
Abstract
Background:
Chronic cough, defined as a cough lasting 8 or more weeks, affects up to 10% of adults. Refractory chronic cough (RCC) is a cough that is uncontrolled despite comprehensive investigation and treatment of comorbid conditions while unexplained chronic cough (UCC) is a cough with no identifiable cause despite extensive evaluation of comorbid conditions. RCC and UCC are often poorly controlled. Understanding individuals’ lived experience of the symptoms and impacts of these conditions may guide therapeutic strategies.
Objectives:
The primary objectives of this study were to assess respondents’ perceptions of the key symptoms of RCC and UCC and the impacts of RCC and UCC and their symptoms on well-being, health-related quality of life, work productivity, and social relationships.
Design:
Qualitative study.
Methods:
This study enrolled 30 adults with physician-diagnosed RCC or UCC. Two trained qualitative researchers conducted individual, in-depth telephone interviews using a semi-structured interview guide. Interviews were audio-recorded, transcribed, coded, and systematically analyzed to identify content themes.
Results:
A total of 15 respondents with RCC and 15 with UCC were included in the study. Many respondents had RCC or UCC for a long duration (median 9 years, range: 0–24). Half of the respondents reported having a coughing episode at least once daily. Only 40% of respondents reported that medication had improved their symptoms. In over half of the respondents, RCC or UCC hindered communication, caused embarrassment, frustration, and worry, and lowered quality of life. Perceptions of meaningful treatment benefits in RCC or UCC varied widely across respondents.
Conclusion:
RCC and UCC remained poorly managed in many individuals and were associated with a wide range of symptoms and cough triggers that hindered daily activities and reduced emotional well-being. Understanding individuals’ lived experiences may inform the development of RCC and UCC therapeutic strategies.
Plain language summary
Chronic cough, particularly refractory and unexplained chronic cough, remain poorly managed in many individuals and are associated with a wide range of symptoms and cough triggers that hinder daily activities and reduce emotional well-being. Currently there are no US Food and Drug Administration-approved treatments for refractory or unexplained chronic cough. Understanding the experience and treatment preferences of individuals with these conditions may help inform the development of new therapies and clarify the potential impact of such therapies on the lives of individuals with chronic cough. Using in-depth interviews, the present study comprehensively evaluated individuals’ experience with refractory or unexplained chronic cough and treatment priorities, a research area that has not been well-studied. This study detailed broad-ranging physical, behavioral, and emotional impacts of chronic cough, which hindered individuals’ social well-being.
Introduction
Chronic cough, defined in current clinical guidelines as a cough lasting 8 weeks or more,1–3 affects 4–10% of adults worldwide, with a higher prevalence in Europe and North America compared with other world regions. 4 Individuals with chronic cough often report uncontrollable bouts of coughing, sometimes in response to minor triggers, such as laughing, speaking, or changes in the ambient temperature. 5 Although smoking significantly increases the risk of chronic cough, chronic cough has an appreciable prevalence in individuals who have never smoked. 6 Among former or never smokers, chronic cough is associated with older age, female sex, abdominal obesity, exposure to environmental triggers, and underlying health conditions, including asthma, gastroesophageal reflux disease, upper airway cough syndrome, or bronchiectasis.6–8
Chronic cough frequently continues for years or decades, leading to substantial physical and emotional symptoms, including fatigue, urinary incontinence, cough syncope, dysphonia, depression, and anxiety. 9 In some individuals, cough persists despite extensive guideline-recommended evaluation and treatment of comorbidities, a condition referred to as refractory chronic cough (RCC). 1 An estimated 12–40% of adults with chronic cough have an unexplained chronic cough (UCC), in which an underlying cause of cough cannot be identified despite rigorous evaluation of comorbid conditions. 10
Cough hypersensitivity syndrome (CHS) or neurogenic cough encompasses the spectrum of cough-related conditions or unexplained cough.10,11 RCC and UCC are clinically challenging conditions that can be frustrating for both patients and clinicians. In the absence of US Food and Drug Administration-approved medications for RCC and UCC, patients with these conditions may receive therapeutic interventions, such as off-label use of medications and behavioral/speech therapy, but without adequate benefit.12,13 However, a range of new therapies for chronic cough are currently being evaluated, and optimism is growing regarding the potential to successfully manage cough that is refractory to standard treatments.14,15 The real-world success of chronic cough therapies may be affected by patient-related factors. 16 Therefore, understanding the experience and treatment preferences of individuals with RCC or UCC may help inform the development of new therapies and clarify the potential impact of such therapies on the lives of individuals with chronic cough.
