
Abstract
Objective
This retrospective study investigated the effects of uterine manipulator use during minimally invasive radical hysterectomy on prognosis in patients with cervical cancer.
Methods
We collected clinical data on 762 patients with stage IA2 to IIB cervical cancer who underwent radical hysterectomy and pelvic lymphadenectomy in Chinese PLA General Hospital from 2009 to 2019. Kaplan–Meier analysis and log-rank tests were used to compare the 5-year overall survival rates between patients treated with and without a uterine manipulator.
Results
Patient demographics did not differ between the two groups. In addition, the incidence of lymphovascular space invasion, tumor size, pathologic types, the International Federation of Gynecology and Obstetrics stage, the histologic grade, and the rate of lymphatic metastases did not differ between the groups. Meanwhile, perioperative clinical indicators were similar in the groups. Furthermore, no significant differences in 5-year survival rates and survival curves were recorded between the groups among both all patients (84.5% vs. 85.6%) and early-stage patients (89.1% vs. 89.2%).
Conclusions
The use of uterine manipulators during minimally invasive radical hysterectomy for cervical cancer did not affect clinicopathological markers or increase the risk of death.
Keywords
Introduction
Cervical cancer is the fourth most common malignant tumor in women after breast, colorectal, and lung cancers,1,2 representing a serious threat to women’s health globally. In low- and middle-income countries, the morbidity of cervical cancer continues to increase, representing the leading cause of cancer death among women. 3 Radical hysterectomy with pelvic lymphadenectomy is recommended for early-stage cervical cancer (International Federation of Gynecology and Obstetrics [FIGO] stage IA–IIA). 4 With advances in medical technology, in addition to traditional laparotomy, laparoscopic surgery and robot-assisted laparoscopic surgery have been increasingly used in recent years. Compared with conventional laparotomy, minimally invasive surgery carries the advantages of less bleeding, less trauma, shorter hospital stays, fewer postoperative complications, and milder pain.5–8
In 2018, a New England Journal of Medicine study on early-stage cervical cancer treatment noted that patients who underwent minimally invasive surgery had lower survival rates and a higher recurrence risk than those who underwent open surgery.9,10 The unexpected outcomes of the series of studies have led to ongoing discussion about the ideal surgical methods for patients with cervical cancer. Gynecologic oncologists have proposed several hypotheses to explain the results. One hypothesis cited the instruments used in minimally invasive surgery, such as uterine manipulators. Uterine manipulators are among the primary instruments designed to improve the performance of laparoscopic hysterectomy. A variety of uterine manipulators have been developed to adapt to different uterine sizes and cervix shapes, making it easier to maneuver the uterus during laparoscopic surgery, as well as adequately expose the operative field and protect other pelvic organs. Nevertheless, these instruments can spread malignant cells by crushing the tumor, leading to lymphovascular space invasion (LVSI), which has been linked to metastasis after surgery in patients with cervical cancer.11,12 Pressure from the uterine manipulators can displace epithelial fragments within vessels or artifactual clefts. 13 In addition, uterine manipulators have the potential to disaggregate tumor cells, making tumors more susceptible to displacement into vascular spaces by pathologists during gross specimen processing. 14
It should be noted that this hypothesis lacks credible medical evidence. To explore the impact of uterine manipulators on the pathologic outcomes, especially LVSI rates and prognosis, in patients with cervical cancer, this retrospective study compared perioperative characteristics, pathologic results, and recurrence and survival rates in patients with cervical cancer according to the use of uterine manipulators.
Materials and methods
Patient selection
This single-center, retrospective, observational study was conducted in the Department of Gynecology and Obstetrics at Chinese PLA General Hospital. We reviewed the electronic medical records of patients who underwent minimally invasive surgical treatment for cervical cancer from January 2009 to December 2019. The reporting of this study conforms to the CONSORT guidelines. 15 The study was approved by the ethics committee of Chinese PLA General Hospital (Ethics number: S2021-329-02; approval date: 25 August 2021). The clinical trial identifier is ChiCTR2100052898 (06/11/2021) (Chinese Clinical Trials Registry Platform, http://www.chictr.org.cn/). Written informed consent was obtained from the patients. We have de-identified all patient details.
