
Abstract
Background:
The adverse effects of pulmonary arterial hypertension (PAH) on physical, emotional, and health-related quality of life (HRQoL) remain primarily unrecognized, especially in resource-limited settings.
Objectives:
This study aims to characterize the HRQoL of patients with PAH in this area and also identify the potential role of clinically relevant characteristics, including the 6-min walk distance test (6MWD), WHO-Functional Classification (WHO-FC), and mental health in the occurrence of lowering quality of life.
Design:
This was a cross-sectional observational study.
Methods:
Inpatients with PAH were chosen from a tertiary hospital located in Gansu province, China. All participants were interviewed face-by-face by using questionnaires, including items from the 36-Item Short Form Health Survey (SF-36), the self-rating anxiety scale, and the self-rating depression scale. Data on demographic and clinically relevant characteristics, including WHO-FC and 6MWD, were also collected by tracing medical recorders. Multiple linear regression analysis was used to determine the association between demographic, clinically relevant characteristics data, and physical component summary (PCS) or mental component summary (MCS) in SF-36.
Results:
Of the 152 participants, SF-36 differed significantly from Chinese norms in all eight domains, with role-physical (21.55 ± 9.87) less than one-third of the norm (88.79 ± 28.49). Multiple linear regression results showed that the factors with the greatest impact on PCS were anxiety scores (β = −0.22, p = 0.001), followed by WHO-FC (β = −0.16, p = 0.014) and 6MWD (β = 0.15, p = 0.036). The factors with the greatest impact on MCS were WHO-FC (β = −0.30, p < 0.001), followed by anxiety (β = −0.23, p = 0.001) and depression scores (β = −0.16, p = 0.013).
Conclusion:
HRQoL was substantially reduced among PAH patients in the resource-limited area, mainly the physiological functions. WHO-FC and anxiety scores were independently associated with both PCS and MCS in SF-36. Clinicians should make reasonable rehabilitation programs and plans for patients according to their cardiac function grade and the severity of clinical symptoms. In addition, psychological interventions should also be taken, especially for those with anxiety symptoms, so as to improve their HRQoL.
Background
Disease overview and treatment advances
Pulmonary arterial hypertension (PAH) is a rare, progressive pulmonary vascular disease 1 with a median survival of 5–7 years. 2 Patients with PAH may exhibit features of heart failure due to the decompensation of the right ventricle in the face of elevated pulmonary vascular resistance. 1 Despite traditionally considered to be a rapidly progressive and fatal disease, 1 new PAH-targeted treatments have shown reduced mortality rates, symptom burden, and increased functional capacity in PAH to varying degrees. 2 Consequently, the goals of PAH therapy have shifted from therapeutic objectives to longer-term improvements and health-related quality of life (HRQoL) benefits. 3
HRQoL importance
HRQoL is an important clinical end-point, economic factor, and predictor of prognosis in PAH.1,4 Although the adverse effect of disease symptoms on the physical, emotional, and HRQoL remained largely unrecognized, some clinical factors seem to be highly associated with these outcomes, such as 6-min walk distance test (6MWD), WHO-Functional Classification (WHO-FC), and mental health (MH) (anxiety and depression).2,5,6 Studies have shown that a decline in 6MWD associated with poor HRQoL in PAH.4,7–9 Also, one study indicated that each increase in WHO-FC was associated with a 10-point decline in the overall HRQoL among PAH. 10 In addition, depression and anxiety were common in patients with PAH, which have been shown to have a negative impact on HRQoL in PAH.11,12 Thus, these clinically relevant characteristics become significant predictors for assessing HRQoL or monitoring the disease in PAH.
In addition, the distribution of factors related to HRQoL in PAH varies widely in different regions, levels of economic development, and urbanization.8,13,14 For example, a study in Gansu, China, reported an apparent heterogeneity in the quality of rural life toward hypertension depending on urbanization and altitude. 15 In contrast, depression prevalence seems to decrease with altitude. 16 A study in Colombia also found that living at high altitudes was associated with lower QoL for older adults. 17 A study reported that chronic exposure to high-altitude environments might impact cardiovascular health and disease development, 18 and also the high altitude was positively related to the prevalence of PAH.14,19 All these findings encourage further study of health outcomes with populations living at higher altitudes.
