
Abstract
Primary lung cancer in childhood is extremely rare, with an incidence rate of less than 2/100,0000, and pulmonary mucoepidermoid carcinoma (PMEC), is even rarer. Their symptoms are usually not specific, and there are no guidelines for their management, which makes their clinical management a challenge for pediatricians. The purpose of this report is to discuss the clinical presentation, positive signs, examinations, pathological characteristics, surgical modalities, chemotherapy regimens, and prognosis in children. The clinical data of four patients diagnosed with PMEC at the Children’s Hospital of Chongqing Medical University from June 2021 to November 2022 were retrospectively analyzed, and their clinical features, treatment, and prognosis were summarized. Among them, two were male and two were female; their ages ranged from 3 years and 10 months to 10 years and 11 months, and all were staged according to tumor node metastasis classification (TNM). Immunohistochemical tests were performed in all children, among which four cases were positive for cytokeratin (CK), two cases were positive for CK7, four cases were positive for p63, about 5–10% of tumor cells were positive for Ki67. Among the four children, three had surgery alone and one had surgery + chemotherapy. All four children are presently living, with no evidence of tumor recurrence or metastasis. PMEC in children is very rare, and its age of onset and symptoms are not specific, and there is no obvious correlation with gender. Its diagnosis mainly relies on pathomorphological diagnosis, and immunohistochemical detection has no specific performance. The prognosis of children with PMEC is related to the clinical stage and whether surgery is performed. Whether further chemotherapy or radiotherapy is needed for patients who cannot undergo surgical resection and for those who have a combination of distant metastases requires further clinical studies.
Plain Language Summary
Lung cancer in childhood is extremely rare, occurring at a rate of less than 2/1000000, and a type of lung cancer called pulmonary mucoepidermoid carcinoma (PMEC), is even rarer. The symptoms are usually not specific, and there are no guidelines for its management, which is a challenge for doctors. The purpose of this report is to discuss the signs and symptoms medical examinations, disease characteristics, surgical procedures, chemotherapy regimens and prognosis in children with pulmonary mucoepidermoid carcinoma. The clinical data of four patients diagnosed with pulmonary mucoepidermoid carcinoma at the Children’s Hospital of Chongqing Medical University from June 2021 to November 2022 were analyzed, and their clinical features, treatment and prognosis were summarized. All four children are currently alive, and there is no recurrence or spread of the tumor after treatment. We have discussed various aspects of the disease, such as the rate of occurrence, causes, signs and symptoms, the way in which it might be diagnosed and treated, and the survival rate after operation, hoping to provide some insights for future work.
Introduction
Although lung cancer is one of the leading causes of cancer death in adults worldwide, it is rare in children and adolescents. In children, despite the more frequent occurrence of solid tumors, primary lung cancer is extremely rare, accounting for only about 25% of all pediatric primary lung tumors and 0.1% of all pediatric malignancies.1–3 In terms of primary lung cancer type, squamous cell carcinoma (SCC) is the most common lung cancer subtype in adults, followed by adenocarcinoma and small cell lung cancer, while Kraywinkel et al. 4 showed that it is pulmonary mucoepidermoid carcinoma (PMEC) that is the most common primary lung cancer in children.
However, the pathogenesis of the PMEC is not clear, and the environmental, smoking, occupational exposure, and chemical triggers in children are not as relevant as they are in adults, and it may be related to a genetic predisposition to cancer and developmental malformations of the lung airways.5–10 There are also no specific clinical signs and symptoms. Clinically, complete surgical resection is preferred, and the need for further chemotherapy or radiotherapy depends on clinical stage and pathologic staging. Most of the cases have a good prognosis. Studies of such disorders in children are mostly case reports, according to a review of the literature, and a complete international standard of care is not available. Hence, experts do not yet have a clear understanding of its clinical features, pathological characteristics, diagnostic and treatment strategies, and prognosis. In this study, we retrospectively summarized and analyzed four cases of PMEC diagnosed and treated in our hospital, in order to gain a deeper understanding of the characteristics of this disease in children and to provide some guidance for clinical work. This study retrospectively summarizes and analyzes four cases of children with PMEC diagnosed and treated in our hospital as a single-center study, in the hope of gaining a deeper understanding of the characteristics of this type of disease in children, and providing some guidance for clinical work.
PMEC is a relatively indolent tumor. Its survival rate is greatly influenced by TNM stage, pathological grade, and the presence of lymph node metastasis, and its prognosis is generally considered optimistic. In children, PMEC is more often seen as low-grade tumors, with stage I–II tumors being common. After complete surgical resection, survival is good, with low rates of recurrence and distant metastasis at long-term follow-up.