The inclusion criteria were as follows: age ≥ 18 years, execution of radical hysterectomy with pelvic lymph node dissection, pathological diagnosis of stage IA2 to IIB cervical carcinoma, and follow-up for at least 12 months.
The exclusion criteria were as follows: history of multiple primary malignancies and previous pelvic or abdominal radiotherapy, pregnancy, severe original disease, and previous subtotal hysterectomy.
Grouping method
The included patients were separated into the uterine manipulator group (UM) and non-uterine manipulator group (NUM) according to the use of a uterine manipulator during surgery. We extracted patients’ clinical data, including age, body mass index (BMI), FIGO stage (2009 system), tumor grade, tumor size, pathologic type, depth of cervical stromal invasion, number of resected pelvic lymph nodes, lymph node metastasis, length of the removed vagina, LVSI, parametrial involvement, and vaginal margin status. We used follow-up procedures to maintain patient confidentiality and provide disease management guidance. The follow-up information, including survival status and time of death, was gathered through telephone follow-up and the China National Death Reporting system covering in-hospital and out-of-hospital deaths in China. 16
All enrolled patients underwent laparoscopic or robotic radical hysterectomy and bilateral pelvic lymphadenectomy. The reservation of unilateral or bilateral ovaries was negotiated with each patient and her family using the criteria of age ≤45 years and pathologic diagnosis of squamous carcinoma. The use of a uterine manipulator was based on the surgeon’s preference. The Hohl manipulator (Karl Storz Gmbh and Co., Tuttlingen, Germany.) or Clermont Ferrand manipulator (Karl Storz Gmbh and Co.) was used during the radical treatment of cervical cancer as required. All surgeries were performed by experienced gynecologists, each of whom performed at least 30 radical cervical cancer surgeries per year.
Statistical analysis
The primary outcome measure was the 5-year overall survival (OS) rate. We defined OS as the time from the operation to death from any cause or last contact. We compared patients’ clinical and pathological characteristics between the groups. Student’s t-test was performed to compare continuous normally distributed variables. The Wilcoxon rank-sum test was performed to compare continuous variables that were not normally distributed. Categorical data including FIGO stage (IA2, IB1, IB2, IIA1, IIA2, IIB), histologic grade (I, II, III, unknown), depth of cervical invasion (≤1/2, >1/2), histologic type (squamous cell, adenocarcinoma, others), pelvic node involvement (positive or negative), vaginal margin status (positive or negative), and parametrial involvement (positive or negative) were compared using the χ2 test or Fisher’s exact test. Statistical significance was defined as P < 0.05 (two-tailed comparison). Kaplan–Meier survival curves for OS were generated and compared between the groups using the log-rank test. The Cox proportional risk model was used to identify independent risk factors and calculate hazard ratios and 95% confidence intervals. Statistical analysis was performed using SPSS software (version 24.0, IBM Corp., Armonk, NY, USA).
Results
We collected clinical data for 762 patients with cervical cancer who underwent radical hysterectomy and pelvic lymphadenectomy in our center from 2009 to 2019. Of the patients, 439 underwent surgery using a uterine manipulator. Patient demographics did not significantly differ between the two groups, including the age distribution (P = 0.940) and mean BMI (24.32 vs. 24.08, P = 0.336). In addition, the patients’ FIGO stage (P = 0.358) and pathologic type (P = 0.513) were similar between the groups (Table 1). The disease stage was IA2 to IB2 in 62.9% and 56.3% of patients in the UM and NUM groups, respectively. Squamous cell carcinoma and adenocarcinoma were the main pathological types. In particular, 83.4% and 84.8% of patients in the UM and NUM groups, respectively, had squamous cell carcinoma, whereas 10.0% and 10.5% of patients in these groups, respectively, had adenocarcinoma (P = 0.513). Meanwhile, 6.6% and 4.6% of patients in the UM and NUM groups, respectively, had other specific pathological types, including adenosquamous carcinoma, neuroendocrine carcinoma, and clear cell carcinoma. The histologic grades were similar in the two groups as grades II and III accounted for 87.7% and 86.1% of all diagnoses (P = 0.717), respectively. Moreover, we compared the risk factors for disease recurrence, including tumor size, depth of invasion, rates of lymphatic metastases, parametrial involvement, and vaginal margin status (Table 1). There were no significant differences in the tumor size distribution (P = 0.301), depth of invasion (P = 0.303), rate of parametrial involvement (3.6% vs. 2.2%, P = 0.239), rate of lymph node positivity (20.5% vs. 18.0%, P = 0.380), and rate of positive vaginal margins (1.4% vs. 0.9%, P = 0.580) between the UM and NUM groups. In addition, the length of the removed vagina was comparable between the groups (1.72 cm vs. 1.81 cm, P = 0.69, Table 1).