Currently, evidence regarding individuals’ lived experience with RCC or UCC is limited. 17 While previous studies have evaluated treatment preferences among individuals with chronic cough due to severe asthma and COPD18–20; to our knowledge, none has assessed treatment preferences among individuals with RCC or UCC or attempted to quantify the minimum desired efficacy for chronic cough treatments. The objectives of this study were therefore to assess respondents’ perceptions of the key symptoms of RCC and UCC and the impacts of RCC and UCC and their symptoms on well-being, health-related quality of life, work productivity, and social relationships. Further objectives of the study were to identify respondents’ treatment priorities and to quantify respondents’ minimum desired and ideal treatment-related changes in chronic cough.
Methods
Study design and population
In this study, we conducted in-depth interviews regarding respondents’ experience with chronic cough and their expectations about the benefits of cough treatments. Interviews were conducted from February to November 2021 with 30 enrolled adults, aged 18 years or older, who had a physician-confirmed diagnosis of RCC or UCC and were able to read and understand English. To ensure that the study sample was representative of individuals with RCC or UCC, the following exclusion criteria were applied: (1) immunocompromised individuals, (2) diagnosis with chronic cough resulting from invasive respiratory tract instrumentation or smoking, (3) diagnosis with a comorbid condition that could exacerbate symptoms of chronic cough or confound interview results, (4) history of substance abuse within the past year, (5) psychiatric disorder that would interfere with the study interview, (6) exposure to someone with COVID-19-related symptoms or a positive test for COVID-19, and (7) participation in a study of an investigational medicinal product within the prior 30 days. Approval to conduct the study was granted by the institutional review boards of RTI Health Solutions and the study sites. Informed consent was conducted and documented for all interviews before carrying out interviews. In one study site (site 2), verbal informed consent was conducted; at the other study site (site 1), written informed consent was also conducted. An unsigned copy of the consent form was given to all study participants before conducting the study interview. The study follows the consolidated criteria for reporting qualitative reserach (COREQ) guidelines for qualitative research. 21
Participants were recruited through convenience sampling at two specialty clinics for chronic cough (site 1: Center for Cough, Largo, FL, USA and site 2: Northwestern University, Chicago, IL, USA) in the United States. Potentially eligible participants were identified through chart review or clinical evaluation at clinic visits; a standardized screening form was used to confirm respondents’ eligibility (Supplemental Appendix A). Soft targets for recruitment were used to enhance the diversity of the participant sample regarding age, sex, ethnicity, education, cough origin (treatment versus unexplained cough), and disease subgroups (gastroesophageal reflux disease, asthma, and upper airway cough syndrome).
In-depth interview
Recorded interviews of approximately 1 h were conducted by two experienced research RTI Health Solutions team members, one of whom led the discussion while the other recorded detailed field notes. Interviews were undertaken via a secure teleconference line or password-secured, web-based system. During the interview, a semi-structured interview guide was used to elicit participant responses concerning their experience with chronic cough symptoms, triggers, and impacts. The interview guide included open-ended and probing questions, such as the following: ‘What, if any, triggers do you experience that seem to cause or worsen your symptoms?’; ‘What, if anything, do your symptoms interfere with your ability to do?’; ‘Tell us about feelings or emotions you have experienced due to your experience with chronic cough.’
Respondents were also asked to describe the minimum meaningful change in cough intensity or frequency that they expected from new treatments. Interview guide questions were developed based on a targeted literature review on the symptoms and impacts of chronic cough that we conducted before study initiation (see Supplemental Appendix B for the search strategy). Audio recordings of the interviews were transcribed verbatim by a medical transcriptionist. Transcripts included no personal identifiers; a unique subject identification number was used instead of a name to identify study respondents.