Materials and methods
We have followed the CARE guideline, which can be downloaded from here: The CARE Guidelines: Consensus-based Clinical Case Reporting Guideline Development | EQUATOR Network (equator-network.org). 11
Patients
From June 2021 to November 2022, a total of four cases of PMEC were admitted to our hospital. Relevant clinical data of these four cases were collected, and diagnosis relies on pathological confirmation. The study was conducted with the informed consent of the parents and approved by the Ethics Committee.
Database
Clinical data were collected from patients, including gender, age, symptoms, tumor location and size, tumor type, TNM stage, tissue sections, immunohistochemistry, treatment modality, outcome, last follow-up, underlying disease, and family history. The different treatment modalities included surgery, chemotherapy, and radiation therapy. Record events during treatment (tumor progression, recurrence, metastasis, second malignancy, or death). The status of the children and the disease during the follow-up after the end of treatment were determined.
Follow-up
Patients were followed up by telephone and outpatient review until 31 January 2023.
Results
From June 2021 to November 2022, four cases of PMEC were admitted to our hospital, and the basic information of the children is shown in Table 1. After admission, routine blood collection, chest CT, and bronchoscopy were performed to clarify the location and morphology of the lesion, as shown in Figure 1. Case 2 was biopsied under bronchoscopy, and the findings suggested the possibility of mucoepidermoid carcinoma, and the imaging data suggested that the tumor had no obvious site of preference. After close preoperative discussion, all four children underwent lobectomy (complete resection of the tumor) and lymph node dissection at the relevant location, and the postoperative pathological findings were all suggestive of pulmonary mucoepidermoid carcinoma, as detailed in Table 2 and Figure 1. In the pathological findings of the child in case 3, more nests of SCC were seen, so we followed the chemotherapy regimen associated with adult non-small cell lung cancer and gave six courses of chemotherapy with paclitaxel + cisplatin after complete resection of the tumor. Four children were followed up after surgery with good results and no recurrence or metastasis.
General information of the children.

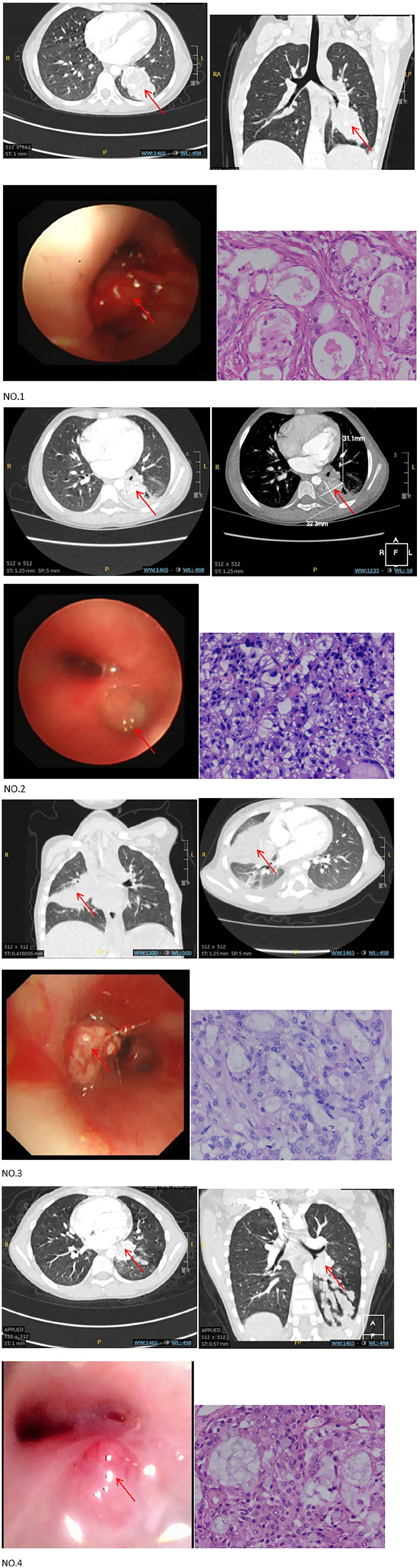
NO.1 to NO.4 represents the numbers of the four children. Each set of images included two CT imaging images, one bronchoscopic image, and one pathological findings. The arrows in the figure point out the location of the lesion.
Pathological and immunohistochemical characteristics.

