
Abstract
During the COVID-19 pandemic, the number of patients with hypoxemic acute respiratory failure (ARF) due to SARS-CoV-2 pneumonia threatened to overwhelm intensive care units. To reduce the need for invasive mechanical ventilation (IMV), clinicians tried noninvasive strategies to manage ARF, including the use of awake prone positioning (PP) with continuous positive airway pressure (CPAP). In this article, we review the patho-physiologic rationale, clinical effectiveness and practical issues of the use of PP during CPAP in non-intubated, spontaneously breathing patients affected by SARS-CoV-2 pneumonia with ARF. Use of PP during CPAP appears to be safe and feasible and may have a lower rate of adverse events compared to IMV. A better response to PP is observed among patients in early phases of acute respiratory distress syndrome. While PP during CPAP may improve oxygenation, the impact on the need for intubation and mortality remains unclear. It is possible to speculate on the role of PP during CPAP in terms of improvement of ventilation mechanics and reduction of strain stress.
Keywords
Introduction
Prone positioning (PP) was first described in 1976 as a procedure to treat patients affected by acute respiratory distress syndrome (ARDS). 1 PP has been widely adopted in patients receiving invasive mechanical ventilation (IMV) for ARDS, with the greatest benefits among those with moderate to severe disease. 2 When combined with lung protective ventilation, protocolized PP of 16 h/day reduces mortality compared to IMV in conventional supine position.3,4 During the COVID-19 pandemic, PP was recommended for patients with severe ARDS receiving IMV, 5 but it was also adopted in patients receiving noninvasive respiratory support, such as noninvasive positive pressure ventilation (NIPPV), continuous positive airway pressure (CPAP) and high flow nasal cannula (HFNC). It was hypothesized that PP in these patients may improve ventilatory physiology as it does in IMV, but during the early phases of the pandemic, there was little evidence to determine the clinical impact of its use.
The evidence for the use of noninvasive respiratory supports in patients with de novo acute respiratory failure (ARF) remains debated.6,7 CPAP has been studied in patients with moderate and severe ARF, and compared to standard oxygen, it improves oxygenation, prevents the evolution of acute lung injury, and reduces the need for endotracheal intubation (ETI).8–10 But noninvasive respiratory supports are not without risk. NIPPV in particular can expose non-intubated patients with spontaneous breathing to high transpulmonary pressure swings and potentially to patient self-inflicted lung injury (P-SILI) 11 and eventual treatment failure. 12 Both CPAP and NIPPV can be delivered using either an oronasal mask, or a helmet interface. By reducing leaks and improving tolerability, the latter interface may allow higher values of positive end-expiratory pressure (PEEP) and longer treatment sessions of NIPPV and CPAP. 13 Additional potential benefits of CPAP over NIPPV in patients with ARF from SARS-CoV-2 pneumonia include its comparative simplicity, resulting in increased feasibility and the possibility of applying it outside of the intensive care unit (ICU).
A recent rapid practice guideline 14 provides a strong recommendation for a trial of PP in adult patients with COVID-19-related hypoxemic ARF who were receiving either NIPPV, CPAP or HFNC. According to the panel of experts, PP appears to reduce the risk of ETI, and although it may not reduce mortality, it should be conducted in an area where patients can be monitored by staff experienced in rapidly detecting and managing clinical deterioration.
In consideration of the peculiarly favourable physiology of CPAP over NIPPV and HFNC, we perform this narrative review with the aim of describing the pathophysiologic effects, the clinical impact and the practical issues of the use of PP during CPAP in non-intubated, spontaneously breathing patients with ARF due to SARS-CoV-2.
Material and methods
As a descriptive review of the effects of CPAP with PP, rather than a comparative review, our structured clinical question was: in adult patients with COVID-19 disease (population), what are the impacts of CPAP with prone positioning (intervention), upon physiologic parameters, adverse events, ETI and death (outcomes)? We searched three electronic databases: PubMed, WHO COVID-19 Research database and LitCovid (up to December 2022) using the keywords COVID-19 AND CPAP AND pronation OR prone position. We included observational studies or randomized controlled trials (RCTs) of patients >18 years of age affected by ARF due to SARS-CoV-2 pneumonia, and treated with CPAP with PP, which reported the outcomes of ETI, death, adverse events and respiratory parameters. Publications in languages other than English were excluded. We extracted data describing the characteristics of the included studies, as well as their results, into tables. As a descriptive rather than comparative review we did not conduct a formal meta-analysis or appraise the quality of evidence. We provide a narrative summary and clinical interpretation of the physiologic results in the text of the review.