Research gap
For establishing health priorities, especially in resource-constrained settings, it is important to understand the local epidemiology of HRQoL, including within-country heterogeneity. 20 This information may provide evidence to establish suitable interventions, goals, and targets. The present study was produced in Gansu province, China. Gansu lies in the western part of the Loess Plateau and is a transitional area from the Tibetan Plateau to the Loess Plateau. Its altitude ranges between 1500 and 2500 m above sea level, which is commonly defined as high altitude (1500–3500 m). 21 In 2017, Gansu Provincial Hospital took the lead in setting up a pulmonary hypertension clinic in the province, so this group of people has been paid attention. As affected by the regional conditions, the economy and information in Gansu have been relatively less developed, which may further impact the awareness and management of PAH. Currently, the prevalence of PAH in the residents has not been reported. With the standardization of diagnosis and treatment, the number of patients with PAH is increasing. There is also an increasing awareness of the importance of clinical data on PAH to inform decisions on patient management and policy makers. However, the data on HRQoL in these populations are largely unknown; as a result, the purpose of this study is to investigate the characteristics of HRQoL in these groups of patients and subsequently to determine the potential role of 6MWD and WHO-FC in the occurrence of HRQoL impairment. In addition, the effects of depression and anxiety on perceived HRQoL will also be studied. These findings will provide clues to policymakers and researchers to help better manage HRQoL of PAHs in resource-constrained and high-altitude areas.
Methods
Study design
This was a cross-sectional, observational study conducted between March 2020 and April 2022. Patients diagnosed with PAH were recruited from a tertiary hospital located in Lanzhou, the capital city of Gansu province. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement. 22
Study subjects
Inpatients diagnosed with PAH were selected from the chosen hospital. Eligible participants were those aged above 18 years who had undergone clinical treatments with PAH-specific oral compounds or intravenous/subcutaneous prostacyclin analogs and had residency in Gansu province. Subjects were excluded if they presented with severe arrhythmia, acute right heart failure, history of exercise syncope, or any condition that would hinder their ability to complete the study measurements or questionnaires, such as non-ambulatory or visual/hearing impaired.
Study methods
Two trained researchers performed the assessment. The patient’s demographic information (age, gender, marital status, home location, and educational level), lifestyle factors (alcohol drinking and smoking), and clinical-relevant data (WHO-FC, 6MWD) were obtained from electronic medical records. For analysis, smoking and drinking were categorized as non-smokers (never-smokers or ex-smokers) or non-drinkers (never-drinkers or ex-drinkers), and current smokers (at least within the past month) or current drinkers (at least once per week within the past month). Educational level was self-reported and divided into three groups: Junior high school or below, high school, and college/university. Home location was divided into two levels: rural and urban. Then, each participant was interviewed face-by-face at the bedside using a structured questionnaire designed to elicit data on HRQoL and symptoms of anxiety and depression. If the respondent was unable to answer or could not answer correctly for some reason (such as illiteracy), the family carers were invited to fill in the questionnaire. The survey took up to 30 min for each patient. Each time, after completing the questionnaire, one researcher collected it and placed it in a sealed bag for safekeeping. After all patients completed the questionnaire, the other two researchers entered the data into Excel 2016.
Assessment
HRQoL was determined using the Chinese version of the Short Form 36 questionnaire (SF-36), which comprised a physical component score (PCS) and a mental component summary (MCS) score. 23 Following eight domains: physical functioning (PF), role limitations due to physical problems (RP), body pain (BP), general health (GH), vitality (VT), social functioning (SF), role limitations due to emotional problems (RE), and MH. The PCS comprised PF, RP, BP, and GH scores, while the MCS comprised VT, SF, RE, and MH scores. Item scores were coded, summed, and transformed along a scale from 0 (worst possible health) to 100 (best possible health) for each domain, with higher scores indicating greater satisfaction with QoL. The questionnaire was administered orally to all of the patients by the same therapist.
Most of the detailed data on symptoms of anxiety and depression was published previously by our team. 24 The Self-Rating Anxiety Scale (SAS), which is composed of 20 easily understood questions, was used to assess the frequency of anxiety-related symptoms. 25 For evaluation, the total score (rough score) was obtained by adding the scores of the 20 items. Subsequently, the standard score is obtained through conversion. That is, the crude score is multiplied by 1.25, and then the integer part is taken. The higher the standard score, the more serious the anxiety symptoms. The self-rating depression scale consists of 20 items, and the scoring method is similar to that of SAS. 26 There were 10 positively worded questions and 10 negatively worded questions. Total scores range from 20 to 80. 26
The sample size was computed by following statistical formula with Zα/2 = 1.96, allowable error δ = 2.

