
Abstract
Objective
To investigate the effectiveness and safety of non-invasive high-frequency oscillatory ventilation (NHFOV) in post-extubation preterm infants.
Methods
This was a randomized, controlled trial. A total of 149 preterm infants aged between 25 to 34 weeks’ gestational age with a birth weight of <1500 g who required invasive mechanical ventilation on admission were included. After extubation, they were randomized to the NHFOV group (n = 47), nasal intermittent positive pressure ventilation (NIPPV) group (n = 51), or nasal continuous positive airway pressure (NCPAP) group (n = 51). We compared the effectiveness and safety among these three groups.
Results
A total of 139 preterm infants finally completed the study. The reintubation rate was significantly lower in the NHFOV group than in the other groups. The duration of non-invasive ventilation and the length of hospital stay in the NHFOV and NIPPV groups were significantly shorter than those in the NCPAP group. The incidence of bronchopulmonary dysplasia in the NHFOV and NIPPV groups was significantly lower than that in the NCPAP group. The NHFOV group had significantly less nasal injury than the NCPAP group.
Conclusion
As post-extubation respiratory support in preterm infants, NHFOV has a lower reintubation rate compared with NCPAP and NIPPV, without increasing the rate of complications.
Keywords
Introduction
Preterm infants are prone to various conditions because of the immaturity of their organs. Respiratory immaturity can lead to respiratory failure, resulting in a decrease in the arterial partial pressure of oxygen (PaO2) and/or an increase in the arterial partial pressure of carbon dioxide (PaCO2). 1 Respiratory immaturity is a leading cause of mortality and morbidity in preterm infants. In recent years, development of neonatal critical care, particularly the innovation of neonatal-assisted ventilation, has led to an improved neonatal survival rate. However, long-term ventilation results in volutrauma and/or barotrauma, which leads to ventilator-associated injuries, such as bronchopulmonary dysplasia (BPD), and causes long-term morbidity for premature infants. 2 Guidelines from the United States and Europe recommend early use of non-invasive ventilation in preterm infants.3,4 While 43% to 80% of preterm infants with moderate or severe respiratory failure still require intubation on invasive mechanical ventilator, 5 16% to 40% of them have difficulty in extubation. 6
Nasal continuous positive airway pressure (NCPAP) is a traditional mode of non-invasive ventilation for preventing failure of extubation in preterm infants by maintaining functional residual capacity and patency of the upper airway. 7 However, complications caused by NCPAP, such as nasal injury, abdominal distension, and air leakage, have a large effect on clinical efficacy. 8 Approximately 30% of infants who are extubated to NCPAP require reintubation owing to retention of CO2 or hypoxemia. 9 Non-invasive positive pressure ventilation (NIPPV) might be superior to NCPAP for decreasing respiratory failure and the requirement for intubation and mechanical ventilation. However, NIPPV requires synchronization to achieve effective ventilation.10,11 Preterm infants have a relatively high respiratory rate and there is inevitable leakage during non-invasive ventilation, which may affect the flow trigger during synchronization process in non-invasive ventilation. Therefore, valid synchronization in non-invasive ventilation is still difficult to achieve. 12 Non-invasive high-frequency oscillatory ventilation (NHFOV) is a new mode of non-invasive ventilation that connects non-invasive circuits to high-frequency ventilators, through which gas exchange is achieved by the superposition of high-frequency oscillation over continuous positive flow. Compared with other non-invasive ventilation modes, NHFOV combines the advantages of NCPAP and high-frequency ventilation, making it more effective at maintaining alveolar stability, eliminating CO2, and limiting barotrauma. 13
Previous studies have described comparison between NCPAP and NIPPV or NHFOV.11,14 Most of these studies had a small sample size and few studies compared NHFOV with NIPPV. Therefore, this study aimed to investigate whether NHFOV as post-extubation respiratory support reduces the reintubation rate in preterm infants compared with NIPPV and NCPAP.
Methods
Participants
We performed a randomized, controlled trial. This study was registered at http://www.chictr.org.cn (ID: ChiCTR1900024289). A total of 149 eligible preterm infants who required invasive mechanical ventilation on admission and were hospitalized at Guangxi Maternal and Child Health Hospital between 1 April 2017 and 31 October 2018 were included. Patients were recruited after intubation and written consent from the patients’ guardians was obtained. This study was approved by the Medical Ethics Committee of Guangxi Maternal and Child Health Hospital on 30 March 2017 in Nanning, Guangxi, China ([2017]MESA[5-1]). Before extubation, the preterm infants were randomized to either the NHFOV group, the NIPPV group, or the NCPAP group (Figure 1).

