
Abstract
Excessive dynamic airway collapse (EDAC) is characterized by abnormal airway collapse during expiration, leading to symptoms such as breathlessness, cough, and reduced quality of life. Treatment options remain limited, and evidence-based guidelines are lacking. This prospective cohort study evaluated the impact of positive airway pressure (PAP) therapy on symptom burden in 23 patients with EDAC referred to a tertiary ventilation centre. Diagnosis was confirmed by computed tomography and/or bronchoscopy. Patients received nocturnal and ambulatory PAP, with symptom ratings and quality of life assessed at baseline and after three months. PAP therapy produced rapid and sustained improvements in breathlessness, orthopnoea, cough frequency, sleep quality, and quality of life, with significant differences in all domains (p < 0.01). Adherence to nocturnal PAP was high. These findings suggest that PAP therapy is an effective symptomatic intervention in EDAC and support consideration of EDAC as an indication for PAP therapy in future clinical guidelines.
Keywords
Dear editor,
Excessive dynamic airway collapse (EDAC) is a condition characterised by abnormal collapse of the airways during the respiratory cycle. There are no fixed criteria to diagnose EDAC but a definition used in the literature is of 50% airway collapse in the horizontal cross-section area of the airway during expiration/coughing. 1 The aetiology of EDAC is broad but has associations with prolonged endotracheal intubation/tracheostomy, chronic obstructive pulmonary disease, gastroesophageal reflux, obesity, relapsing polychondritis, and smoking. 2 It is largely under-recognised and under-diagnosed, as it can be challenging to diagnose; however, it can result in debilitating symptomatology. It is often misdiagnosed as asthma due to the clinical presentation. Patients frequently complain of symptoms related to increased airway resistance (breathlessness and wheeze) as well as chronic cough and reduced exercise tolerance. In addition, individuals may suffer from poor sleep quality and report reduced health-related quality of life (QoL). There are no evidence-based guidelines to advise on the appropriate management of patients with EDAC. Treatment options include medical interventions to treat the associated conditions (such as bronchodilators and corticosteroids for chronic obstructive pulmonary disease, or proton-pump inhibitors for gastroesophageal reflux), bronchoscopic interventions such as tracheal stents and surgical options such as tracheobronchoplasty. 2 Positive airway pressure (PAP) therapy is increasingly recognised as a useful intervention in patients with EDAC to splint the airway, although there are no randomised clinical trials to provide robust evidence for its use. In this study, we report on the impact of PAP therapy on the symptom burden of patients with EDAC.
This was a prospective cohort study of consecutive EDAC patients referred to a tertiary ventilation centre for consideration of PAP therapy. Our institution determined that ethical approval was not required; the study was registered as a clinical audit (Ref number: 11811). The inclusion criterion was a diagnosis of EDAC based on computed tomography (CT) and/or bronchoscopy examination. Before initiation of PAP therapy, individuals underwent lung function testing and overnight pulse oximetry. Patients were asked to rate their symptom burden (breathlessness at rest, breathlessness on exertion, orthopnoea, cough frequency) on a categorical Likert scale (0 = none, 10 = maximal). They were also asked to rate their sleep quality and QoL (0 = worst possible, 10 = best possible). They were offered ambulatory PAP for use during the daytime (Z1TM Auto, Breas Medical). Nocturnal PAP was delivered using a full-face mask and ambulatory PAP delivered using a nasal mask. At 3-months following initiation of overnight PAP therapy, they were asked to provide the ratings again. Data were presented as mean ± standard deviation if normally distributed, or median (interquartile range) if not. Symptom burden prior and following initiation of PAP therapy was compared using a Wilcoxon matched-pairs signed rank test. Statistical analyses were performed using SPSS Statistics v29.0.1 (IBM Corp, New York, USA). A p-value <0.05 was considered significant.
Baseline demographics, lung function results and overnight pulse oximetry.

Symptom scores.