Clinicopathological characteristics of patients with cervical cancer according to the use of uterine manipulators.

UM, uterine manipulator group; NUM, non-uterine manipulator group; BMI, body mass index.
Furthermore, we compared the perioperative parameters of patients with cervical cancer. A similar number of lymph nodes was retrieved in both groups (20.58 vs. 19.39, P = 0.087, Table 2). We also reviewed the medical records of the enrolled patients. As presented in Table 2, the operative time was longer in the UM group (P < 0.001), and this group exhibited less blood loss (208.74 mL vs. 281.05 mL, P = 0.004). The two groups had similar postsurgical recovery times, including the length of postoperative hospital stay and time to first flatus. We did not find complications associated with uterine manipulators.
Perioperative parameters of patients with cervical cancer according to the use of uterine manipulators.

UM, uterine manipulator group; MUM, non-uterine manipulator group; LVSI, lymphovascular space invasion.
The median follow-up times were 66 and 63 months in the UM and NUM groups, respectively. In the UM group, 5-year OS rates were 97.1%, 89.6%, 82.9%, 83.7%, 75.0%, and 70.4% in stages IA2, IB1, IB2, IIA1, IIA2, and IIB, respectively. Meanwhile, the respective rates in the NUM group were 100.0%, 89.0%, 82.8%, 79.7%, 82.2%, and 82.1%. However, survival rates did not differ between the two groups (Table 3). Moreover, we generated survival curves for the two groups, and no difference in survival was detected between the groups (P = 0.760, Figure 1). As some studies advocated, minimally invasive radical hysterectomy was associated with lower rates of disease-free survival and OS than open abdominal radical hysterectomy among women with early-stage cervical cancer in whom uterine manipulators were used. We also compared the OS rate among stages IA2 to IB, and there was also no significant difference between the groups (P = 0.938, Figure 2). Cox survival analysis identified the depth of invasion, LVSI, pelvic lymph node positivity, and particular pathologic type as independent prognostic factors for patients with cervical cancer (Table 4). For patients with stage IA2 to IB cervical cancer, pelvic lymph node positivity, parametrial invasion, and tumor diameter influenced their prognosis. The use of a uterine manipulator was not an independent prognostic factor in patients with cervical cancer.
Overall survival rate by stage.

UM, uterine manipulator group; MUM, non-uterine manipulator group.