Where ‘n’ is the estimated sample size, and ‘σ’ is the standard deviation (SD) of PAH patients’ quality of life score. According to the analysis of pre-survey results, σ = 11.72. Plug the above data into the calculation formula, n=132. To compensate for questionnaires that were discarded due to insufficient information and filling errors, the sample size was increased by 10–20%, with a required sample size of 145–158. In the end, the sample size collected was 152.
Statistical analysis
Statistical analyses were undertaken using the SPSS 21.0 software (IBM Corp, Armonk, NY, USA). First, variables were summarized using descriptive statistics, namely absolute (n) and relative (%) frequencies for categorical variables and mean
Results
Demographic, WHO-FC, and 6MWD
In total, 152 of the patients completed the questionnaire. The median age of the participants was 54.78 ± 14.20 years; 54.6% were female, and 84 (55.3%) were from rural, 44 (29%) had an educational level of high school or above. The mean 6MWD was 353.43 ± 58.65 (205–476) m among the participants. Over 55% of the queues belong to WHO-FC III/IV (Table 1).
Univariate analysis of general characteristics and PCS/MCS in SF-36 (N = 152).

Pearson correlation coefficient.
Equal to t value.
Equal to F value.
MAP, mean arterial pressure; MCS, Mental Component Total Score; 6MWD, 6-min walk distance; PCS, Physical Component Total Score; SD, standard deviation; WHO-FC, World Health Organization-functional class.
p < 0.05, **p < 0.01.
HRQoL domains and summary scores
The average PCS and MCS scores in SF-36 were 43.73 ± 19.58 and 55.32 ± 18.92, respectively (Table 1). As shown in Figure 1, HRQoL differed significantly from Chinese normative values in all eight domains (p < 0.05), among which RP (21.55 ± 9.87) was less than one-third of the Chinese norms (88.79 ± 28.49).

Mean scores of SF-36 for PAH patients versus Chinese population norms.
Univariate analysis of the relationship between WHO-FC, 6MWD, and PCS/MCS