Discussion
Although primary lung cancer is one of the most common causes of death in adults, it is very rare in adolescents and children. 12 Primary tumors account for less than 2% of congenital lung diseases in children, and the annual incidence of primary lung cancer in children is merely 1 in 2 million. 13
Firstly, the ratio of primary lung tumors to metastatic tumors to inflammatory/congenital lung disease has been reported to be 1:5:60 in children with lung disease. 12 An analysis of SEER registry data in the United States estimated that the annual incidence of primary lung cancer in children was 1 in 2 million. 13 And in this data set, it was shown that the majority were endocrine tumors (51.6%), followed by sarcomas (11%), mucinous epidermodysplasic carcinomas (9%), (pleural) pneumoblastomas (9%), adenocarcinomas (6%), SCCs (4.5%), and small cell carcinomas (4.5%). Secondly, it can be very difficult to identify primary lung tumors in children clinically, not only they are very rare, but also their clinical presentation is not clearly specific and may even mimic the nonspecific symptoms of common entities. 14 More worrisome is that many lesions are accidentally discovered during chest imaging examinations, which are often caused by completely unrelated diseases. 15 This was also reflected in our four children in this case, who did not have specific relevant clinical signs, thus making the diagnosis of an already rare-onset lung tumor in children more difficult.
The causes of lung tumors in children are still unclear, and the relatively rapid pathogenesis is more ambiguous. In terms of comparison of tumor occurrence time and tumor types, when adults discover tumors, individuals have already survived for decades, which also means that tumors have also experienced decades of occurrence, among which epithelial tumors (carcinomas) are most common, while childhood tumors start earlier, mostly develop within a few years or even months, and are mostly seen in mother cells or mesenchymal cells (sarcomas). Smoking, occupational exposure, chemical factors, and environmental carcinogen are the main risk factors for adult primary lung cancer, and are closely related to exposure duration. But these factors may not be important in primary tumors in children. 5 Instead, genetic susceptibility to cancer and congenital structural alterations play a dominant role in primary lung cancer in children. In related studies, cancer susceptibility syndromes (such as Li Frauemeni syndrome) have been shown to be associated with the occurrence of childhood lung cancer, and it has been reported that about 10% of childhood cancer patients show germ line mutations in precancerous genes.6–7 In addition, congenital structural lung diseases have been correlated with the development of lung cancer in children, such as congenital pulmonary airway malformations, recurrent respiratory papillomatosis and so on.8–10
The histological origin and tissue classification of PMEC are not well established, but because of their histological similarity to salivary gland tumors originating in the head and neck, these tumors are now thought to originate in the salivary glands of the tracheobronchial tree as a subclass of salivary gland-type tumors, which well explains the fact that PMEC are usually seen in segmental or large lobar bronchial. 16 Combined with the location of the onset of disease in the four cases in our group of studies, it also fits well and corroborates this well. In contrast, for salivary gland-type lung tumors, it has been recognized since the 1950s that they have the potential to develop ferociously and metastasize, and that they are less aggressive than the more common bronchial cancers.17–18
Since the symptoms, imaging features, and relevant clinical examinations of PMEC in children have no obvious specificity and relevance, the diagnosis of PMEC mainly relies on biopsy. Broadly speaking, PMEC tumors are tan or light brown polypoid masses. PMEC are histopathologically defined by a combination of squamous epithelial, mucous, and intermediate cells with defects in keratinization. It is common practice to classify PMEC into low-grade and high-grade tumors based on histologic appearance, mitotic frequency, cell isotype, and necrotic cells.19–21 Chin et al. 22 observed that high-grade tumors have a higher proportion of squamous epithelium. Invasion of adjacent lung parenchyma and regional lymph node involvement are more common in high-grade PMEC. Mutations t (11; 19) (q21; p13) that produce the MECT1-MAML2 fusion protein have been shown to be specific genetic events in PMEC pathogenesis. 23 The rearrangement of MAML2 is of great value in determining the diagnosis of difficult cases and correlates with poorly differentiated tumors. It has been shown that MECT1-MAML2 rearrangements are more common in low-grade PMEC than in high-grade PMEC.24–25 However, there was no specific indication of its role in patient survival, and it was not a relevant gene for its specific expression. The four children in this study had significant pathologic features and were very certain to have mucoepidermoid carcinoma at the pathological level, so our center did not further improve the detection of the relevant genes. This article is mentioned to inform doctors that while the pathologic diagnosis is relatively difficult, but highly suspected, further screening of the MAML2 gene can be considered to help the diagnosis.
