
Abstract
Background:
Empiric therapy with multichannel intraluminal impedance-pH monitoring (MII-pH) has been used for the initial treatment of gastroesophageal reflux-induced chronic cough (GERC). However, an algorithm based on the gastroesophageal reflux disease questionnaire (GerdQ) has the potential to achieve a simple, structured, and effective treatment approach for patients with GERC.
Objectives:
This study compared the efficacy of anti-reflux therapy based on GerdQ (new structured pathway, NSP) with medical treatment after MII-pH examination (ordinary clinical pathway, OCP) in the management of GERC.
Design:
For the NSP, we adapted the GerdQ score to establish the basis for a treatment algorithm. For the OCP, treatment was determined using the MII-pH examination results.
Methods:
The non-inferiority (NI) hypothesis was used to evaluate NSP versus OCP.
Results:
Overall, the NSP and OCP-based therapeutic algorithms have similar efficacy for GERC [NI analysis: 95% confidence interval (CI), −4.97 to 17.73, p = 0.009; superiority analysis: p = 0.420]. Moreover, the cough symptom scores and cough threshold improved faster in the NSP group than in the OCP group at week 8 (p < 0.05). In the subgroup analyses using the GerdQ and GerdQ impact scale (GIS) scores, patients with low-likelihood GERC (GerdQ < 8) were more likely to benefit from OCP (NI analysis: 95% CI, −19.73 to 18.02, p = 0.213). On the other hand, in patients with high-likelihood and low-reflux impact GERC patients (GerdQ > 8 and GIS < 4), the NSP arm was not inferior to the standard treatment of OCP (NI analysis: 95% CI, −8.85 to 28.21%, p = 0.04; superiority analysis: p = 0.339), indicating that GerdQ- and GIS-guided diagnosis and management of patients with GERC could be an alternative to MII-pH management, especially in settings with reduced medical resources.
Conclusions:
The use of the GerdQ algorithm should be considered when handling patients with GERC in the primary care setting.
Trial registration:
This research was registered in the Chinese Clinical Trials Registry (ChiCTR-ODT-12001899).
Introduction
Gastroesophageal reflux cough (GERC), also known as reflux cough syndrome, is a special form of gastroesophageal reflux disease (GERD) predominantly characterized by coughing symptoms. 1 There is evidence that GERC is responsible for 10–40% of chronic cough cases in Western countries and 6–29% of cases in China.2–4 Because of the extraoesophageal reflux-related symptoms and the lack of unified diagnostic criteria, most patients with GERC are unable to obtain proper diagnosis and treatment. Instead, patients with GERC undergo a series of auxiliary examinations and therapeutic drug regimens for an extended period, seriously affecting the patients’ quality of life and leading to a substantial socioeconomic burden.
In patients with suspected GERC, with or without gastrointestinal manifestations (heartburn and regurgitation), empirical anti-reflux therapy has been reported to relieve the cough in most patients. Empiric therapy typically consists of varying doses of proton pump inhibitors (PPIs), ranging from a standard dose of PPIs to a double dose of PPIs. However, the therapeutic effects of this treatment regimen are controversial, as some guideline experts maintain a negative consensus on the limited effectiveness of anti-acid treatment in patients without peptic symptoms. Moreover, a number of meta-analyses of randomized clinical trials have yielded inconsistent or contradictory results.5–7 It is important to note that only some patients with GERC, particularly those with objective evidence of reflux symptoms, benefit from anti-acid therapy. The therapeutic gain after proper PPI therapy is greater in patients with GERC and pathologic oesophageal acid exposure or concomitant oesophageal reflux-associated symptoms than in those without. 6 Moreover, severe oesophageal acid exposure may require a higher dose of PPI to effectively control gastric acid secretion. The residual acid reflux continually elicits cough by microaspiration or through the oesophageal–tracheobronchial reflex, as reported in patients with refractory GERC treated with PPIs twice daily.8,9 Notably, the inconsistency between reflux-associated symptoms and oesophageal acid exposure could represent the PPI response. Misinterpretation of the evaluation of symptom burden in physician interviews can often lead to unsatisfactory acid-suppressive therapy. Thus, it is important to ensure accurate diagnosis and identify patients likely to be responsive to PPIs.
