication between secondary and primary care. 47 Moreover, health professionals find it challenging to engage end of life care (EOLC) conversations due to lack of training and clarity regarding their roles and responsibilities in ACP initiation and follow-up.36,48
To optimise the quality of ACP discussion and respond to patients’ needs, there is an increasing role for generalist palliative care in the community, particularly for patients in regional and rural settings.31,49 Patients with advanced COPD may benefit from community or home-based care programmes that can overcome psychosocial or geographical barriers and encourage their ongoing engagement. 50 A collaborative approach between general practitioners with specialist physicians, nurses and allied health professionals can facilitate an accessible and sustainable palliative care model. 31
Symptom palliation
Patients with advanced COPD often suffer from multiple comorbidities, leading to severe symptom burden, psychological distress and functional impairment. 8 Breathlessness is the most prominent and debilitating symptom experienced by patients.51,52 It is a subjective feeling that varies individually and may predict poor prognosis.53,54 However, it is often under-recognised and under-treated due to insidious symptom onset and poor understanding of disease trajectory. 55 Therefore, patients tend to normalise and adapt to the symptom by restricting their daily activities. 52 Chronic breathlessness syndrome is defined as severe and persistent breathlessness despite optimised disease-directed therapy, 56 which requires a multi-disciplinary approach to integrate both non-pharmacological and pharmacological interventions.17,57 Non-pharmacological interventions should be prioritised and optimised first with early referral to pulmonary rehabilitation, education on breathlessness exercise, and written self-management plans. 58 In addition, singing has also been trialled in patients with advanced respiratory conditions and has shown positive effects on well-being, enjoyment, social engagement and self-management.59,60 These strategies are greatly valued by patients and caregivers.
In regard to pharmacological management, low-dose (<30 mg daily) sustained-release oral opioids may be safe and effective to relieve refractory breathlessness.61,62 However, it is worth noting that current guideline recommendations are based on trials of stable outpatients, but opioids are frequently initiated in the inpatient setting after an acute exacerbation with lack of opioid education and delayed follow-up. 63 This is a particularly vulnerable group to treat. Therefore, careful initiation, slow titration, thorough education and prompt outpatient review are highly recommended to ensure safe opioid use in the community. 63
Furthermore, cough and fatigue are highly prevalent among patients with COPD. They commonly co-exist with breathlessness and complicate its management. 64 The burden of chronic cough is under-estimated and often normalised to be the consequence of smoking and disease progression. 65 Many factors, including physical and psychosocial, interact with fatigue, making it more challenging to provide effective symptom relief. The underlying aetiology and clinical assessments of fatigue remain unclear and heterogeneous. 66 To optimise symptom relief with tailored treatment, detailed screening of symptoms and their impact on quality of life and families should be integrated into routine practice. 66 Further research in comprehensive assessment tools and evaluation of their complex interaction is needed to gain a better understanding of symptom burden and to develop targeted treatment. 64
Support for caregivers
Caring for patients with COPD can be demanding and cause burnout, but carers have received little attention, resulting in significant physical, occupational and psychosocial burdens and negative family dynamics. 67 Carers play an essential role in improving treatment adherence, reducing exacerbations and supporting symptom palliation at home. 68 However, with increasing care dependency and responsibilities, carers have reported experiences of anxiety, helplessness, social isolation, worries for future uncertainty, and fear to discuss end-of-life treatment decisions. 69 As COPD patients may die suddenly and unexpectedly, bereavement support should be accessible and actively provided to all carers and families to reduce their anxiety, guilt and post-traumatic grief. 70
Existing palliative care models for advanced COPD
This section will describe the key models of care that have been implemented and evaluated for people with COPD (Figure 2). These models describe distinct but often overlapping components that aim to expand access to palliative care.