The database search resulted in 1090 results, of which 11 were eligible for inclusion in the clinical review. Table 1 describes the characteristics of the included studies.15–25
Observational or RCT studies of patients >18 years affected by acute hypoxemic respiratory failure due to SARS-CoV-2 pneumonia treated with CPAP associated to prone positioning.

CPAP, continuous positive airway pressure; ED, Emergency department; ETI, endotracheal intubation; HFNC, high flow nasal cannula; ICU, Intensive Care Unit; MW, medical ward; NIPPV, noninvasive positive pressure ventilation; P(A-a)O2, Alveolar-arterial PO2 difference; RICU, Respiratory Intermediate Care Unit; RR, respiratory rate; SBP, Systolic Blood Pressure.
Difference supine versus prone position.
Wilcoxon test.
Group P: tolerate prone and side positioning for at least 10 h/d; group nP: patient noncompliant about PP.
Analysis of variance with post hoc correction for multiple testing.
One from the subgroup of fourteen patients in whom ETI was appropriate.
OR 0.4 (95% CI 0.3–0.8) p value 0.02.
Borg dyspnea scale.
In consideration of the narrative design of this review, we did not apply the methodology of systematic review aiming at producing evidence-based recommendations (i.e. Patient, Intervention, Comparison, Outcome (PICO), certainty of evidence, biases, desirable and undesirable effects). With this narrative review, we aim at reporting the pathophysiologic effects, the clinical impact, and the practical issues of the use of PP during CPAP in non-intubated, spontaneously breathing patients with ARF due to SARS-CoV-2.
Results
Physiologic effects of prone positioning
Respiratory mechanics
Moving from supine to PP changes the respiratory mechanics of the patient. The anterior chest wall, in contact with the fixed surface of the bed, cannot completely expand; at the same time, the dorsal chest wall has more freedom of movement but, due to the anatomical conformation of the thorax, it has less compliance than the anterior wall. The overall compliance of the chest wall is reduced, but is more homogeneous.26,27 The diaphragm elasticity does not change, but the abdominal compression force is redistributed across the diaphragm in a more homogeneous pattern, resulting in a relieved compression on the atelectatic basal dorsal regions. 28 Moreover, PP decreases the gravitational pressure of the anterior structures of the thorax (e.g. heart and mediastinum) upon the lungs. 29 The lung compliance improves, limiting the regional lung stress strain and reducing the risk of ventilation-induced lung injury in patients receiving IMV.30–32
Ventilation distribution and shape matching
In healthy, upright persons, the density of the lung increases along the vertical gravitational axis. As a result, there is a low regional gas volume relative to the tissue volume in the lower (dependent) lung areas, resulting in a ventilation/perfusion (V/Q) ratio gradient oriented along the gravitational axis. In the prone position, the gravitational redistribution of lung density changes: the dorsal areas become non-dependent, therefore the gas volume increases and the tissue volume decreases. To the contrary, the ventral areas become dependent, with the opposite effects.33–36 In the PP the gravitational gradient of perfusion is markedly reduced 37 and the gravitational distribution of V/Q ratio is more uniform, 38 decreasing the shunt fraction and improving oxygenation.32,39 V/Q ratio is also impacted in the PP by the “shape matching.” In supine position, the lungs can be modelled as conical structures positioned inside the cylindrical thoracic cage (the apex towards the ventral part of the thorax). This creates a great distention of the ventral lung regions (non-dependent zones). In prone position, the gravitational force collapses the ventral zone, but the anatomical regional expansion cushions this collapse thanks to shape matching, avoiding atelectasis.33–41 The result is a more uniform gravitational gradient of V/Q ratio. 38
CO2 clearance
The major dorsal recruitment compared to the ventral de-recruitment leads to a reduction of the overinflated areas and of the physiologic dead space, resulting in an increased number of opened and ventilated alveoli. The clearance of CO2 can improve, especially in patients with dynamic hyperinflation. 42 The reduction in PaCO2 in PP is associated with better clinical outcomes, both in patients with ARDS in IMV and in spontaneous breathing.43,44
Figure 1 summarizes the physiologic effects of PP.