Ambulatory multichannel intraluminal impedance-pH monitoring (MII-pH) is a novel method for diagnosing and treating patients with GERC 7 by providing information about the oesophageal acid exposure time (AET), reflux episodes, and other reflux parameters. The Lyon Consensus proposed MII-pH examination as the gold standard for the diagnosis of GERD. 10 Based on the comparison of reflux parameters, the MII-pH examination guides the anti-reflux treatment of GERC and improves the treatment success rate to some extent. Research has revealed that the PPI response to GERC may be predicted by the AET, reflux episodes, or other baseline impedance values in patients with chronic cough. 8 However, some obvious limitations, such as requirement for technical equipment, invasive examinations, and low patient acceptance, hinder its widespread use.
Therefore, it is important to implement a symptom-based management algorithm, to optimize the management of patients, preferably assisted by patient questionnaires. The gastroesophageal reflux disease questionnaire (GerdQ) is a self-report questionnaire that contains two reflux symptom-related positive questions, two gastrointestinal symptom-related negative questions, and two reflux symptom impact-related positive questions. 11 In our previous study, GerdQ demonstrated a high diagnostic value for predicting GERC at a cutoff point of 8.0, with a sensitivity of 66.7% and a specificity of 91.7%, compared with MII-pH. 12 Moreover, the GerdQ impact scale (GIS) has a score range of 0–6 and contains two reflux symptom impact-related positive and negative questions. GIS focuses on the reflux symptom impact, which is a useful aid in the anti-reflux treatment of GERD patients. 13 In this study, we assessed the use of GerdQ and GIS in an algorithm for diagnosing and selecting anti-reflux treatment for patients with GERC as an alternative to routinely performing MII-pH before initiating therapy.
Materials and methods
Patient selection
This is a prospective, parallel-group, randomized clinical trial that was conducted over a 3-year period in one treatment center. All patients suspected of having GERC who were referred to the Department of Pulmonary and Critical Care Medicine, Tongji Hospital of Tongji University, between October 2018 and September 2021, were recruited for this study. Each patient completed a series of examinations, such as chest radiography, chest computed tomography (CT), lung function tests, histamine bronchial provocation test, and sputum cytology, to identify other common causes of chronic cough, following a step-by-step protocol. 4
The inclusion criteria for patients with GERC are as follows: (1) aged 16–80 years; (2) with cough symptoms persisting for >8 weeks, with or without concomitant gastrointestinal symptoms; (3) can undergo cough severity test, cough sensitivity test, GerdQ examination, and MII-pH examination; and (4) positive for acid reflux through AET ⩾6.0 or an acid reflux symptom association probability (SAP) ⩾95% or an acid reflux symptom index (SI) ⩾50%; or positive with nonacid reflux through nonacid reflux SAP ⩾95% or nonacid SI ⩾50% during MII-pH test.
The exclusion criteria are as follows: (1) pregnant and lactating women; (2) smokers or previous smokers within the last 2 years; (3) patients with reading and writing disabilities; (4) patients with other definitive chronic cough causes; (5) patients with chronic cough but with improved symptoms after receiving treatment for other concomitant causes; (6) patients with rales and obvious abnormalities on lung physical examination, chest radiography, or chest CT; and (7) inability to tolerate MII-pH examination. Notably, patients who failed to attend scheduled visits or whose information was incomplete were excluded.
The study will be reported according to the STARD (Standards for Reporting Diagnostic accuracy studies) 2015 statement. 14
Laboratory investigations
Cough symptom severity score
At the first visit and every 4 weeks during the follow-up period, we performed a cough severity test based on the study of Hsu et al., 15 which uses a six-point scale from 0 to 5 (0 means no cough and 5 means the worst cough).
Cough sensitivity test
According to the method described by Fujimura et al., 16 cough sensitivity to capsaicin was evaluated in all suspected patients with GERC. Cough thresholds C2 and C5 were defined as the lowest concentrations of capsaicin required for the induction of two or more coughs and five or more coughs, respectively, upon exposure to capsaicin.