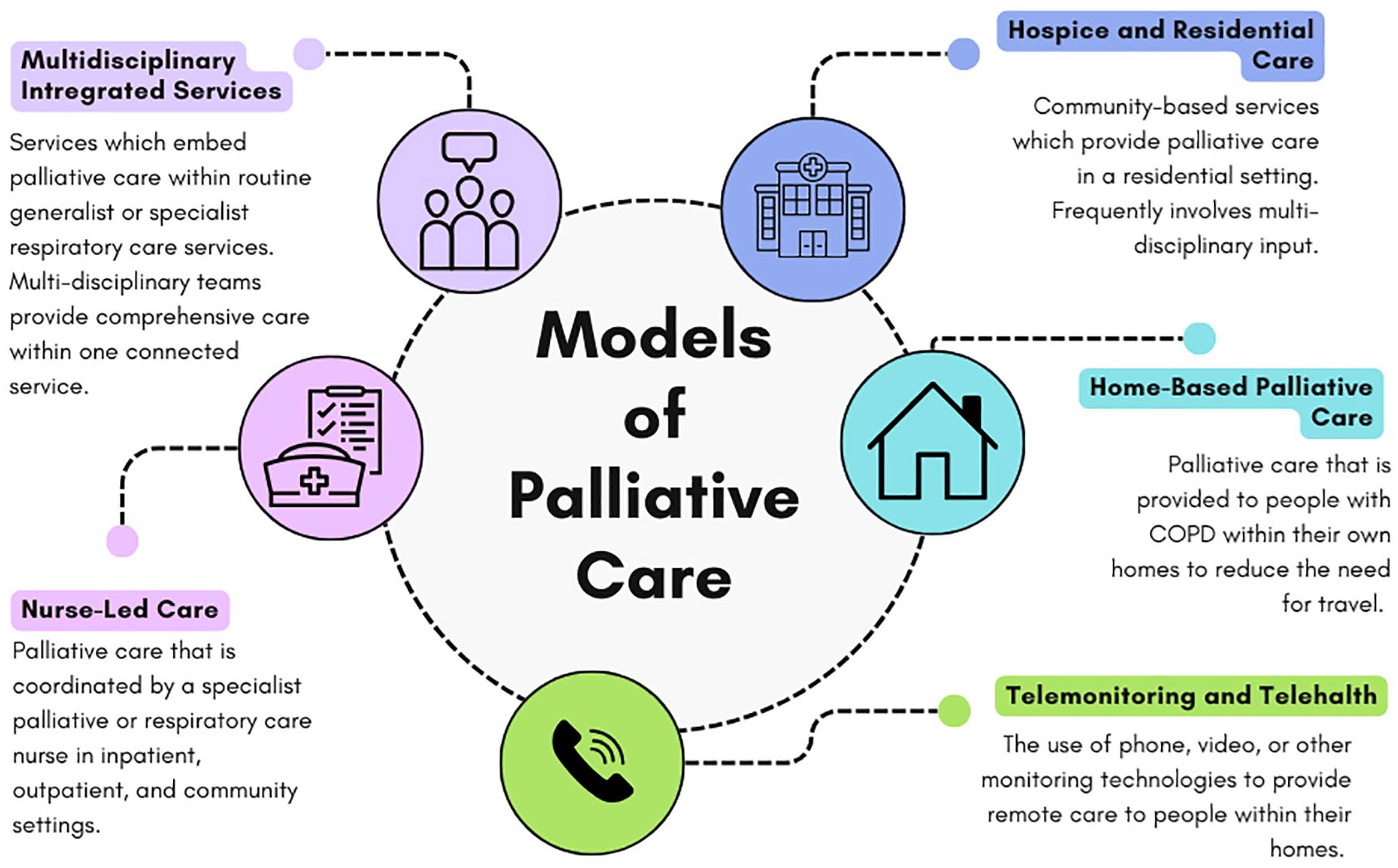
Models of palliative care for people with COPD.
Multi-disciplinary integrated services
There has been increasing emphasis on integrating palliative care into standard disease-directed optimisation approaches for people with non-malignant respiratory diseases. Multiple models of multi-disciplinary, multi-professional, single point-of-access services have emerged since the late 20th century71 –75 (Table 1). These services consist of palliative care and/or respiratory specialists for the initial face-to-face disease and symptom assessment, followed by regular counselling and review by nurses and allied health professionals via home visits or telephone consultations. The evidence-based non-pharmacological interventions have become an essential part of education and self-management, such as pulmonary rehabilitation, handheld fans, airway clearance and pacing techniques, cognitive behaviour therapy and psychosocial support. 17 These interventions may be offered together by an integrated breathlessness service to target the complex interaction between symptoms (breathlessness, anxiety, depression, fatigue, etc.) and improve symptom palliation.71 –75 Written information and crisis action plans tailored to individuals’ needs are also provided to patients and carers. 76 The team meets regularly to discuss individualised treatment plans and work closely with other medical specialists, primary care practitioners and community services (hospital support teams, rehabilitation programmes, aged care assessment, dietitians, community palliative care and hospices) to identify any gaps and ensure sustainable patient-centred care.71 –75
Summary of multi-disciplinary integrated services.