For the treatment of PMEC, complete surgical resection is considered the main treatment strategy, which implies even better survival outcomes, especially for stage I–II PMEC. The surgical approach is mainly determined by the location of the tumor. If the tumor is located in the lobar bronchi, lobectomy is the most common surgical approach, and if it invades the main bronchi, sleeve lobectomy is considered. If incurable, a total pneumonectomy should be considered. Considering the slow growth and low metastatic potential of PMEC in children, it seems reasonable to perform nonradical, tissue-preserving surgery in most cases of PMEC. Most studies have concluded that surgical adjuvant radiotherapy or chemotherapy is not necessary for low-grade PMEC. 26 And there are no uniform guidelines or consensus for the treatment of chemotherapy and radiotherapy. For pediatric PMEC, if treatment other than surgery is required, it seems reasonable to adopt treatment strategies from adult practice and plan treatment in collaboration with the expertise of adult oncologists, as there is no evidence base for pediatric treatment. In case 3, because of the large number of SCC nests and the pathological grading tended to be poorly differentiated, and we took a more aggressive approach. The child was treated with chemotherapy after surgery. The chemotherapy regimen was based on the adult chemotherapy regimen for non-small cell lung cancer, and six courses of postoperative chemotherapy were administered with paclitaxel + cisplatin. The chemotherapy course was smooth, with no major chemotherapy adverse effects and good follow-up with no obvious signs of metastasis or recurrence. This is our insight into the treatment of mucoepidermoid carcinoma in children, and we hope that it will help to form a standard of care for children with mucoepidermoid carcinoma in the future. We will also conduct more long-term follow-up.
PMEC is a relatively indolent tumor. Its survival rate is greatly influenced by TMN stage, pathological grade, and the presence of lymph node metastasis, and its prognosis is generally considered optimistic. Because of its rarity in children, there is a lack of large data on survival rates. Analogously to related studies in adults, Zheng et al. showed in their study 27 that the five-year survival rate for patients with stage I–II tumors was 100%, with all deaths occurring in patients with stage III or IV tumors. In their study, it was shown that the 5-year survival rate for patients with high-grade tumors was only 28.6%, while the five-year survival rate for patients with low-grade tumors was 81.25%. Kang et al. 25 reported a five-year survival rate of 31% for high-grade PMEC and 80% for low-grade PMEC, and the recurrence rate for high-grade PMEC was as high as 80%. In the clinic, it was found that PMEC was more often seen as low-grade tumors, with stage I–II tumors being common in children. In children, after complete surgical resection, survival is good, with low rates of recurrence and distant metastasis at long-term follow-up. We consider that this may have more to do with the cause of tumor formation. Of course, this needs to be supported by more clinical data, which is what we are trying to do now.
However, because of the rarity of the disease, only four cases have been reported in our center, which has some limitations in forming a clinical diagnosis and treatment standard. In this paper, we only provide the relevant reports from a single center, and hope that it can provide some help to clinicians in the diagnosis and treatment process. In the future, we need to continue more in-depth research.
Conclusion
PMEC is very rare in children, and its clinical symptoms are atypical, mostly presenting as non-specific symptoms such as cough, howling wheeze, fever, chest pain, or even incidental findings on physical examination or incidental chest imaging. Chest CT is necessary in clinical diagnosis, and even further refinement of bronchoscopy and bronchoscopy aspiration biopsy is possible. Complete surgical resection is the treatment of choice, as it is a relatively inert tumor, and lymph node dissection is not routinely performed in the clinical setting. TNM stage, pathological grade, and the presence of lymph node metastasis determine to a certain extent whether further chemotherapy and radiotherapy are needed after surgery, which are not conventional treatments in children and are mostly referred to adult treatment strategies. Because of the early staging and low-grade pathology in children, the 5-year survival rate is high, and metastasis and recurrence are rare in the long-term follow-up.
Supplemental Material
sj-docx-1-tar-10.1177_17534666241258679 – Supplemental material for Clinical presentation and treatment of four children with pulmonary mucoepidermoid carcinoma
Supplemental material, sj-docx-1-tar-10.1177_17534666241258679 for Clinical presentation and treatment of four children with pulmonary mucoepidermoid carcinoma by Yiting Yang, Quan Wang, Zhengxia Pan, Hongbo Li, Yong An and Chun Wu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-jpg-2-tar-10.1177_17534666241258679 – Supplemental material for Clinical presentation and treatment of four children with pulmonary mucoepidermoid carcinoma
Supplemental material, sj-jpg-2-tar-10.1177_17534666241258679 for Clinical presentation and treatment of four children with pulmonary mucoepidermoid carcinoma by Yiting Yang, Quan Wang, Zhengxia Pan, Hongbo Li, Yong An and Chun Wu in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
I would like to thank the Children’s Hospital Affiliated to Chongqing Medical University for providing such a good platform for learning, scientific research, and clinical work. I would like to appreciate all the doctors and nurses of the Cardiothoracic Surgery Department of the Chongqing Medical University Affiliated Children’s Hospital for giving me so much advice and help. Thanks to my parents and family for companionship, support, and care.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.