Data analysis
Immediately following each interview, the two interviewers documented their thoughts regarding the interview’s themes, such as the respondent’s experience of symptoms and the respondents’ perceptions about the impacts of chronic cough. The same two interviewers then conducted a line-by-line coding of the interview transcript to identify key themes and responses using a coding framework. A saturation grid was developed to record all symptoms reported by respondents during the interview. Respondent demographics, clinical symptoms, and cough diagnoses were extracted from medical charts by the study investigators and used to describe the study population. A descriptive analysis of respondents’ response data was conducted using percentages, means, and medians to evaluate trends in the overall sample and by category of RCC and UCC.
Results
Characteristics of respondents with RCC or UCC
Respondents with RCC or UCC enrolled in this study were predominantly older, female, and White [mean (SD) age, 64.9 (12.4) years, 83% female, 87% White; Table 1]. Overall, 57% of respondents had experienced a chronic cough for 6 or more years.
Sociodemographic and clinical characteristics of respondents with refractory or unexplained chronic cough. a

Values are presented as n (%) unless otherwise indicated.
High school equivalent includes General Education Diploma (GED).
One response is missing because the patient did not know.
Symptoms and triggers of chronic cough
Regardless of the duration of diagnosis, respondents were precise in describing the characteristics of their cough. Less than half of the respondents (43%) reported having a productive cough or a cough that led to mucus or excessive mucus production and 57% described their cough as dry cough (Table 2).
Patient-reported symptoms of refractory or unexplained chronic cough. a

Values are presented as n (%).
GERD, gastroesophageal reflux disease; RCC, refractory chronic cough; UCC, unexplained chronic cough.
Cough frequency
Respondents highlighted the frequency of cough as a distinguishing aspect of the condition. Half of the respondents reported experiencing a coughing episode at least once daily, up to multiple times per hour, while other respondents reported experiencing coughing intermittently. Many respondents reported experiencing seasonal or day-to-day fluctuations in the frequency of cough, with some expressing frustration at the unpredictability of their coughing (Table 3).
Select quotations from respondents.

Cough severity
Cough severity was also a defining characteristic of respondents’ experience with this condition. Respondents described a spectrum of cough severity ranging from throat clearing to severe, uncontrollable coughing episodes or ‘fits’. Coughing ‘fits’ were described as embarrassing or frightening, as they could cause one to leak urine, gag, vomit, become short of breath, feel faint, or feel physically exhausted. Respondents expressed concern over how they may appear to others when they cough, even if the coughing is mild (Table 3).
Twelve respondents (40%) reported that, over time, their cough had become more frequent or severe or was accompanied by additional or changing symptoms. For example, some respondents had developed hoarseness or lowering of their voice. However, 13 respondents (43%) reported diminished cough severity following treatment.
Associated symptoms
RCC and UCC were associated with multiple symptoms, most frequently were the sensation of postnasal drip (80%), hoarseness or changes in voice (77%), tickle or lump in the throat (73%), shortness of breath (63%), excessive mucus (57%), and fatigue or tiredness (50%; Table 2). Respondents with RCC reported a similar frequency of symptoms as respondents with UCC. Many respondents reported experiencing multiple symptoms (Supplemental Table 1).
Respondents described some symptoms, such as hoarseness and postnasal drip, as irritating, while other symptoms were considered distressing or severe. For example, shortness of breath was described as frightening or potentially dangerous, as some respondents worried about not having enough air to live or stay conscious. Similarly, gagging or vomiting due to cough or coughing-related fatigue, sometimes related to sleep disruption, were described as disturbing or draining. Some respondents said that their coughing caused substantial physical discomfort (e.g. pulling a muscle, sore ribs, back pain), and several female respondents indicated that they experienced urinary incontinence during coughing. Respondents’ descriptions showed the distressing nature of chronic cough symptoms (Table 3).
Triggers
In some respondents, bouts of cough were unpredictable, while in others cough was caused or worsened by specific triggers. Among the cough triggers reported most often by patients were environmental irritants (67%; Table 4). Respondents cited an array of environmental irritants as cough triggers, including cold or warm ambient air, pollen, mold, dust, pet dander, air conditioning, and smells, such as bleach, spray cleaners, candles, fragrances, and diesel fumes (Table 3).