ACP, advance care planning; CRQ, Chronic Respiratory Disease Questionnaire; ED, emergency department; GP, general practitioners; MRC, Medical Research Council; N/A, not applicable; OT, occupational therapist; PT, physiotherapist; RCT, randomised controlled trials; SW, social worker.
The Cambridge Breathlessness Intervention Service (CBIS) was founded in 2003 in the department of palliative care at Addenbrooke’s Hospital, a tertiary referral centre in the United Kingdom. It comprises a palliative care specialist (as the service leader) and a clinical specialist physiotherapist or an occupational therapist. 73 The service focuses on optimisation of severe chronic breathlessness regardless of the underlying causes. They provide clinical assessment predominantly in the patient’s home or via phone calls. The service was developed and remodelled through phase I–III exploratory, feasibility, randomised controlled studies.77–79 The phase III fast-track randomised controlled trial was conducted over 4 weeks in people with advanced non-malignant diseases, with COPD being the most common diagnosis.79,80 The study demonstrated non-statistical improvements in distress, mastery in chronic breathlessness, and anxiety and depression in patients and carers. The CBIS resulted in minimal higher inpatient costs (£100) after excluding the outliers. 80 Patients and carers reported a positive impact on their emotions (reduced fear, anxiety and worry) and confidence in breathlessness management. Additionally, consumers highly valued the multi-disciplinary expertise and advice, positive and professional approaches, flexible locations and adequate time for counselling and reassurance. 80
Based on the CBIS model, the Breathlessness Support Service (BSS) was developed at King’s College Hospital in Southeast London, UK. The BSS served patients with refractory breathlessness (Medical Research Council (MRC) dyspnoea score ⩾2) despite optimisation of the underlying disease, including malignancy, cardiology, respiratory or neurological conditions. 81 Patients were referred from three large teaching hospitals and general practitioners. Different from the CBIS, the BSS was predominantly an outpatient clinic-based model, combined with home visits and telephone calls between clinics, and led by respiratory and palliative specialists jointly. 81 The service was extended to involve respiratory specialists to assess and optimise the underlying condition in the initial clinic. Other team members included a clinical nurse specialist and allied health professionals—a physiotherapist, an occupational therapist and a social worker, to facilitate adjustment to daily activities and tailor training and self-management strategies based on the home situation. 81 The fast-track randomised controlled trial of 105 patients referred to the BSS was conducted between 2010 and 2012. 71 There was a significant improvement (16%) and difference between the BSS and control groups in mastery of breathlessness measured by Chronic Respiratory Disease Questionnaire (CRQ) at 6 weeks. 71 The BSS intervention group also reported improvement in secondary outcomes - breathlessness severity, depression and daily activities, although they were not significantly different from the control group. There was no significant reduction in healthcare costs. 71 Qualitative interviews revealed that patients appreciated the patient-centred holistic approach of the BSS and found the interventions and recommendations acceptable and very helpful. 82
In 2010, Rocker and Cook implemented the INSPIRED community outreach programme in Canada for patients with advanced COPD. 74 The service offers home-based care bi-weekly from a respiratory therapist as the care coordinator, a community-based respirologist, and a spiritual care practitioner. The model is underpinned by an approach of continuity of care and non-abandonment. 74 In addition to provision of personalised breathlessness management, the INSPIRED programme also focuses on proactive in-home ACP as routine practice throughout the disease trajectory. 74 An observational mixed-methods study of the INSPIRED model suggested improved self-efficacy, confidence and engagement in care over 6 months, as well as significant and sustained cost savings from reduced emergency visits, hospital admissions and length of stay.83,84
In Australia, the Advanced Lung Disease Service (ALDS) was established in 2013 at the Royal Melbourne Hospital, a tertiary hospital, for patients with non-malignant respiratory diseases. 72 The service provides long-term hospital and home-based care and is also founded on an approach of continuity of care and non-abandonment. All patients are introduced to both respiratory and palliative care specialists in the ALDS clinic with respiratory specialists being the primary care provider. 72 The respiratory specialists in the ALDS clinic have completed basic palliative care training (e.g. clinical diploma or university postgraduate certificate in palliative medicine). 