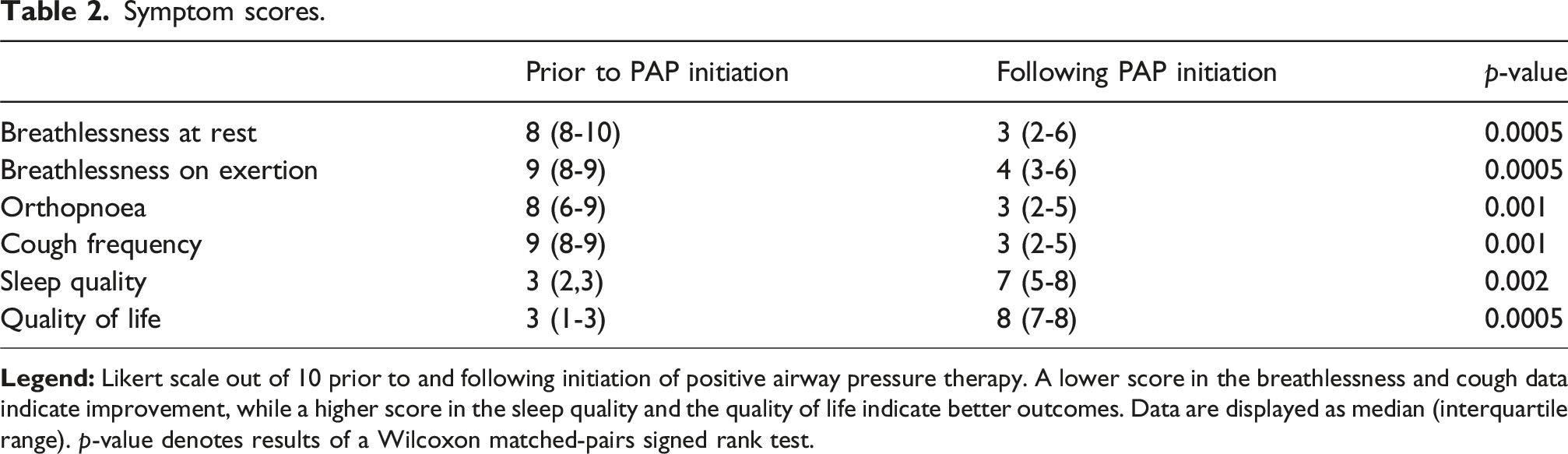
In individuals with EDAC, 3 months of overnight PAP therapy resulted in a significant improvement in breathlessness, orthopnoea, cough frequency, sleep quality and QoL. Although current international guidelines do not include EDAC as an indication for starting PAP therapy, these data suggest it should be considered a therapeutic option for patients suffering from symptomatic EDAC.
There are limited data reporting on the effect of PAP therapy in patients with EDAC. A retrospective review of 13 patients with relapsing polychondritis and EDAC reported that of the seven patients who were offered PAP therapy, five were able to tolerate it. 3 In our cohort, all patients were able to tolerate PAP therapy, with good adherence to nocturnal PAP. A retrospective cohort study in patients with EDAC who were initiated on PAP reported that 80% of patients had an improvement in their sleep and 29% had an improvement in their respiratory symptoms. 4 In our cohort, almost all patients reported improvements in both sleep and respiratory symptoms. It is unclear why PAP therapy provides such a dramatic improvement in symptoms. The overnight oximetry data demonstrate that these patients do not tend to desaturate overnight, suggesting that airway patency is maintained, which is what PAP therapy ordinarily targets. A case series reporting on the investigation of patients radiologically and bronchoscopically with and without PAP therapy demonstrated that PAP therapy resulted in a considerable increase in the diameter of the airway; thus, it can be hypothesised that it is the mechanical impact of PAP on the large airways that provides benefit to patients. The pneumatic stenting may abolish arousals that are not elicited in the ODI recorded by the overnight oximetry, and thereby improve sleep quality. Investigating this would require patients to undergo polysomnography as part of their clinical assessment. In addition, in doing this, PAP is stabilising the airway during the most demanding part of resting breathing, namely, in the supine position and during sleep. Stabilising the airway may accommodate the more efficient excretion of secretions, resulting in a decrease in airway resistance. By reducing airway resistance, the overnight work of breathing would improve, facilitating rest of the respiratory muscles. This may in turn result in improved capacity of the respiratory muscle pump during the daytime, resulting in less breathlessness. It is unclear why patients did not tolerate ambulatory PAP as well as nocturnal PAP. A potential explanation is the stigma around device use during the daytime, especially when ambulating outside of the home. A limitation of this work is that it reports a small cohort of patients; however, it represents the incidence of EDAC at a specialist referral centre for PAP therapy over 2 years. In conclusion, PAP therapy can provide considerable benefit to the symptomatic burden of patients with EDAC. Although it does not feature as an indication for PAP therapy in current guidelines, patients with EDAC should be considered candidates for PAP therapy. Future work should look to understand the pathophysiology to explain why PAP provides substantial benefit to these patients, and to facilitate appropriate selection of responders to this type of treatment.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.