Prone positioning-induced physiologic benefits.
Notably, we have to underline that all described physiologic effects of PP on mechanics, V/Q matching and CO2 clearance are manly demonstrated in intubated patients. To our best knowledge, the precise mechanisms underlying the effectiveness of pronation in COVID-19 pneumonia are not completely understood. It has been speculated that the rapid improvement in PaO2/FiO2 ratio observed under PP in noninvasively ventilated COVID-19 patients, is likely related to the degree of ventilation/perfusion mismatch and to the amount of atelectasis and consolidations developed in the lung parenchyma. 45
PP during CPAP therapy
Physiologic changes
PP combined with noninvasive respiratory therapies has been successfully applied to non-COVID-19-related ARF or moderate ARDS (PaO2/FIO2 100–200). It increased the PaO2/ FIO2 ratio and reduced the need for intubation with good tolerance.46,47 In patients with predominantly hypoxic respiratory failure, PP combined with CPAP may provide sufficient respiratory support, especially in paediatric patients in whom it decreases the inspiratory effort. 48
The 20–41% of patients affected by severe SARS-CoV-2 pneumonia can develop ARDS.49–52 Similar to ARDS from other causes, COVID-19 infection increases the capillary permeability, resulting in interstitial oedema, reduced surfactant and increased intrapulmonary shunt with altered V/Q ratio. 49 The efficiency of gas exchange is further reduced by inflammatory cell infiltration, desquamation of alveolar cells and the hyaline membrane formation. 53 Moreover, a deficit in the normal regulation of the lung perfusion, with a lack of hypoxemic vasoconstriction contributes to the deterioration of V/Q ratio.54,55 Initially, the respiratory mechanics are typically preserved, with a rapid and sudden deterioration in the advanced phases of disease. 49
In patients affected by SARS-CoV-2 pneumonia PP may help to reduce lung heterogeneity, to improve alveolar recruitment in dorsal regions, to decrease the ventral dead space and to achieve better V/Q matching, 56 improving the gas exchange.57,58 The more homogenous lung aeration with PP could result in reduced respiratory effort, which limits the lung stress strain and the risk of P-SILI especially if the patient is spontaneously breathing.11,24 Moreover, the reduction of the necessary FIO2 due to PP-associated improvement of oxygenation may reduce the risk of absorption atelectasis. 59 Because of these effects, early application of PP could reduce the overdistension of healthy lung zones, preserving gas exchange and reducing the need for ETI.60,61
Though conventional oxygen, HFNC and NIPPV may all be combined with PP in COVID-19-related ARF, CPAP delivered by helmet has some theoretical advantages over these other options. The effects of CPAP on the respiratory system are well described, and its use in treating ARF has spread in the everyday real world of clinical practice. 62 CPAP may further assist by improving lung and thorax mechanics [compliance, functional residual capacity (FRC)], optimizing work of breathing, reducing atelectasis and stabilizing the airways (avoiding the open/closure of alveoli). Moreover, CPAP improves redistribution of lung perfusion (although it does not change the dorsal predominance of pulmonary perfusion 39 ) and decreases the intrapulmonary shunt, improving the V/Q ratio and gas exchanges.60,62–64 CPAP, compared to NIPPV, also has the desirable effect of being simple to apply and titrate, requiring only a pressure, flow and inspiratory fraction of oxygen (FIO2) to be specified. Compared to HFNC, CPAP provides higher mean airway pressures, without a need for the patient to keep a closed mouth. With a helmet interface, CPAP may also have a reduced risk of dislodgement during PP compared to the nasal interface of HFNC, resulting in increased safety for use outside of ICU.