CONSORT flow diagram.
Inclusion criteria
The inclusion criteria were as follows: 1) preterm infants with a gestational age (GA) of 25 + 0 weeks to 33 + 6 weeks and a birth weight of <1500 g; 2) preterm infants met the criteria of intubation 15 requiring invasive mechanical ventilation of any mode on admission; 3) only the first extubation from invasive ventilation was included in this study; and 4) informed consent was obtained from a guardian.
Exclusion criteria
The exclusion criteria were as follows: 1) preterm infants with major life-threatening congenital malformations; 2) preterm infants who died within 24 hours after admission; 3) preterm infants with an abnormal upper airway structure (e.g., Pierre–Robin’s syndrome, congenital laryngomalacia, choanal atresia, and severe nose injury); and 4) preterm infants with surgical conditions requiring surgery before extubation. These conditions included congenital diaphragmatic hernia, congenital tracheal esophageal fistula, gastrointestinal malformations, and complex congenital heart disease, but did not include ligation of patent ductus arteriosus (PDA) and surgical necrotizing enterocolitis (NEC). Further exclusion criteria were preterm infants who had grade IV intraventricular hemorrhage (IVH) before extubation, and those with congenital pulmonary hypoplasia or surfactant protein B deficiency.
Interventions
Participants pre- and post-extubation had their ventilatory settings adjusted on the basis of blood gases, transcutaneous oxygen saturation, and clinical conditions. Preterm infants were weaned to non-invasive respiratory support when extubation criteria were met and they were reintubated if their respiratory condition deteriorated or they were on non-invasive support. All respiratory management was performed by clinicians who did not belong to the study team.
Criteria for extubation
Preterm infants received extubation using the following criteria: 1) they received caffeine citrate treatment (loading dose of 20 mg/kg, maintenance dose of 5 mg/kg/day) before extubation; 2) arterial blood gases were within the target range (pH ≥7.20, PaO2 ≥50 mmHg, and PaCO2 ≤60 mmHg) with a low mechanical ventilation setting (mean airway pressure [MAP] ≤7 cm H2O, fraction of inspired oxygen (FiO2) ≤30%); 3) spontaneous breathing occurred; and 4) they were hemodynamically stable.
NHFOV group
NHFOV was generated by the Fabian HFO machine (Acutronic Medical System AG, Hirzel, Switzerland). The NHFOV machine was connected to preterm infants through binasal prongs (size: small, medium, or large; diameter: 2.50, 3.15, or 3.80 mm; NeoJet System; Löwenstein Medical GmbH & Co. KG, Bad Ems, Germany). A nasal mask was not available in Guangxi market during the study period, and therefore, we were not able to use this mask. The initial settings were as follows: frequency of 10 Hz (regulation range, 6–12 Hz), MAP of 10 cm H2O (regulation range, 6–12 cm H2O), inspiration time of 33%, and amplitude of 25 cm H2O (regulation range, 25–50 cm H2O). Hypercapnia was corrected by increasing the amplitude or decreasing the frequency, but increasing the amplitude was preferred. 16 FiO2 was adjusted in the range from 0.21 to 0.40 to maintain a target oxygen saturation in arterial blood (SpO2) of 90% to 95%. Hypoxia was corrected by increasing MAP and/or FiO2. Visible jaw oscillation was appropriate, and visible chest oscillation was not always necessary in NHFOV because a major part of CO2 clearance occurs in the upper airway dead space. 17
NIPPV group
The Comen NV8 machine (Shenzhen Comen Medical Instruments Co. Ltd., Shenzhen, China) was used for preterm infants who were assigned to the NIPPV group. The NIPPV machine was connected to preterm infants through binasal prongs (size: small, medium, or large; diameter: 2.50, 3.15, or 3.80 mm; NeoJet System). The initial settings were as follows: positive end-expiratory pressure (PEEP) of 4 cm H2O (regulation range, 4–8 cm H2O), positive peak pressure of 15 cm H2O (regulation range, 15–25 cm H2O), inspiratory time of 0.45 to 0.5 s, respiratory rate of 30 breaths per minute (regulation range, 15–40 breaths per minute), and hypercapnia could be corrected by increasing the respiratory rate. FiO2 was adjusted from 0.21 to 0.40 to maintain a target SpO2 of 90% to 95%. Hypoxia was corrected by increasing MAP and/or FiO2.
NCPAP group
The Fabian HFO machine (Acutronic Medical System) was used for preterm infants who were assigned to the NCPAP group. The NCPAP machine was connected to preterm infants through binasal prongs (size: small, medium, or large; diameter: 2.50, 3.15, or 3.80 mm; NeoJet System). The initial settings were as follows: PEEP of 5 cm H2O (regulation range, 3–8 cm H2O). FiO2 was adjusted from 0.21 to 0.40 to maintain a target SpO2 of 90% to 95%. Hypoxia was corrected by increasing PEEP and/or FiO2.
Criteria for discontinuing non-invasive ventilation for each group