Patient-reported triggers of refractory or unexplained chronic cough. a
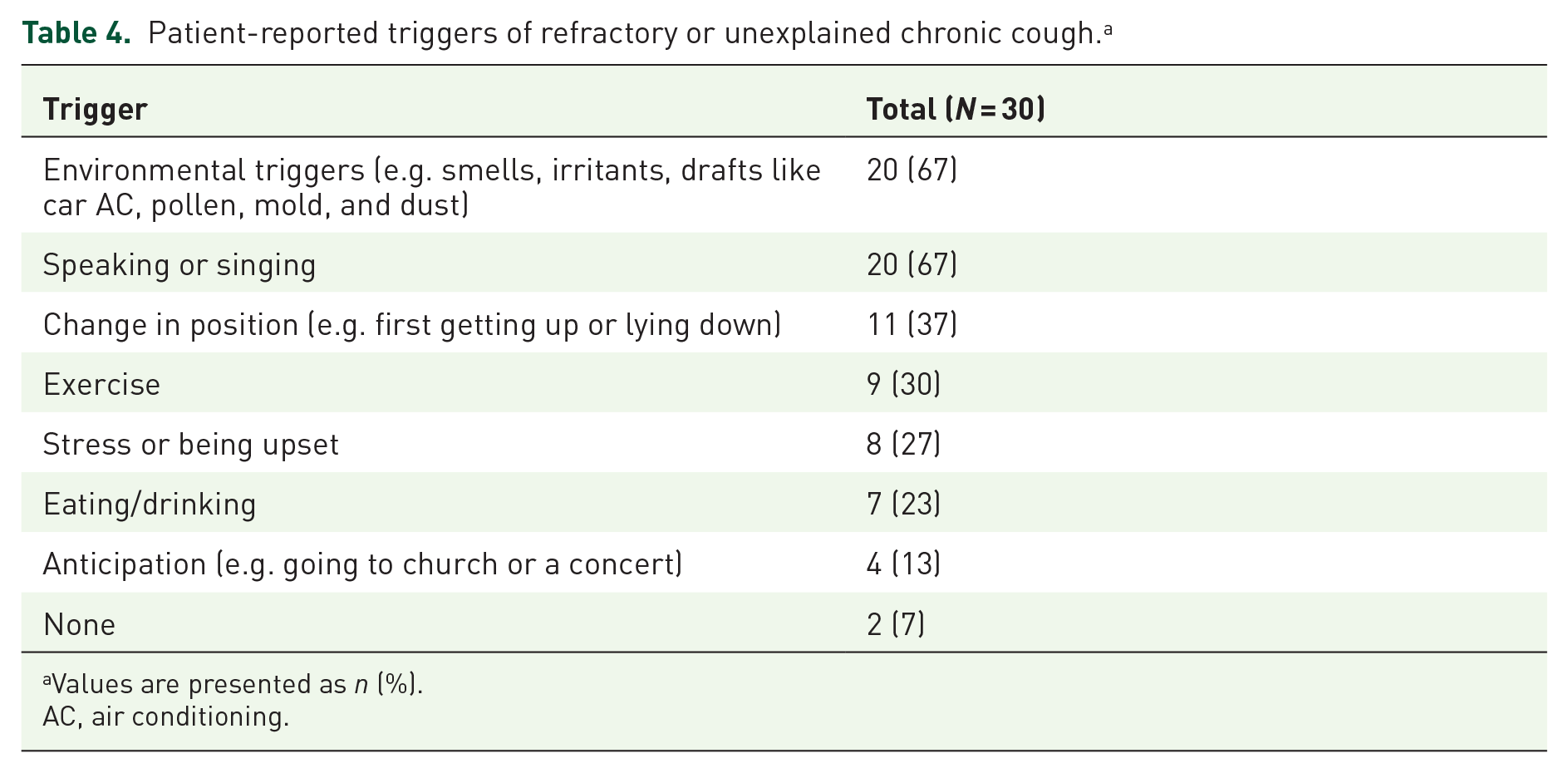
Values are presented as n (%).
AC, air conditioning.