PP delivered concomitantly to the helmet CPAP reduces the work of breathing 25 and improves the ROX index. 23 It appears to be safe and feasible for spontaneously breathing, non-intubated patients with COVID-19-related pneumonia, also outside the ICU.15,24,57 A recent study has demonstrated the efficacy of PP associated with CPAP in reducing the work of breathing, possibly lowering the risk of SILI and subjective dyspnea COVID-19 hypoxemic patients. 25 PP compared with usual care reduced the risk of ETI,24,65 the benefits of proning combined with CPAP upon mortality and ETI remains to be clarified.15,24,25,57,66 In patients with treatment limitation who do not wish to undergo ETI under any circumstances [e.g. Do Not Resuscitate (DNR) or Do Not Intubate (DNI)], PP is a reasonable rescue strategy if there is no response to conventional therapy.
Timing of PP: early application and pattern-disease linkage
A better response to PP is observed when performed soon after hospital admission among patients with a more activated inflammatory response.15,24 One of the explanations for this finding is that there may be a higher proportion of potentially recruitable lung in the early phases of ARDS compared to later phases when lung compliance is preserved or increased. 67 This observation suggests that the application of PP could enhance lung recruitment in areas other than usual (i.e. basal dorsal) atelectatic regions. The pre-COVID study of Cammarota et al. demonstrated that recruitment manoeuvres during noninvasive CPAP in patients with ARF and bilateral lung involvement entail a better oxygenation than in those with unilateral involvement. 68 This also suggests the possibility of a higher efficacy of PP in patients with extensive bilateral SARS-CoV-2 pneumonia. Tonelli et al. found that a diffuse, patchy pattern on chest CT scan was independently associated with NIPPV failure; this pattern probably correlated to pulmonary vascular endothelitis, thrombosis and angiogenesis, which can complicate COVID-19. 24
Three distinct phenotypes of SARS-CoV-2 pneumonia,49,69 suggest varied strategies for applying CPAP:
A CT pattern characterized by multiple focal ground-glass opacity (GGO) areas associated to overperfusion (normal-high compliance, low recruitability, phenotype L according to Gattinoni or “non-ARDS” type 1). At this stage, keeping a low inspiratory pressure is crucial. PP associated to moderate levels of PEEP (8–10 cm H2O) may improve V/Q ratio and decrease stress and strain redistribution with a minor risk of P-SILI, allowing patients more time to heal. 60
A transition pattern with atelectasis and peribronchial opacity, especially in dependent areas in which PP along with moderate-high levels of PEEP (10–12 cm H2O), works primarily by recruiting the non-ventilated areas. 22
ARDS-likely pattern (low compliance, high recruitability, phenotype H according to Gattinoni), with extensive bilateral infiltrates of non-aerated tissue, which should be treated as severe ARDS with PP associated with high levels of PEEP (>12 cm H2O), often progressing to requiring the need for ETI. 49
Setting and duration of proning positioning sessions
When initiating a trial PP with CPAP, the initial settings can remain the same as in supine position, with levels of PEEP (8–12 cm H2O) titrated to patient need. While low levels of PEEP could promote the collapse of small airways at the end of expiration, 70 high levels of PEEP may increase the hyperinflation at the end of expiration and cause hemodynamic instability. 70 Whether PP mitigates these effects remains to be clarified. Tolerance of therapy is associated with improved survival and should be supported. 18 Strategies to enhance tolerability and prolong the session of PP on CPAP include:
– Training the patient to collaborate during the manoeuvre of pronation/supination to minimize the need for healthcare workers (HCWs) to assist, improving patient comfort and reducing the accidental removal of the devices. When applied to non-intubated patients, the feasibility of PP is more dependent upon patient’s compliance rather than on the number of dedicated personnel. 22 Education about the value of PP, and its ability to reduce the need for ETI may help to motivate patients and increase compliance.
– Supporting patient comfort using pillows or sheets under the ventral thoracic wall and the neck. Being careful not to increase the intra-abdominal pressure, that significantly decreases the stroke volume and increases the heart rate. 71
– Ensuring a call bell available to the patient to ensure rapid assistance, if needed.
– Choosing an interface that is comfortable for the patient. It is not clear if the benefits of the helmet in terms of tolerance and safety for HCWs are also present during PP.22,72,73 If a helmet is used, those without armpit belts or rigid collars are preferred.74,75
– Encouraging PP in obese patients if they are willing and if well tolerated. The benefits of PP may be even more pronounced in obese patients. 76 However, PP may not be feasible in severely obese patients, limiting its applicability.