The criteria for discontinuing non-invasive ventilation with settings were as follows: for the NHFO group, MAP was <6 cm H2O and FiO2 was <30%; for the NIPPV group, positive peak pressure was <14 cm H2O, PEEP was <4 cm H2O, the respiratory rate was <15 breaths per minute, and FiO2 was <30%; for the NCPAP group, PEEP was <4 to 5 cm H2O, and FiO2 was <30%. Additionally, no apnea or bradycardia requiring stimulation for at least 24 hours was required for discontinuation. Preterm infants who met the criteria were weaned to high-flow humidified oxygen.
Criteria for restarting non-invasive ventilation
The criteria for restarting non-invasive ventilation were as follows: FiO2 >30% and SpO2 <85% constantly; a Silverman Score 18 of 3 to 5 points; and more than three self-resolving apneas within 24 hours. Preterm infants were revaluated for discontinuing non-invasive ventilation again at least 48 hours after restarting.
Criteria for reintubation
Criteria for reintubation were as follows: 1) respiratory acidosis (pH <7.20 and PaCO2 >60 mmHg); 2) hypoxemia (SpO2 <90% constantly, despite FiO2 up to 40%); 3) recurrent apnea (defined as at least three times of self-resolving apnea or bradycardia within 1 hour, or one profound apnea event requiring positive pressure ventilation within 24 hours); 4) pulmonary hemorrhage or pneumothorax; 5) respiratory deterioration lasting for 4 hours (Silverman score ≥6); 6) hemodynamic instability (defined as mean arterial blood pressure lower than that for GA, requiring dopamine or dobutamine exceeding 5 µg/kg/minute, or any dose of norepinephrine/epinephrine/milrinone/nitric oxide to maintain circulation); 7) cardiac arrest requiring intubation during resuscitation; and 8) reintubation within 7 days of the first extubation.
Outcomes
Primary outcome
The primary outcome was the rate of reintubation within 7 days of extubation.
Secondary outcomes
Secondary outcomes were the oxygenation index ([OI] = MAP×FiO2×100/PaO2) post-extubation, duration of non-invasive ventilation, duration of O2 supplementation, duration of parenteral nutrition, length of hospital stay, incidence rates of pneumothorax, BPD, ventilation-associated pneumonia, NEC (stage II and higher), retinopathy of prematurity (ROP) (stage II and higher), PDA, IVH (grade 3 and higher, Papile standard 1 ), and nasal injury, and girth while on non-invasive ventilation (measurements were taken at 48 and 96 hours after non-invasive ventilation).
Sample size calculation
The sample size was calculated using IBM SPSS software version 22 (IBM Corp, Armonk, NY, USA). Based on previous research,19,20 the reintubation rate within 1 week after extubation was 55% in VLBW infants (GA: 25–33 weeks) supported by NCPAP post-extubation. Furthermore, a previous study showed that NHFOV significantly reduced the reintubation rate compared with NCPAP (24.3% vs. 56.4%). 21 Therefore, according to our clinical experience, we estimated that the reintubation rate in the NHFOV group should be 30% or lower. Considering an alpha error rate of 0.05 and a power of 90%, 39 neonates needed to be enrolled in each arm (with a 1:1:1 design) to detect the same difference. Therefore, we planned to recruit at least 47 preterm infants in each group to account for dropouts.
Randomization
A computer-generated random numbers list was devised by an independent statistician to create sequentially numbered sealed opaque envelopes containing a card indicating the arm of randomization. After documenting parental consent, all preterm infants were assigned in a 1:1:1 ratio using a table of random numbers and sealed opaque envelopes to NCPAP, NHFOV, or NIPPV. The trial was blinded to parents, but blinding to the doctors was not possible owing to the nature of the intervention.
Statistical analysis
Data were analyzed using IBM SPSS 22.0 software (IBM Corp. Armonk, NY, USA). The Shapiro–Wilk and Kolmogorov–Smirnov tests were applied to determine normality. Measurement data with a normal distribution are expressed as mean ± standard deviation. Comparison of multiple means was performed by analysis of variance and two-two comparison was performed by the least significant difference method. Measurement data that were not normally distributed are expressed by the median (interquartile range) and were analyzed by the Kruskal–Wallis test. Categorical variables were analyzed by the chi-square or Fisher’s exact test. A p value of <0.05 was regarded as statistically significant.
Results
Baseline data
A total of 139 preterm infants finally completed the study, including 70 boys and 69 girls. The mean GA was 29±1.9 weeks and the mean weight was 1113.1±186.8 g. A total of 45, 47, and 47 preterm infants were assigned to the NHFOV, NIPPV, and NCPAP groups, respectively. There were no significant differences in baseline characteristics among the groups (Table 1).
Baseline characteristics of the preterm infants.