Lung function test
Lung function and bronchial provocation tests were performed as described in the guidelines of the American Thoracic Society 17 and Respiratory Society of the Chinese Medical Association. 18
Induced sputum cytology
Cytological examination of induced sputum was conducted following a previous protocol. 4
MII-pH examination
The MII-pH examination was performed as previously described. The MII-pH catheter was inserted into the esophagus with six impedance channel amplifiers (3, 5, 7, 9, 15, and 17 cm above the lower esophageal sphincter) and an antimony pH probe (5 cm above the lower esophageal sphincter). All seven channels serving as the event markers were recorded over 24 h using a portable data logger. AET (%) was defined as the total time when the pH was below 4 divided by the total time monitored. The Lyon Consensus proposes that AET <4% definitively rules out pathologic gastroesophageal acid reflux and that >6% is considered definitively abnormal, with intermediate values between these limits being inconclusive. 10 The DeMeester score was analyzed using database software with a global measure of esophageal acid exposure. The temporal association between detected reflux and cough recorded on the patients’ diary cards was assessed using the SAP. The SI is the ratio of the number of symptoms preceded by reflux episodes to the total number of symptoms within 2 min of the reflux event.
GerdQ evaluation
There are six symptom domains assessed by the GerdQ, including the GIS, gastrointestinal symptom rating scale, and reflux disease questionnaire (RDQ). 19 The GerdQ evaluation scale has a range of 0–18 points based on the patients’ recall of their symptoms in the past week. Based on the GerdQ score (0–18) and GIS score (0–6), patients with suspected GERC were divided into three different groups: low likelihood of GERC (LL GERC, GerdQ < 8), high likelihood of GERC and low reflux impact (HLLI GERC, GerdQ > 8 and GIS < 4), and high likelihood of GERC and high reflux impact (HLHI GERC, GerdQ > 8 and GIS > 4). All patients were blinded to their GerdQ scores throughout treatment.
Research procedure
Eligible patients with symptoms suggestive of GERC were consecutively allocated randomization codes using an electronic case report form. Randomization was performed in blocks of four into two distinct pathways: (1) the new structured pathway (NSP), in which patients are diagnosed using the MII-pH examination and sequential stepwise anti-reflux therapy, and are treated based on the GerdQ score and (2) the ordinary clinical pathway (OCP), in which patients undergo the MII-pH examination to guide the treatment. The allocation was concealed until all patients entered the trial. In the NSP group, the investigators were blinded to the MII-pH examination results throughout the treatment. In the OCP group, the investigators were blinded to the GerdQ and GIS scores during treatment. All patients were blinded to the GerdQ scores and MII-pH examination results throughout treatment. To identify the primary and secondary endpoints, data were examined by two independent assessors and disagreements were resolved by a third assessor. The clinical trial coordinator oversaw and instructed the investigators while reviewing the accuracy of the data and the compliance to randomization.
Before therapy, initial patient assessments in the OCP and NSP groups included cough symptom score, cough sensitivity evaluation, lung function test, induced sputum cytology, GerdQ assessment, and MII-pH examination. Each follow-up visit at 4 weeks included assessments of the cough symptom score, cough sensitivity test, MII-pH examination, and GerdQ. The treatment regimens were changed or maintained based on the above results. The study was terminated after 4 weeks for those with cough resolution and was extended for another 4 weeks for those without cough resolution (Figure 1).

Patient flow chart.
New structured pathway
Patients with suspected GERC who were randomized into the NSP group were categorized into three different subgroups according to their GerdQ and GIS scores, each with their corresponding initial treatments. MII-pH examination was performed to confirm the diagnosis of GERC, and the investigators and patients were blinded to the MII-pH results during the entire treatment period.
(1) LL GERC: Patients with LL GERC are recommended initial therapy with a standard dose of PPI (omeprazole, 20 mg, twice daily) and prokinetic (osapride 10 mg thrice daily) for 8 weeks. Patients who responded to generic PPI continued treatment until their cough was relieved. In the fourth week, baclofen (20 mg, three times daily) was administered if the cough has not resolved.
(2) HLLI GERC: Patients with HLLI GERC also started initial treatment with a standard dose of PPI (omeprazole, 20 mg, twice daily) and prokinetic (osapride 10 mg thrice daily) for 4 weeks. In the next 4 weeks, incremental high-dose PPI therapy was administered to patients who failed to respond to standard anti-reflux therapy. In the remaining nonresponders, baclofen (20 mg, three times daily) and omeprazole (40 mg, two times daily) were administered daily as the third step in the protocol.