– Using light sedation (morphine and/or dexmedetomidine) alongside CPAP, within an appropriately monitored setting.16,19
– Using a semi-prone position or a tripod position in patients unable to adopt a full prone position.23,77
The duration of PP in non-intubated, spontaneously breathing patients is likely to be shorter than the 16 h recommended in intubated, mechanically ventilated patients, although a shorter duration of the sessions may reduce the effectiveness of PP. 24 In published studies, the duration of the sessions of PP during CPAP ranges between 1 and 13 consecutive hours, with better outcomes demonstrated when PP is performed for long periods (e.g. more than 10 h/d). 22 To obtain a better adherence to treatment, intermittent PP of periods of 2–3 h three times a day, interspersed with breaks for personal care, is a reasonable approach.
Practical issues of pronation
Most published literature on PP describes the technique in intubated unconscious patients, in which 5 HCWs and a large quantity and variety of supports are used to check the postural changes steps. There are few descriptions of how to implement PP in awake patients. Teaching patients PP may be particularly challenging in patients treated with CPAP or NIPPV delivered through the helmet, due to verbal communication difficulties from high flow related noise and the physical barrier between the patient and HCWs. To ensure safe and efficient PP, there should be a shared mental model for awake proning amongst all HCWs involved, including both a theoretical and practical knowledge of the manoeuvre. Practical training in small groups should be implemented, involving physiotherapists and nurses. In patients using CPAP with helmet interface, pairs of HCWs, including a physiotherapist or a nurse, assisted the patient in turning, supervised by a medical doctor who checked the subject’s clinical parameters before, during and after the manoeuvre. In some cases, patients may be able to turn themselves with gentle supervision only, and in other cases, it may be helpful for the patient to be as passive as possible, using high-sliding sheets, which the HCWs use to turn the patient. This helps to shorten the time needed for the postural changes, safely manage the helmet, and increase control of lines and devices.
Table 2 reports the activities to be performed before, during and after the pronation and supination manoeuvres.
Safety and practical aspects of proning positioning manoeuvre during CPAP.
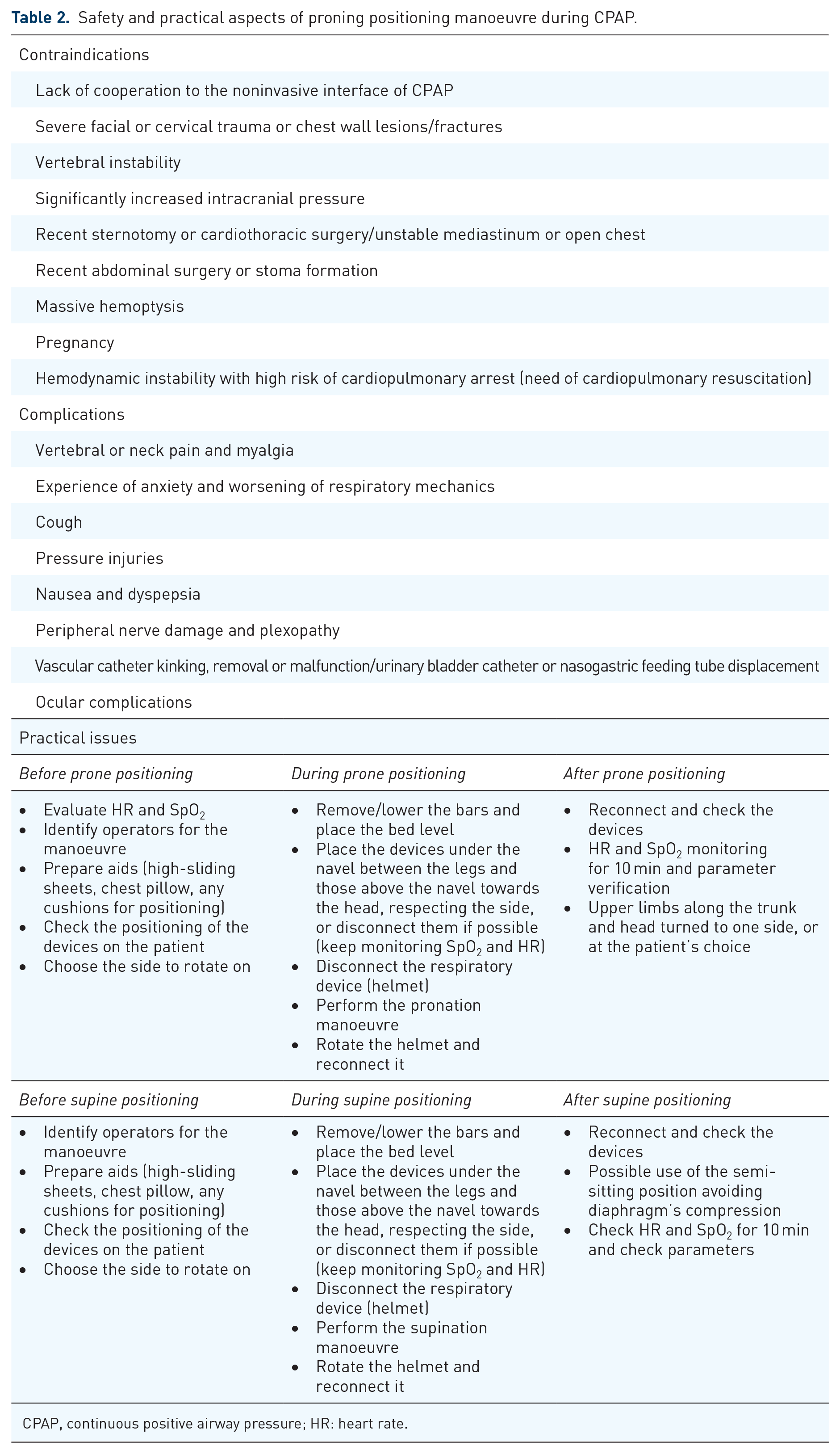
CPAP, continuous positive airway pressure; HR: heart rate.