The univariate analysis of the relationship between WHO-FC, 6MWD, and PCS/MCS scores is presented in Table 1. WHO-FC and 6MWD were significantly correlated with PCS, and MCS showed significant correlations with gender, smoking, drinking, WHO-FC, and 6MWD (all p < 0.05).
As shown in Figure 2, PCS and MCS scores exhibited a consistent decline with increasing anxiety and depression scores, and there was a strong negative correlation between anxiety scores and PCS (r = −0.439, p < 0.001), as well as MCS (r = −0.425, p < 0.001).
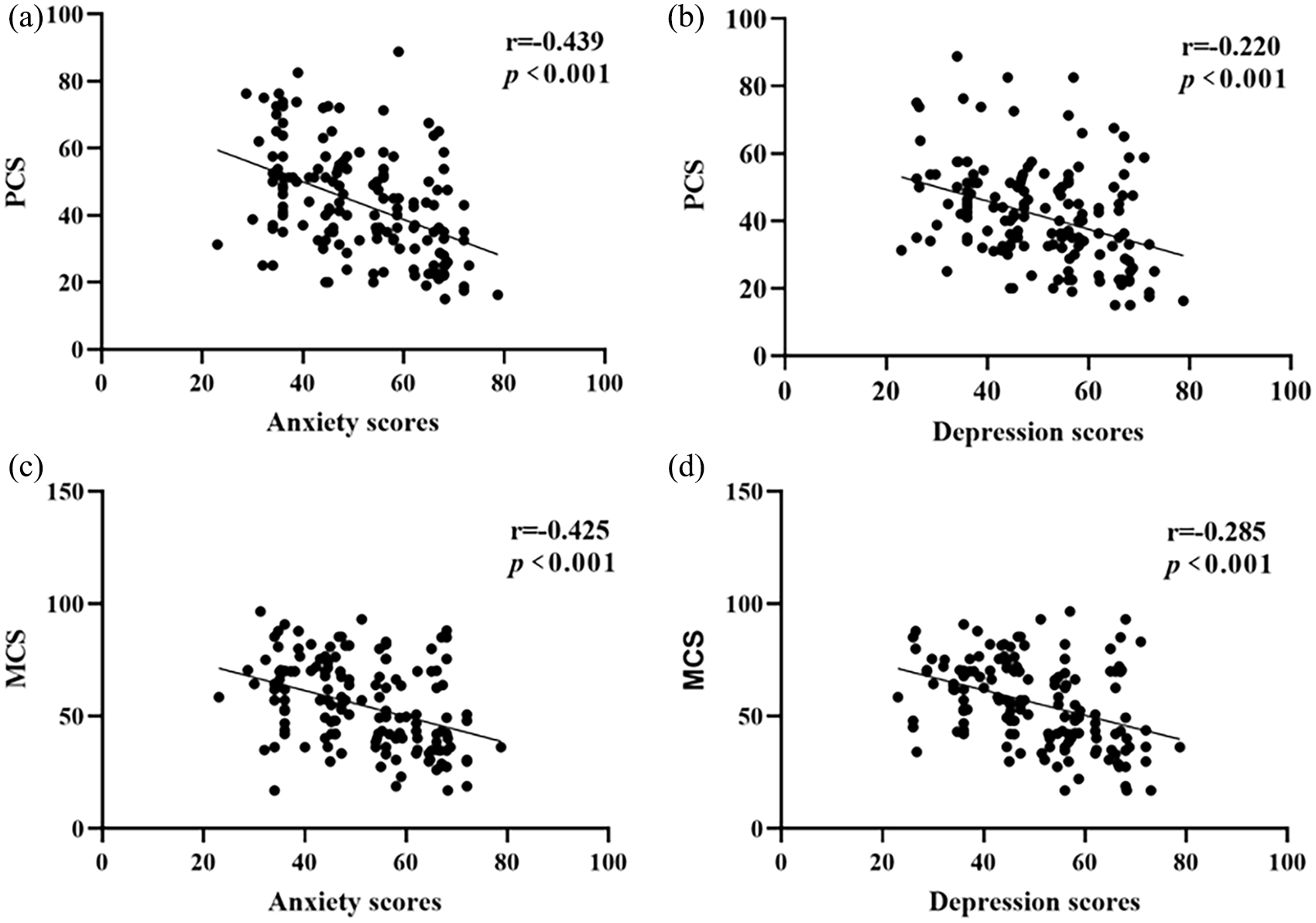
Associations between the anxiety and depression scores and PCS (a, b) and MCS (c, d).
Multiple linear regression analysis of the relationship between WHO-FC, 6MWD, and the PCS/MCS
To exclude the interference of confounding factors, we included statistically significant factors in the univariate analysis results in the multiple linear regression model. The results showed that the most crucial factor influencing PCS was WHO-FC (β = −0.22, p = 0.001), and for every 1-point increase in anxiety scores, PCS decreased by 0.33 points, followed by WHO-FC (β = −0.16, p = 0.014) and 6MWD (β = 0.15, p = 0.036) (Table 2). The factor with the most significant impact on MCS was anxiety scores (β = −0.30, p < 0.001), and PCS decreased by 6.04 points for each grade increase in cardiac function, followed by anxiety scores (β = −0.23, p = 0.001) and depression scores (β = −0.16, p = 0.013) (Table 3). Other parameters associated with the summarized scores of HRQoL were gender and home location for PCS gender for MCS (all p < 0.05).
Multiple linear regression analysis of PCS and general characteristics, anxiety, and depression scores.

95% CI, 95% confidence interval for B; MAP, mean arterial pressure; 6MWD, 6-min walk distance; SE, standard error; WHO-FC, World Health Organization-functional class.
p < 0.05, **p < 0.01.
Multiple linear regression analysis of MCS and general characteristics, anxiety, and depression scores.

95% CI, 95% confidence interval for B; MCS, Mental Component total Score; 6MWD, 6-min walk distance; SE, standard error; WHO-FC, World Health Organization-functional class.
p < 0.05, **p < 0.01.