72 The ALDS also involves a psychologist, a nurse-led community outreach service and telehealth support to allow flexible follow-up tailored to patients’ needs and social situations. The service works collaboratively with ‘Hospital in the Home’, community respiratory and palliative care teams, and aged care assessment services. In particular, the ALDS offers shared care with general practitioners to encourage partnership with primary care. 72 The ALDS observational cohort study was the first study that showed longer-term results over 4 years. The ALDS results are consistent with those from RCTs and cohort studies, including improved end-of-life care, better access to palliative care specialist services, reduced emergency department visits, and increased engagement in advanced care planning. 72 Moreover, the mixed-methods prospective cohort study of ALDS patients with COPD showed a clinically significant improvement in breathlessness measured by the numeric rating score at 6 weeks. 85 Patients and carers reported high levels of satisfaction due to individualised breathlessness education, self-management, continuity of care, and reassurance that an acute episode of breathlessness would pass.85,86
Lastly, the Munich Breathlessness Service (MBS) commenced at the Munich University Hospital in 2014. 75 The MBS provided 6-week, short-term care for patients with refractory breathlessness due to any condition, with COPD being the most common diagnosis (75%). The service was led by palliative care physicians in conjunction with respiratory physicians (who assessed patients in the first appointment and switched to optional based on their needs), physiotherapists, psychologists, social workers and nurses.75,87 Patients attended two outpatient MBS appointments in the first and last week and four weekly 60-min community-based physiotherapy sessions in between clinics. Patients’ participation, treatment outcomes, care needs and advanced care planning were reviewed in the second appointment by palliative care clinicians to plan for future management, including referrals to allied health professionals and ongoing palliative care clinics. 75 Alongside the MBS, the fast-track RCT (BreathEase) of 183 patients was conducted from 2013 to 2015. 88 The study confirmed significant improvement in CRQ Mastery and CRQ quality of life in the treatment group. 88 Unfortunately, only half of the participants were able to complete the treatment within 6 weeks and about 12% were lost to follow-up in the treatment group.75,88 This reflects the real-world challenge of both delivering care and conducting clinical trials with patients experiencing severe illness and major symptom burden.
These five integrated palliative care services adopt a multi-disciplinary and multi-professional model of care tailored to patients’ complex symptom burden and diverse physical and psychosocial needs.71 –75 Patients and carers greatly benefited from professional expertise, personalised education, positive reassurance and continuity of care.80,82,84,85,88 Studies demonstrated significant improvements in breathlessness, quality of life, confidence in disease and symptom management, as well as symptom-related distress in patients and carers. Beyond the disease and symptom management, the mode of care delivery strengthened patients’ trust, engagement and commitment to ongoing care.71 –75 These breathlessness services provide a patient-centred and holistic approach that allows time for patients to tell their stories, variation in treatment components, and flexibility around patients’ physical and social needs.71 –75 Based on the CBIS study, Spathis et al. proposed the Breathing, Thinking, Functioning (BTF) clinical model to explain and address the complex neurophysiological nature of breathlessness and its interaction with patients’ emotions, perception and consequently negative behavioural changes, causing vicious cycles. 89 Therefore, the multi-modal interventions utilised in these services, integrating respiratory physiotherapy (breathing domain), psychological support (thinking domain), aids and behaviour adjustments (function domain), potentially inform the structure for breathlessness management and education in the future. 75
Nurse-led care
Long et al. conducted a prospective, mixed-method pilot study to evaluate the feasibility and effectiveness of an advanced practice nurse-led palliative care programme for patients with advanced stage COPD (GOLD stage III and IV) over 3 months. 90 The programme aimed to optimise the symptom triad of breathlessness, anxiety and depression. Fifteen patients were enrolled in a tertiary care respiratory clinic. They were provided with individualised pharmacological and non-pharmacological interventions via three outpatient appointments and telephone reviews. 90 The advanced practice nurse as the care coordinator was able to consult and update the palliative and pulmonary clinicians for the treatment plans. 90 Patients reported improvement in breathlessness and reduced anxiety and depression even without the use of antidepressants or anxiolytics. They all had positive experiences and wanted to follow-up long term. 90 Therefore, nurses and allied health professionals have a key role in symptom management and supporting people with COPD.