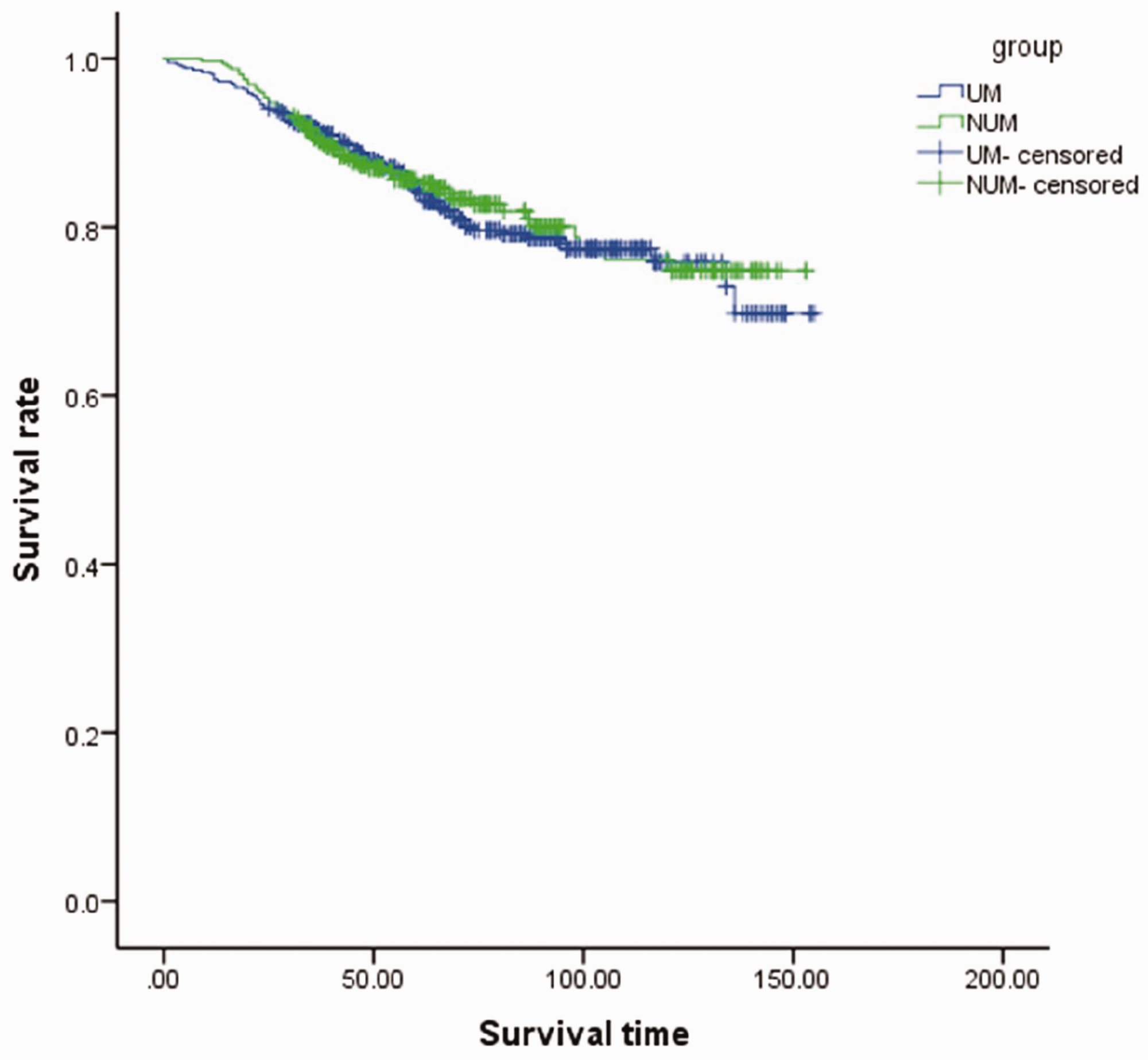
The Kaplan–Meier survival curves of the entire cohort. NUM, non-uterine manipulator group; UM, uterine manipulator group.

The Kaplan–Meier survival curves of patients with stage IA2 or IB cervical cancer. NUM, non-uterine manipulator group; UM, uterine manipulator group.
Multivariate analysis of the associations of potential prognostic factors with survival in patients with cervical cancer.

UM, uterine manipulator group; MUM, non-uterine manipulator group; LVSI, lymphovascular space invasion; HR, hazard ratio; CI, confidence interval.
Discussion
In this study, we investigated the relationships of the use of uterine manipulators during radical surgery for cervical cancer with postoperative pathologic results and patient prognosis. The results revealed that the incidence of LVSI was similar irrespective of the use of uterine manipulators in patients with similar tumor sizes, pathologic types, FIGO stages, and histologic grades. Meanwhile, 5-year survival rates and survival curves did not differ between the two groups for both all patients and only early-stage patients. Our study cannot prove the causation between the use of uterine manipulators and the increased risk of death in patients with cervical cancer who underwent minimally invasive surgery.