(3) HLHI GERC: Patients with HLHI GERC received a double-dose PPI (omeprazole, 40 mg, twice daily) and prokinetic (osapride 10 mg thrice daily) for 8 weeks. Baclofen (20 mg, three times daily) was added to the treatment regimen for patients who failed to respond to double-dose PPI therapy after 8 weeks.
Ordinary clinical pathway
Patients with suspected GERC who were randomized into the OCP group underwent evaluation of cough symptom score, cough sensitivity, GerdQ, GIS, and MII-pH at the initial visit and for each subsequent visit. Notably, the GerdQ and GIS scores were blinded to the investigators and patients during the treatments.
According to the MII-pH evaluation and cough resolution at each clinical assessment, a corresponding therapeutic regimen, varying from a standard-dose PPI to a double-dose PPI, is provided for patients with suspected GERC. Sequential stepwise anti-reflux therapy with baclofen was provided to the remaining nonresponders.
Outcome measure and follow-up
Overall cough resolution was interpreted as the primary endpoint. 20 GERC is considered controlled and improved when the cough disappears or when the daytime and nighttime cough symptom scores decrease by two or more. On the other hand, failure of treatment was defined as a worsening of cough or lack of a recognizable weakening of cough. The cough resolution rate after each step of treatment, along with changes in cough symptom score, reflux symptom score, and cough sensitivity to capsaicin, were used as secondary endpoints.
All patients were confirmed to have GERC at the end of treatment if the following criteria were met: (1) cough symptoms lasting >8 weeks; (2) abnormal acid reflux: AET ⩾6.0 or acid reflux SAP ⩾95% or acid SI ⩾50%; or abnormal nonacid reflux: nonacid reflux SAP >95% or nonacid SI >50%; and (3) cough resolution or improvement with a stepwise anti-reflux therapy.
Following the stepwise protocol, patients underwent two follow-up visits every 4 weeks to the respiratory clinic, where changes in cough symptom scores, reflux symptom scores, and cough sensitivity to capsaicin were monitored. A follow-up period of at least 12 weeks was required if the treatment was ineffective.
Statistical analyses
We assumed the PPI overall response to be 75% in both the NSP and OCP groups by referring to a previous study 21 and the non-inferiority (NI) difference (for NSP relative to OCP) was set at 10%. Based on the response rate and NI difference, we calculated a requirement of 96 patients for each group, with a statistical power of 80%. In addition, we included a 10% dropout rate in the sample estimation.
NI analysis was used to measure the difference in treatment efficacy between the NSP and OCP pathways within a 10% margin of clinical indifference. Clinical indifference was based on symptomatic response rates to PPIs reported in previous studies. A test-based two-sided 95% confidence interval (CI) was calculated and the NI of treatment responders between the NSP and OCP pathways was declared when the CI was within the NI limit of 10%. The NSP would be judged to be superior to the OCP if the 95% CI was greater than 0. For conducting equivalence and NI studies, SAS 9.4 (SAS Institute, Cary, NC, USA) and PASS 15.0 (NCSS, LLC, Kaysville, UT, USA) was used for testing hypotheses, assessing statistical power, and determining sample size.
Normally distributed data are presented as mean ± standard deviation (SD), and skewed data as median (25–75% interquartile range). In addition, C2 and C5 were logarithmically transformed and represented as geometric SD. In addition, we performed the analysis of primary variables using the t test, Mann–Whitney U test, Chi-square test, and Fischer’s exact test using SPSS 22.0 (IBM Corp., Armonk, NY, USA), and the p values of the two sides were <0.05.
Results
General clinical information
A total of 309 patients with suspected GERC and abnormal acid or nonacid reflux between October 2018 and September 2021 met the inclusion criteria for this study. GERC was confirmed by a sequential stepwise anti-reflux therapy in 189 patients. Among the patients with GERC, 124 responded to PPI therapy with a standard or double dose of PPIs, while 65 had symptoms controlled by baclofen therapy. Of the other patients with suspected GERC, 42 quit the study, 46 were lost to follow-up, and 32 failed to respond to the sequential stepwise anti-reflux therapy. Among the 32 nonresponders, the cause of the cough was attributed to cough variant asthma (19), upper airway cough syndrome (9), eosinophilic bronchitis (2), or psychogenic factors (2). The patient flowchart is shown in Figure 2.