Figure 2 shows a subject in PP during COVID-19 pandemic.

Patient in prone position receiving CPAP delivered by the helmet. The comfort of the patient got better with a small pillow under the chest and another one under the head.
Drawbacks and failure
PP has some contraindications76,78 and possible complications, listed in Table 2.15,16,19,20,22,23,79–82
Compared to PP during IMV, conscious patients are able to adjust their position, monitor their own devices, and call for assistance, which may contribute to the lower complication rate. 15,23,32,57
A potential risk of applying noninvasive respiratory therapies in patients with COVID-19-related ARF is the delay in intubation and IMV.7,83 Close clinical monitoring for early identification of treatment failure during PP, despite a correct position and the absence of an unintentional leak, is essential. Common criteria used to determine PP inefficacy include SpO2 < 90%, PaO2/ FIO2 < 100, unchanged PaO2, intolerance or signs of respiratory distress.15,18,19,20 It is unclear how long a trial of PP on CPAP should continue as there is little evidence of predictors of PP and CPAP failure. In general, as a patients FIO2 requirements improve, proning can be gradually discontinued and weaned along with other respiratory supports. However, evidence guiding discontinuation of PP is limited.
Conclusion
PP provides unique physiologic benefits in patients with ARF, such as patients with SARS-CoV-2 pneumonia. While awake PP can be combined with most forms of noninvasive respiratory support, the combination of PP with CPAP has unique benefits. It is possible to speculate on the role of PP during CPAP in terms of improvement of ventilation mechanics and reduction of strain stress and SILI, which could increase the use of PP in the early phase of the disease. In our review of existing literature, the use of PP with CPAP in patients with hypoxic ARF is feasible and may be safe for some patients outside of the ICU, given its simplicity compared to NIPPV. Compared to patients receiving IMV, awake PP in CPAP appears to have a reduced risk of adverse events, especially in terms of dislodgment of surgical devices or skin and nerve pressure injuries. Given the reduction in intubation with the use of awake PP and in COVID-19, the combination of PP CPAP may represent an attractive therapeutic in many settings.
We should acknowledge the limitations of this narrative review, that could not provide evidence-based recommendations on the application of PP under CPAP in COVID-19 hypoxemic patients as compared to other comparators (i.e. non-proning strategy, PP under NIPPV or HFNC).