Discussion
Although being a PAH population living in a resource-limited and as well as high-altitude area, we have found higher mean PCS and MCS scores than that reported in a systematic review. 13 Our study challenges the notion that altitude and development level significantly impact HRQoL in PAH patients. Previous observation reported a negative relationship between altitude and QoL among older adults, 17 also there is study that found no association between PCS and high altitude. 28 Since contrary results and no previous findings have elucidated the difference in PAH patients in different altitudes areas, further studies are warranted to explore the effectiveness of different altitudes on HRQoL with PAH. Despite the differences, a significant decrease in HRQoL in our sample was observed when compared with the Chinese norms. In addition, contrary to other studies, those from rural areas tended to have higher PCS in SF-36 compared to those from urban areas.5,29 Indeed, while providing benefits like healthcare access, urban living may also lead to stress due to a lack of green spaces and intense social interactions. In addition, a lack of social connections between individuals of a given geographic area in urban may significantly affect their HRQoL. Our study found that higher WHO-FC, shorter 6MWD, and elevated anxiety and depression scores, all indicative of higher risk, were associated with significant PCS and MCS impairment.
Similar to other studies,30–32 our study found that 6MWD was significantly reduced in PAH patients. As indicated in previous studies, 30 this condition was expected to impact HRQoL. Furthermore, in our study, the degree to which 6MWD predicted MCS in the linear regression model was not obvious, indicating that patients’ exercise capacity was more related to PCS than to MCS, which may also be related to the fact that more than 60% of the patients in our study were WHO-FC III/IV. The WHO-FC severity and an overall decrease in 6MWD (mean distance 353.43 ± 58.65 m) may further induce the risk of death and hospitalization. 33 Previous surveys by our team found a significant delay in PAH diagnosis in Gansu, which was also reported in others.24,34,35 The delayed diagnosis may be a significant challenge in the future, especially where resources are limited. In addition, high altitude may also affect 6MWD and WHO-FC in PAH patients. Previous studies have shown that higher pulmonary artery pressure and impaired ventricular function limit exercise capacity in patients chronically exposed to high altitudes.36,37 Studies also found that exposure to moderate altitudes can lead to hypoxemia and reduced exercise capacity. 36 Meanwhile, daily activities in patients at higher altitudes may require relatively higher work rates, resulting in significantly impaired functional capacity. 38
In the context of improved vital and clinical outcomes, enhancing HRQoL will be a primary treatment goal. Thus, these factors must be monitored and assessed within PAH patients, especially when WHO-FC is increasing, to establish better strategies for evaluating patient outcomes. A previous study showed that low altitude positively affects areas of physical and functional status, and those living at lower altitudes reported better overall well-being. 17 In addition, PCS in SF-36 is a significant predictor of follow-up outcomes among PAH. 31 However, a study in Latin America reported that less than 50% of the institutions evaluate QoL in PAH as usual, 39 we suggest HRQoL evaluation deserves more attention in routine care visits, especially in the PCS-related domains. In addition, non-pharmacological strategies such as exercise training and palliative care have remarkably improved 6MWD and the QoL in PAH patients.40–44 Therefore, clinicians should make reasonable rehabilitation programs for PAH patients according to their WHO-FC and 6MWD to improve their HRQoL.
PAH patients are more likely to have anxiety and depression emotions. 45 Patients with anxiety have significantly lower 6MWD, which seriously affects their HRQoL. 45 Our study showed that SF-36 HRQoL scores, including PCS and MCS, were all negatively correlated with anxiety scores. Meanwhile, anxiety scores also showed the most significant on PCS in our study; therefore, enhancing anxiety management could potentially contribute to improved HRQoL among PAH patients. In addition, unlike the results of other studies46,47 that reported an association between depression score and PCS/MCS, we found that depression score was only correlated to MCS in multiple linear regression. Several other investigators have also reported this relationship.48,49 The strength of this relationship is very significant and suggests the possibility that MCS could be significantly improved if it was possible to improve depression. In our previous survey, 24 we found no additional treatment beyond anxiety and depression for PAH in Gansu province, which may suggest that these symptoms were either inadequately recognized or else they were felt to be a natural consequence of the disease. Similar to our findings, several previous studies have emphasized the lack of recognition and treatment of depressive symptoms.48,50 It is important to note that any adverse psychological symptoms can interfere with the management of the disease and affect health outcomes.51,52 Meanwhile, European Society of Cardiology/European Respiratory Society guidelines recommend psychological support for all patients with PAH. 53 This highlights the need for those caring for patients with PAH to screen for depression and anxiety, familiarize themselves with the diagnosis and management of depression and anxiety, and consider referral to MH professionals.