The construct of NSP and OCP algorithms.
Of the remaining 189 patients with GERC, 96 were randomized into the NSP pathway and 93 were randomized into the OCP pathway. Demographic data and baseline characteristics such as body mass index (BMI), duration of cough, cough symptom score and C2/C5 ratio are shown in Table 1. Based on the GerdQ and GIS scores, 38.54% of all patients had a low likelihood of GERC, 32.29% had a high likelihood and low impact of GERC and 29.16% had a high likelihood and high impact of GERC in the NSP group. Notably, the distribution was similar in the OCP group.
Demographic characteristic of 189 patients with GERC.

C2, the lowest concentration of capsaicin required for the induction ⩾2 coughs; C5, the lowest concentration of capsaicin required for the induction ⩾5 coughs; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; GERC, gastroesophageal reflux-induced chronic cough; GerdQ, gastroesophageal reflux disease questionnaire; HLHI, high-likelihood GERC and high symptom impact (GerdQ total score 8–18 and GerdQ impact score 4–6); HLLI, high likelihood of GERC and low symptom impact (GerdQ total score 8–18 and GerdQ impact score 0–3); LL, low likelihood of GERC (GerdQ total score 0–7); NSP, new structured pathway; OCP, ordinary clinical pathway.
GerdQ and the findings of MII-pH
All variables, including MII-pH-related parameters, were balanced between the two pathways, as demonstrated by Chi-square statistics and Fischer’s exact test (Table 2).
The comparison of MII-pH examination-related parameters.

NSP, new structured pathway; OCP, ordinary clinical pathway; SAP, symptom association probability.
The changing patterns of cough symptom scores over the treatment period were similar between the two groups [Figure 3(a)]. However, the cough symptom scores (including daytime and nighttime cough scores) improved faster in the NSP group than in the OCP group at week 8 (p < 0.05). The cough thresholds C2 and C5 to capsaicin increased, while the GerdQ score showed a corresponding reduction in both the NSP and OCP groups [Figure 3(b) and (c)], with no significant differences between the two groups (p > 0.05).

Changes in cough symptom score, cough threshold C2 and C5, and the score of GerdQ and MII-PH parameters over the time after treatment algorithms of NSP (n = 96) and OCP (n = 93), respectively. (a) Left: changes in daytime cough symptom score over time; Right: changes in nighttime cough symptom score over time. (b) Left: changes of cough threshold C2 and C5 in NSP group; Right: changes of cough threshold C2 and C5 in OCP group. (c) Left: changes of GerdQ score in NSP group; Right: changes of GerdQ in OCP group. (d) Left: changes of oesophageal acid exposure time in OCP group; Right: changes of reflux episodes in OCP group.
Based on the post-study MII-pH examination for the OCP group, the AET score and reflux episodes over 24 h were significantly decreased when compared to baseline MII-pH characteristics [AET: 5.08 ± 0.77 versus 3.62 ± 0.64, t = 2.407, p = 0.017; reflux episodes over 24 h: 86.00 (95.50) versus 59 (53.10), Z = −3.232, p = 0.001, Figure 3(d)].
Comparison of the PPI response between the NSP and OCP pathways
Overall, cough was controlled by PPI therapy in 124 patients with GERC (65.60%) and resolved with baclofen in 65 patients (33.39%). The overall therapeutic success rate of PPI was 65.60%. A total of 66 patients (68.75%) in the NSP group had symptoms controlled by PPI therapy, whereas 58 patients (62.36%) in the NSP group OCP responded to PPI therapy. The NI analysis demonstrated that the two-sided 95% CI is calculated as −4.97% to 17.73%. Importantly, there is evidence of equivalence between the NSP and OCP groups (p = 0.009, Figure 4). Thus, a superiority analysis was performed to assess the difference in the probability of treatment response and the superiority of the NSP group over the OCP group was not established (p = 0.420).