The HELP-COPD programme was developed in Scotland in 2012–2013 for patients recently admitted for an exacerbation of COPD. 91 The programme was coordinated by a specialist respiratory nurse (who had experience in respiratory and palliative care) and aimed to offer a holistic care approach via home visits and telephone consultation over 6 months. 91 Despite the positive feedback, 12 out of 44 (27%) patients withdrew from the study due to illness, death, or loss of contact, indicating the importance of trying to offer supportive care earlier in the illness trajectory. 91
Hospice and residential aged care services
Community palliative care services and hospice programmes can expand the reach of palliative care and enable patients to access care locally. These models are diverse in nature but frequently adopt a multi-disciplinary approach to provide comprehensive care. COPD-specific palliative and rehabilitation programmes have been developed in residential aged care and hospices to provide personalised pulmonary rehabilitation and facilitate end-of-life care.92,93 The multi-disciplinary geriatrician-led rehabilitation programme and the community hospice programme demonstrated improvement in function capacity, health status and reduction in hospitalisation. For patients in the hospice, they were more likely to receive end-of-life care at home or in the hospice based on their wishes. Notably, symptom management and carers’ stress were the two main reasons for referral to the community hospice programme. 92 However, the low enrolment rate in the community hospice programme might reflect patients’ and healthcare providers’ hesitance and reluctance in introducing palliative care, and misconceptions about the scope of palliative care management. More recently, a mixed-methods pilot study of the Multidisciplinary Breathlessness Support Service (MBSS) provided evidence for the feasibility and acceptability of hospice-based care. 94 The MBSS adopted the BTF clinical model to inform its management. Again, it highlighted challenges in referral, implementation and maintenance of services due to lack of clear referral pathways, limited access to primary care practitioners for safe prescribing, as well as patients’ willingness to accept palliative care referrals.
Home-based palliative care
Home-based palliative care represents a model of delivery which expands upon community and outpatient-based services to deliver palliative care services directly within the person’s home. Many people with COPD struggle to attend traditional consultations due to reduced mobility, lack of readily accessible and affordable transport options, and avoidance of public settings due to exposure to infection risk. 95 These services aim to reduce the treatment burden for people with COPD and their carers and support people to remain in their homes and communities.
A randomised controlled trial of nurse-led home-based hospice service in the United States, PhoenixCare, which enrolled 192 people with COPD or chronic heart failure who were within the last 2 years of life was effective in reducing symptom distress and unscheduled healthcare utilisation whilst improving physical functioning and quality of life. 96 Similar programmes piloted in Canada 97 and Switzerland 98 were unable to demonstrate effectiveness, yet a larger scale audit in Belgium which included over 58,000 decedents with COPD, of which 644 had received palliative home care demonstrated effectiveness at reducing hospitalisation and increasing odds of dying at home. 99
Telemonitoring and telehealth
Whilst services which provide in-home care are promising, they are extremely resource intensive for health services which can limit their capacity. Telehealth and other remote consultations are an alternative and lower-cost means of providing care at home. The use of telehealth for management of COPD is not a novel concept,100,101 however the COVID-19 pandemic necessarily increased familiarity and uptake of such services particularly in regards to end-of-life care.
An evaluation of a nurse-led telehealth palliative care intervention in the United States, Project EPIC, which consisted of six sessions mapped against commonly identified palliative care needs was shown to be feasible and acceptable for people with COPD and their carers. 102 Another feasibility study in Italy delivered follow-up telehealth consultations for people discharged after an exacerbation of COPD with high levels of reported patient satisfaction. 103 Although these pilot trials are promising, larger studies are necessary to determine effectiveness. Qualitative studies of both patients and clinicians indicate that future models should look towards blended care delivery with telehealth available as a means of providing low-cost and accessible follow-up support, but suggest that telehealth alone is not an adequate substitute for face-to-face consultations.103,104
Conclusion
Palliative care plays a significant role in the care of people with COPD and should be accessible early and concurrently with disease-directed therapies throughout the illness trajectory. This review highlighted the importance of proactive palliative care management and explored the provision of diverse palliative care models through generalist and/or specialist approaches via different delivery methods in a range of settings. The integrated multi-disciplinary services demonstrated their effectiveness, safety and feasibility by achieving improvements in disease and symptom burden, and high levels of satisfaction in patients and caregivers. It should be noted that the models described are often resource intensive and may be challenging to implement in low-resource healthcare services, particularly in low- and middle-income countries where COPD is highly prevalent and burdensome. The challenges of implementing integrated palliative care within low- and middle-income countries are not unique to COPD and cost-effectiveness and scalability remain a challenge even within high-income countries. A successful palliative care model must be practical, accessible, and innovative to respond to individuals’ complex and evolving needs, enhance interdisciplinary and interprofessional partnerships, and to optimise utilisation of local healthcare resources.