Limitations
There are several limitations to this study. First, as the PAH clinic in Gansu province has been established briefly and PAH is a rare disease, the sample is small, resulting in low statistical power and limited ability to analyze and measure the correlation between clinical parameters and SF-36 in multivariate analysis. In addition, there was no subgroup analysis of the differences in altitude level so that patients may differ in clinical symptoms, psychological problems, and HRQoL with varying altitudes. Finally, we use a generic, rather than PAH-specific, quality of life scale. However, despite these limitations, this study provided clinical data on HRQoL in patients with PAH in this high-altitude and underdeveloped area.
Conclusion
We used the SF-36 to assess the HRQoL and its association with WHO-FC, 6MWT, and MH among PAH patients in a underdeveloped and high-altitude area. The study showed that HRQoL was substantially reduced in these populations compared to healthy ones. Significantly PCS was markedly decreased, and the RF score was less than a third of the general Chinese population. WHO-FC, 6MWT, and anxiety scores were independently associated with summarized PCS, whereas those with lower WHO-FC, higher anxiety, and depression scores had lower summarized scores of MCS for HRQoL. Clinicians should develop tailored rehabilitation programs based on WHO-FC and symptom severity to enhance HRQoL in PAH patients.
Supplemental Material
sj-docx-1-tar-10.1177_17534666241246428 – Supplemental material for Impression life with pulmonary hypertension: clinically relevant characteristics and quality of life among patients in Gansu, China
Supplemental material, sj-docx-1-tar-10.1177_17534666241246428 for Impression life with pulmonary hypertension: clinically relevant characteristics and quality of life among patients in Gansu, China by Juxia Zhang, Yujie Wen, Yuhuan Yin, Yiyin Zhang, Rong Zhang, Xiaoli Zhang, Jianying Ye, Yuping Feng and Hongyan Meng in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-2-tar-10.1177_17534666241246428 – Supplemental material for Impression life with pulmonary hypertension: clinically relevant characteristics and quality of life among patients in Gansu, China
Supplemental material, sj-docx-2-tar-10.1177_17534666241246428 for Impression life with pulmonary hypertension: clinically relevant characteristics and quality of life among patients in Gansu, China by Juxia Zhang, Yujie Wen, Yuhuan Yin, Yiyin Zhang, Rong Zhang, Xiaoli Zhang, Jianying Ye, Yuping Feng and Hongyan Meng in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-3-tar-10.1177_17534666241246428 – Supplemental material for Impression life with pulmonary hypertension: clinically relevant characteristics and quality of life among patients in Gansu, China
Supplemental material, sj-docx-3-tar-10.1177_17534666241246428 for Impression life with pulmonary hypertension: clinically relevant characteristics and quality of life among patients in Gansu, China by Juxia Zhang, Yujie Wen, Yuhuan Yin, Yiyin Zhang, Rong Zhang, Xiaoli Zhang, Jianying Ye, Yuping Feng and Hongyan Meng in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-docx-5-tar-10.1177_17534666241246428 – Supplemental material for Impression life with pulmonary hypertension: clinically relevant characteristics and quality of life among patients in Gansu, China
Supplemental material, sj-docx-5-tar-10.1177_17534666241246428 for Impression life with pulmonary hypertension: clinically relevant characteristics and quality of life among patients in Gansu, China by Juxia Zhang, Yujie Wen, Yuhuan Yin, Yiyin Zhang, Rong Zhang, Xiaoli Zhang, Jianying Ye, Yuping Feng and Hongyan Meng in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-4-tar-10.1177_17534666241246428 – Supplemental material for Impression life with pulmonary hypertension: clinically relevant characteristics and quality of life among patients in Gansu, China
Supplemental material, sj-pdf-4-tar-10.1177_17534666241246428 for Impression life with pulmonary hypertension: clinically relevant characteristics and quality of life among patients in Gansu, China by Juxia Zhang, Yujie Wen, Yuhuan Yin, Yiyin Zhang, Rong Zhang, Xiaoli Zhang, Jianying Ye, Yuping Feng and Hongyan Meng in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.