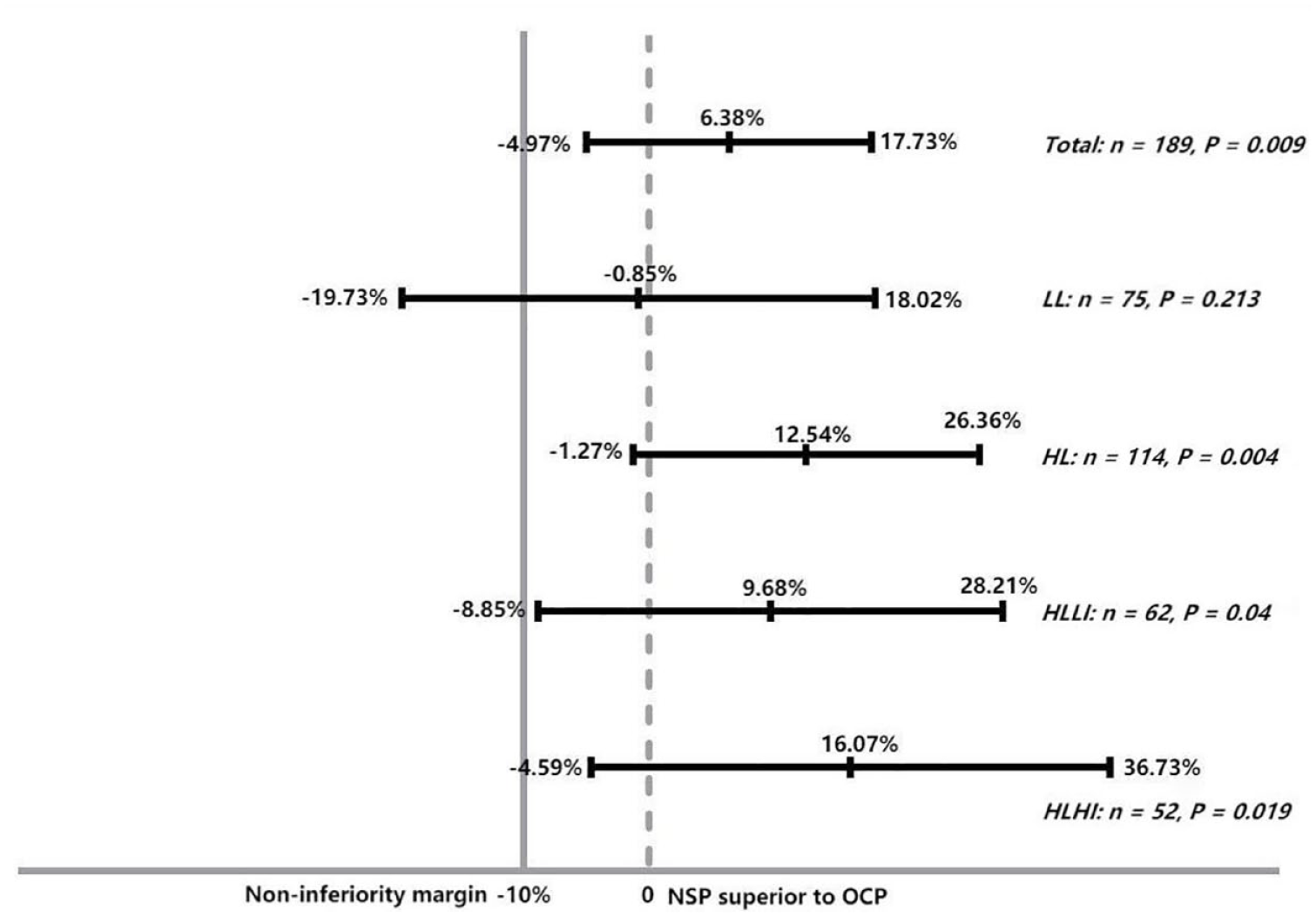
NI analysis of the NSP compared to OCP group.
Subgroup analysis
We also performed subgroup analyses based on GerdQ and GIS scores. In the stratified analyses of GerdQ scores, we concluded that LL GERC patients (GerdQ < 8) were more likely to be responsive to the standard treatment in the OCP arm when compared to the NSP arm (NI analysis, 95% CI: −19.73% to 18.02%, p = 0.213, Figure 4).