Singing or speaking, especially when prolonged, excited, or loud, was also frequently cited as a cough trigger (67%; Table 4). Other cough triggers reported were changing body position (37%), exercise (30%), stress (27%), and eating or drinking (23%). These individuals reported having seen multiple specialists, in some cases over a period of years, before determining that their cough was due to hypersensitivity.
Psychosocial and behavioral impacts of chronic cough
Chronic cough affected respondents’ daily functioning, often hindering social interactions (Table 3). Over half of the respondents (57%) reported that coughing interfered with their ability to communicate, especially by phone or when talking for a long time, leading to strain in personal and professional relationships (Table 5). About one-third of respondents reported that coughing impeded their socializing, caused them to limit their social interactions with close family or friends, or triggered feelings of stigmatization. This trend was intensified by the COVID-19 pandemic. However, some respondents expressed determination to maintain social interactions despite their coughing.
Impact of refractory or unexplained chronic cough on daily activity and psychosocial well-being. a

Values are presented as n (%).
RCC, refractory chronic cough; UCC, unexplained chronic cough.
For almost half of the respondents (47%; Table 5), coughing disrupted their sleep or that of their partner, sometimes for years, leading to daytime tiredness and poorer quality of life. Notably, some respondents reported being so desensitized to their condition that they were unaware of their nighttime coughing. Some respondents reported cough-related impacts on food choices and participation in sports, exercise, or hobbies, but few reported impacts on productivity at work or home. The frequency of coughing-related impacts on daily function was similar among respondents with RCC and those with UCC.
Respondents reported that chronic cough contributed to negative emotions, compounding the burden of physical symptoms. Seventy percent of respondents expressed frustration at the persistence of their condition and the lack of effective treatments (Table 5). Many respondents (57%) reported feeling embarrassed by their cough, particularly during the COVID-19 pandemic; embarrassment was most frequently reported as the most burdensome symptom of chronic cough (Table 6). Worry, stigma, depression, anxiety, and irritability were other emotional impacts often reported by respondents, with nearly half indicating that cough diminished their quality of life (Table 5). The emotional distress caused by chronic cough was apparent in respondents’ comments (Table 3).
The most bothersome symptom and impact of refractory or unexplained cough as reported by patients. a

Values are presented as n (%).
The total sum of the percentages will be greater than 100% because respondents were allowed to report more than one symptom/impact.
Coping strategies for chronic cough
Respondents reported using various strategies to cope with chronic cough. Eight respondents reported the current use of one or more medications for symptom alleviation, including gabapentin, amitriptyline, inhalers, or antihistamines. Respondents also used non-pharmacological strategies, such as taking cough drops or lozenges, drinking water or a hot beverage, doing breathing exercises or relaxation techniques, and walking away to avoid disturbing others.
Perceptions of chronic cough treatments
Most respondents had sought medical treatment for their cough, with many reporting substantial delays in receiving a diagnosis. Fewer than half of the respondents (40%) reported having experienced an improvement in symptoms due to medication use.
Respondents expressed a range of views regarding their ideal cough treatment. Concerning treatment effects, most respondents (67%) prioritized improving the physical symptoms of cough over improving emotional well-being, noting that physical improvements would subsequently enhance social and emotional well-being. Most respondents cited reductions in the frequency or intensity of coughing or elimination of coughing as key characteristics by which they evaluate a new treatment. Some respondents stated they would evaluate a new treatment by weighing its effectiveness in reducing cough, cough severity, and cough-associated symptoms against the tolerability of treatment-related side effects.
Respondents’ minimum meaningful change in cough following a new treatment varied and appeared to be related to the severity of the respondent’s cough. A few respondents with intense or frequent coughing indicated that any reduction in cough frequency would be considered a meaningful change in their health state. For most respondents, however, a meaningful improvement meant a ‘noticeable’ improvement in their cough, with subjects noting a range of a 25–50% reduction in cough frequency. A few respondents reported that they had experienced a substantial improvement in the severity of their cough with a new treatment, with one respondent stating that he would expect future treatments to meet or exceed this benchmark. Some respondents described meaningful treatment-related changes in terms of their cough experience, such as no coughing at night, less frequent throat clearing, easier breathing, less mucus production, or less frequent medication dosing. Respondents’ comments show a wide variation in perceptions of meaningful treatment benefits (Table 3).