Since the invention of uterine manipulators, many gynecologic surgeons have appreciated their benefits in hysterectomy procedures. They noticeably improve the visualization of key anatomic structures and facilitate operation cooperation throughout the dissection. 17 However, the safety of uterine manipulators in patients with malignant tumors remains controversial. Especially after the LACC trial was reported, minimally invasive radical hysterectomy was considered an independent risk factor in patients with early-stage cervical cancer. Gynecologic oncologists proposed several hypotheses to explain the results concerning the dissemination of malignant cells into the peritoneal cavity in laparoscopic surgery performed using a uterine manipulator. It was reported that more malignant cells were present in the peritoneal washings of patients treated with uterine manipulators throughout endometrial cancer surgery, potentially increasing the risk of disease recurrence. 18 According to this study, tubal ligation was recommended before using the manipulators to help reduce the rate of positive cytology tests after the insertion of uterine manipulators.18,19 Meanwhile, some studies did not find that uterine manipulators increased the positive peritoneal cytology examination rate.20,21 In addition, several observational and prospective studies have verified the safety of using uterine manipulators in radical robotic or laparoscopic surgery for cervical cancer.22–25 Some studies examined the relationship between clinicopathological parameters and the use of uterine manipulators during radical surgery for cervical cancer and identified no significant difference in histologic parameters, including the incidence of LVSI, according to the use of a manipulator.26–28 These studies also reported no consistent evidence that uterine manipulators were associated with cancer recurrence and disease-specific survival.29,30 In our study, we did not find that uterine manipulator use affected the rate of LVSI and other clinical pathologic parameters, consistent with the results of previous studies. However, some surgeons developed several techniques to replace uterine manipulators during laparoscopic or robotic hysterectomy.31–34 These techniques have limitations such as complex procedures and the need for special equipment or specialized staff training, resulting in longer operative times or greater labor and financial costs. To date, uterine manipulators have been considered the best modalities for mobilizing the uterus. They expose the pelvis and push the uterus away from vital structures, facilitating laparoscopic hysterectomy, particularly in large uteri. Our study found that the use of uterine manipulators during laparoscopic or robotic surgery did not increase the risk of recurrence and death. Thereby, they are safe and effective for use in radical surgery for cervical cancer.
This was a single-center study, which might have resulted in bias in case selection. However, this would be advantageous in other aspects, such as controlling the influence of factors other than uterine manipulators, including surgeons’ skills, postoperative care, and adjuvant therapies. Moreover, this study had a large sample size and long follow-up period, and thus, we believe this research is compelling. However, we acknowledge several limitations. First, we included patients with stage IB2 to IIB cervical cancer who underwent radical hysterectomy. However, in other countries, radical radiotherapy would have been recommended for most of these patients, indicating that our conclusions are not broadly applicable. Nevertheless, a considerable number of patients with stage IB2 or IIB cervical cancer would choose surgery as the primary treatment in Asia and parts of Europe. Thus, we deemed it necessary to investigate their outcomes. This study was retrospective, as it is challenging to organize a large randomized controlled trial under current conditions.
Conclusions
In this study, we assessed the value of potential prognostic factors, including the use of uterine manipulators, for predicting the OS rate of patients with cervical cancer. The use of uterine manipulators was not found to influence prognosis in this study. This large retrospective study adds evidence of the safety of uterine manipulators in malignant gynecological tumor operations. However, more studies are required to clarify the indications and contraindications for uterine manipulators.
Footnotes
Acknowledgements
We wish to acknowledge the support of Nankai University and Chinese PLA General Hospital.
Authors’ contributions
Availability of data and materials
The data underlying this article cannot be shared publicly because of the privacy of individuals who participated in the study. The data will be shared on reasonable request to the corresponding author.
Declaration of conflicting interests
All authors declare no competing interests.
Funding
This study was supported by the National High-tech Research and Development Program (No. 2015AA020402).