In further consideration of the subgroup analyses by GerdQ and GIS scores, we divided the high-likelihood GERC patients into those with low reflux impact (impact score 0–3) and high reflux impact (impact score 4–6). For the HLLI GERC group, the new treatment efficacy of the NSP group was not inferior to the OCP group (NI analysis, 95% CI: −8.85% to 28.21%, p = 0.040; superiority analysis: p = 0.339), indicating that GerdQ and GIS guided the diagnosis and management of patients with GERC. This also supports that the NSP could be an alternative to MII-pH examination in settings with reduced medical resources. A greater numerical difference was observed between the NSP (78.57%) and OCP (62.50%) groups for the HLHI GERC patients, which supports NSP in settings with an increased symptom burden, despite the difference not reaching statistical significance (superiority analysis: p = 0.189).
Discussion
GERC is one of the most common causes of chronic cough. 22 Generally, patients with both GERC and reflux symptoms, such as heartburn and regurgitation, are more likely to respond to PPI treatment. However, an estimated 10–40% of patients with GERC do not benefit from empiric PPI therapy, either partially or completely. 23 A study documented residual acid reflux in patients with GERC and persistent heartburn and cough who were being treated with PPI once or twice a day. 24 It showed that the use of high-dose PPI resulted in an improvement in cough symptoms in 28.1% of the patients. 21 Thus, the therapeutic benefits of appropriate anti-acid therapy in patients could not be ignored. Moreover, evidence suggests that a rigorous PPI therapeutic algorithm in patients with GERC is necessary to facilitate prompt diagnosis, guide the choice of treatment, and identify responsive patient populations.
Our study compared the treatment efficacy between the NSP group, which utilizes a GerdQ-guided treatment approach, and the OCP group, which is the current clinical practice standard utilizing MII-pH. For the NSP group, in response to PPI therapy, the cough symptom score decreased, with a corresponding reduction in the GerdQ score. Similarly, in the OCP group, 50 patients with GERC, as confirmed by the MII-pH-based treatment strategy, had decreased cough symptoms, GerdQ scores, and AET scores when compared to baseline characteristics. In addition, cough symptom scores improved faster in the NSP group than in the OCP group at week 8. Based on the results of the overall primary efficacy, there was an improvement in the symptom response rate for the NSP (68.75%) compared to the OCP (62.36%). Notably, the NI analysis revealed that the two diagnostic procedures were equally effective in resolving cough.
Stratified analyses of patients with high and low likelihoods of GERC indicated that patients with a low likelihood of GERC would benefit from MII-pH examination to determine the correct course of treatment, rather than GerdQ assessment. The GerdQ assessment for regurgitation and heartburn is not sufficient to distinguish acid GERC from nonacid GERC, resulting in a relatively lower frequency of acid GERC in LL patients. Thus, the acid GERC in the LL GERC group would be less likely to be responsive to acid-suppressive therapy when compared to the MII-pH-based approach. Therefore, there were more responders in the LL GERC group patients who underwent the MII-pH examination.
To further examine the GerdQ score, we also assessed the subgroup of patients with HLHI GERC, and the results showed a numerically larger difference in response rate between the NSP and OCP groups, supporting NSP in patients with an increasing symptom burden. We deduced that the reason for this is that patients with a high reflux impact score would benefit from more potent acid inhibition beginning from the initiation of treatment (double PPI). This may provide a longer duration of acid suppression and would overcome cough symptoms, especially those induced by reflux episodes due to late evening meals and sleep.
For patients with HLLI GERC, GerdQ-guided diagnosis and management could be an alternative to MII-pH examination because their treatment efficacy is comparable according to the NI analysis. Our previous study indicated that in predicting acid GERC, GerdQ presented higher sensitivity and GerdQ scores were significantly correlated with DeMeester scores on MII-pH examination in patients with acid GERC. In addition, the therapeutic algorithms for patients with HLLI GERC in the OCP and NSP groups were similar.