A conceptual model of chronic cough
The findings of a review of the chronic cough literature that we conducted were further informed by the current study. This, in turn, supported the development and refinement of a conceptual model of chronic cough symptoms, diagnosis, and impacts (Figure 1). This model highlights RCC and UCC as key diagnostic categories of chronic cough and shows the extensive impacts that chronic cough may have on respondents’ well-being, regardless of the underlying cause.

Conceptual model of chronic cough symptoms, diagnosis, and impacts.
Discussion
In this qualitative study, we evaluated individuals’ experience with RCC and UCC, finding that many had a persistent, debilitating cough that was sometimes so severe that it impacted their daily lives and activities and had emotional consequences. Respondents’ symptom burden was exacerbated by sequelae, including breathlessness, exhaustion, and physical pain. Extensive psychosocial impacts were also observed, as cough often hindered respondents from communicating or interacting with others and engendered feelings of frustration, embarrassment, and fear. A novel insight of this study is that patients’ expectations regarding meaningful treatment benefits appeared to vary according to the severity and frequency of cough.
In the current study, respondents highlighted the frequency and severity of cough as fundamental aspects of their experience with RCC or UCC. Other studies of RCC and UCC have similarly identified cough frequency as a defining characteristic of disease severity and a key determinant of patients’ psychological and social well-being.22–24 Similar to our study, other studies have also reported cough intensity and the physicality of intense coughing as key facets of individuals’ perception of the severity of chronic cough.17,23,24 We found that, for many individuals with RCC or UCC, the disruptive nature of cough was exacerbated by its unpredictability, a finding that accords with a 2021 observational study of UCC. 24 The wide range of chronic cough symptoms described in the current study, including hoarseness, fatigue, vomiting, and shortness of breath, have been widely observed in other studies of chronic cough,17,24–29 underscoring the importance of these symptoms to patients’ experience. Two findings of the current study, to our knowledge, have not previously been reported: RCC and UCC patient subgroups experience a similar frequency of symptoms, and a patient’s symptom profile may change over time.
Diminished communication emerged as the most frequently reported daily function impact of chronic cough, affecting over half of the study patients. This finding is consistent with the understanding that trivial mechanical exposures, such as talking and laughing, are key cough triggers in patients with cough hypersensitivity 30 and reports that interrupted conversations and loss of voice are common adverse effects of chronic cough.23,24,26,29 RCC and UCC further impacted the social dimension of individuals’ lives by engendering feelings of embarrassment and stigma, which were exacerbated by the COVID-19 pandemic and contributed to individuals’ limiting their social interactions. Similar findings concerning stigma and social isolation among patients with chronic cough have been reported by other studies,17,29,31,32 including a UK survey in which 64% of respondents stated that cough disrupted their social life. 28
In the present study, we found that cough disrupted sleep in 47% of respondents. In many,25,29,32,33 but not all studies, 24 sleep disruption has been identified as an important adverse impact of chronic cough, affecting 30–80% of respondents. However, the role of disturbed sleep in the well-being of individuals with chronic cough is complex. Sleep deprivation can hinder social functioning, 34 thereby contributing to social isolation among individuals with chronic cough. In contrast to other studies of chronic cough,35–37 few individuals in the current study reported cough-related impacts on work productivity, which may be because most were older adults who may have retired.
Frustration and worry were frequently reported by respondents in this study, as well as in other studies of chronic cough.17,24,28,29,32,38 These emotions may be linked to a challenging healthcare journey, which for refractory and idiopathic conditions, like RCC and UCC, is marked by delayed diagnosis and suboptimal treatment outcomes.39–42 Emotional impacts that are frequently reported in studies of chronic cough are feelings of vulnerability and hopelessness, fear, as well as depression, which affect 53–90% of patients with RCC or UCC.9,12,17,24,26,28,43,44 However, few individuals in the current study expressed feeling depressed, helpless, or hopeless, and indeed some conveyed a sense of humor and resiliency concerning their cough. These divergent findings may be due to differences in the psychological profiles of the patients or to differences in patients’ experience with cough treatments.