GerdQ is a tool designed to evaluate the frequency and intensity of gastrointestinal symptoms to improve and standardize symptom-based diagnosis and treatment response. 13 Our previous research revealed that GerdQ has good performance in diagnosing GERC, with a sensitivity of 66.7% and specificity of 91.7%. 12 Likewise, Grusell et al. 25 argued that the GerdQ score was highly sensitive and specific in predicting PPI response in patients with GERD, with a positive predictive value (PPV) of 99% at a cutoff of 8. The impact of cough and reflux symptoms on sleep and the use of additional nonprescription medication items in the GerdQ were used to judge the severity and consequences of GERC symptoms, providing a separate GIS (0–6). Jones et al. 26 demonstrated that GIS can assist doctors in identifying treatment needs in newly diagnosed patients with GERD, as well as in identifying patients chronic GERD who need more effective treatment. GerdQ can be used to identify patients requiring MII-pH evaluation, especially those with oesophageal reflux symptoms, nonacid reflux, and other differential diagnoses. For the HLHI GERC patients, GerdQ and GIS can identify those in need of an initial augmented acid suppression therapy. Moreover, we postulate that GerdQ may be useful in determining the initial and sequential therapy of patients with HLHI GERC, comparable to MII-pH examination. The GerdQ can also conserve medical resources since treatment selection is based on patient needs and the need for invasive MII-pH examination is reduced.
The study findings enable the primary care physician to use a simple tool for ensuring appropriate initial therapy for patients with GERC. The GerdQ eliminates the long waiting period necessary for the MII-pH approach, which may result in the possible deterioration of patient well-being and a potential loss of productivity during waiting time. A more structured follow-up of patients with GERC based on GerdQ and GIS to evaluate treatment response and select patients should be established. Specifically, for patients with LL GERC (GerdQ < 8), our study suggests that an MII-pH examination may be necessary to clarify the presence of nonacid reflux and the need for neuromodulator therapy. For patients with HLLI GERC (GerdQ > 8 and GIS < 4), stepwise treatment from standard-dose PPI to double-dose PPI anti-reflux is indicated. Finally, for patients with HLHI GERC (GerdQ > 8 and GIS > 4), double-dose PPI anti-reflux therapy was indicated. To conclude, GerdQ prevents physicians from underestimating the symptom burden or overestimating the effectiveness of medical treatment, as previously described. 27
Our study has several strengths and weaknesses. To date, this study is the first to focus on the difference in efficacy between a GerdQ-based algorithm and an MII-pH-based approach for the treatment of GERC. In our study, a symptom-based approach enabled proper primary care, avoided suboptimal treatment, and allowed for fewer MII-pH examinations, shortening the long waiting time for referral. A potential limitation of our study is its short duration and long follow-up interval, which may not have recorded the characteristics of cough in detail. In addition, a post-study MII-pH examination for the NSP group was lacking, as the NSP patients declined a repeat invasive MII-pH test after treatment. In our study, it is likely that some patients with GERC who were resistant to anti-reflux therapy but are responsive to other therapies, such as anti-reflux therapy, might have been underdiagnosed. In addition, the number of GERC cases in the stratified analysis was relatively small, leading to a weaker statistical power. A larger sample size of patients with GERC in different groups is required.
Conclusion
For patients with GERC experiencing a high reflux impact, a symptom-based approach facilitated by the GerdQ is more beneficial in directing appropriate medical treatment and reducing the overuse of medical resources. Furthermore, the algorithm ensured that primary care physicians could utilize a simple tool to perform more accurate diagnosis and therapy for patients with GERC.
Supplemental Material
sj-doc-1-tar-10.1177_17534666231220817 – Supplemental material for A comparison between a gastroesophageal reflux disease questionnaire-based algorithm and multichannel intraluminal impedance-pH monitoring for the treatment of gastroesophageal reflux-induced chronic cough
Supplemental material, sj-doc-1-tar-10.1177_17534666231220817 for A comparison between a gastroesophageal reflux disease questionnaire-based algorithm and multichannel intraluminal impedance-pH monitoring for the treatment of gastroesophageal reflux-induced chronic cough by Wanzhen Li, Tongyangzi Zhang, Wenhua Gu, Wenbo Shi, Shengyuan Wang, Yiqing Zhu, Cuiqin Shi, Li Yu and Xianghuai Xu in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.