Previous research on treatment preferences in chronic cough indicates that patients prioritize easier dosing and administration, improvements in quality of life, and, as in the current study, reductions in physical symptoms.18,19 The range of perceptions regarding meaningful treatment benefits reported in this and other studies may reflect the multiple, and often inter-related, aspects of patients’ therapeutic experience, as well as differences in the phrasing of study questions. Most individuals in the current study considered a 25–50% reduction in cough severity as meaningful. A recent phase IIb study of RCC or UCC participants also found that a ⩾30% reduction in 24-h cough frequency is a meaningful change threshold to define treatment response in chronic cough clinical trials. 45 This information can be helpful in the development of future trials of RCC or UCC treatments.
This study has limitations. As this was a qualitative evaluation, findings were based on self-reported data, which may be subject to bias from patients’ desire to give socially acceptable responses. Enrollment was limited to two clinical sites offering state-of-the-art care; thus, the study may have underestimated the impacts of RCC and UCC that might have been observed in the general population not receiving this level of care. Furthermore, epidemiological and clinical diagnostic criteria used to define chronic cough vary. 46 A 2016 systematic literature review of publications between 1980 and 2013 included 70 studies with the majority (79%) of studies utilizing a ⩾3-month cutoff for chronic cough, 4% of studies using a ⩾8-week cutoff, and 16% studies not specifying a cutoff. 46 Future chronic cough studies should use a standard clinical definition of chronic cough that can be used across all chronic cough literature. In addition, the management of chronic cough is challenging and the success of management has varied. In a survey of 1120 individuals with chronic cough, only 30% of individuals felt that ‘their doctor had dealt with their cough thoroughly’. 47 Furthermore, the medication prescribed was judged as having limited (57%) or no effectiveness (36%). 47 While these results align with the results presented here, it is possible that the data captured here reporting that only 40% of respondents reported that medication had improved their symptoms, may not be reflective of a patient’s true treatment pathway as we do not know if the patient took the prescribed medications as directed.
Conclusion
This study comprehensively evaluated individuals’ experience with RCC or UCC and treatment priorities, a research area that has not been well-studied. Using in-depth interviews, this study detailed broad ranging physical, behavioral, and emotional impacts of chronic cough, which hindered individuals’ social well-being. This and other study findings enabled the elaboration of a conceptual model of chronic cough, highlighting the importance of cough as a disease entity, regardless of etiology. Key study insights on patients’ experience of cough and treatment preferences may inform the development of clinical interventions for RCC and UCC, including therapeutic drug trials.
Supplemental Material
sj-docx-2-tar-10.1177_17534666241236025 – Supplemental material for Patient-reported experiences with refractory or unexplained chronic cough: a qualitative analysis
Supplemental material, sj-docx-2-tar-10.1177_17534666241236025 for Patient-reported experiences with refractory or unexplained chronic cough: a qualitative analysis by Vishal Bali, Jonathan Schelfhout, Mandel R. Sher, Anju Tripathi Peters, Gayatri B. Patel, Margaret Mayorga, Diana Goss and Carla (DeMuro) Romano in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-3-tar-10.1177_17534666241236025 – Supplemental material for Patient-reported experiences with refractory or unexplained chronic cough: a qualitative analysis
Supplemental material, sj-docx-3-tar-10.1177_17534666241236025 for Patient-reported experiences with refractory or unexplained chronic cough: a qualitative analysis by Vishal Bali, Jonathan Schelfhout, Mandel R. Sher, Anju Tripathi Peters, Gayatri B. Patel, Margaret Mayorga, Diana Goss and Carla (DeMuro) Romano in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-1-tar-10.1177_17534666241236025 – Supplemental material for Patient-reported experiences with refractory or unexplained chronic cough: a qualitative analysis
Supplemental material, sj-pdf-1-tar-10.1177_17534666241236025 for Patient-reported experiences with refractory or unexplained chronic cough: a qualitative analysis by Vishal Bali, Jonathan Schelfhout, Mandel R. Sher, Anju Tripathi Peters, Gayatri B. Patel, Margaret Mayorga, Diana Goss and Carla (DeMuro) Romano in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
The authors thank Trina Cook of RTI Health Solutions, Research Triangle Park, NC for providing analytic support. The authors also thank Ingrid Peterson, PhD, in collaboration with ScribCo for medical writing assistance.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.