†Data are shown as median (interquartile range) or frequency (%); ‡data are shown as mean ± standard deviation.
¶Analyzed by the rank sum test; *analyzed by Fisher’s exact test.
NHFOV, non-invasive high-frequency oscillatory ventilation NIPPV, nasal intermittent positive pressure ventilation; NCPAP, nasal continuous positive airway pressure; GA, gestational age; BW, body weight; IUGR, intrauterine growth retardation; CRIB, clinical risk index for babies; MV, mechanical ventilation; OI, oxygenation index; PaCO2, arterial partial pressure of carbon dioxide.
Outcomes
Primary outcome
The reintubation rate in the NHFOV group was significantly lower than that in the NIPPV and NCPAP groups (p = 0.035 and p < 0.001, respectively). The reintubation rate in the NIPPV group was significantly lower than that in the NCPAP group (p = 0.006) (Table 2).
Reintubation rate of the preterm infants.

NHFOV, non-invasive high-frequency oscillatory ventilation NIPPV, nasal intermittent positive pressure ventilation; NCPAP, nasal continuous positive airway pressure; OR, odds ratio; CI, confidence interval.
Secondary outcomes
At 6 hours post-extubation, the NHFOV and NIPPV groups had a lower OI compared with the NCPAP group (p < 0.001 and 0.026, respectively). The pH value in the NHFOV group was significantly higher than that in the NIPPV and NCPAP groups 6 hours after treatment (p = 0.004 and p < 0.001, respectively). PaCO2 in the NHFOV group was significantly lower than that in the NCPAP group 6 hours after treatment (p = 0.002) (Table 3).
Respiratory status of preterm infants after non-invasive ventilation.

Data are shown as mean ± standard deviation.
NHFOV, non-invasive high-frequency oscillatory ventilation NIPPV, nasal intermittent positive pressure ventilation; NCPAP, nasal continuous positive airway pressure; OI, oxygenation index; PaCO2, arterial partial pressure of carbon dioxide.
The duration of non-invasive ventilation and the length of hospital stay in the NHFOV and NIPPV groups were significantly shorter than those in the NCPAP group (all p < 0.05). The duration of non-invasive ventilation and the length of hospital stay in the NHFOV group appeared to be shorter than those in the NIPPV group, but this was not significant. The duration of parenteral nutrition and the duration of oxygen supplementation were similar among the three groups (Table 4).
Comparison of clinical data of preterm infants.

Data are shown as median (interquartile range).
PN, parenteral nutrition; NHFOV, non-invasive high-frequency oscillatory ventilation NIPPV, nasal intermittent positive pressure ventilation; NCPAP, nasal continuous positive airway pressure. Bold values indicate P < 0.05).
The incidence of BPD in the NHFOV and NIPPV groups was significantly lower than that in the NCPAP group (both p < 0.05). The NHFOV group had a significantly lower rate of nasal injury than that in the NCPAP group (p < 0.05). No pneumothorax occurred during the study period. The incidence of NEC (stage III and higher), ROP (stage III and higher), (PDA), and IVH (grade III and higher) was similar among the three groups. Abdominal girth while on non-invasive ventilation was also not significantly different among the three groups (Tables 5–8).
Morbidities of preterm infants.

†Data are shown as frequency (%); ‡data are shown as mean ± standard deviation.
*Analyzed by Fisher’s exact test.
ap<0.05, compared with the NCPAP group; bp<0.05, compared with the NCPAP group.
NHFOV, non-invasive high-frequency oscillatory ventilation NIPPV, nasal intermittent positive pressure ventilation; NCPAP, nasal continuous positive airway pressure; VAP, ventilation-associated pneumonia; BPD, bronchopulmonary dysplasia; NEC, necrotizing enterocolitis; ROP, retinopathy of prematurity; PDA, patent ductus arteriosus; IVH, intraventricular hemorrhage.
Morbidities in the NHFOV versus NIPPV groups.

NHFOV, non-invasive high-frequency oscillatory ventilation; NIPPV, nasal intermittent positive pressure ventilation; OR, odds ratio; CI, confidence interval; VAP, ventilation-associated pneumonia; BPD, bronchopulmonary dysplasia; NEC, necrotizing enterocolitis; ROP, retinopathy of prematurity; PDA, patent ductus arteriosus; IVH, intraventricular hemorrhage.
Morbidities in the NHFOV versus NCPAP groups.
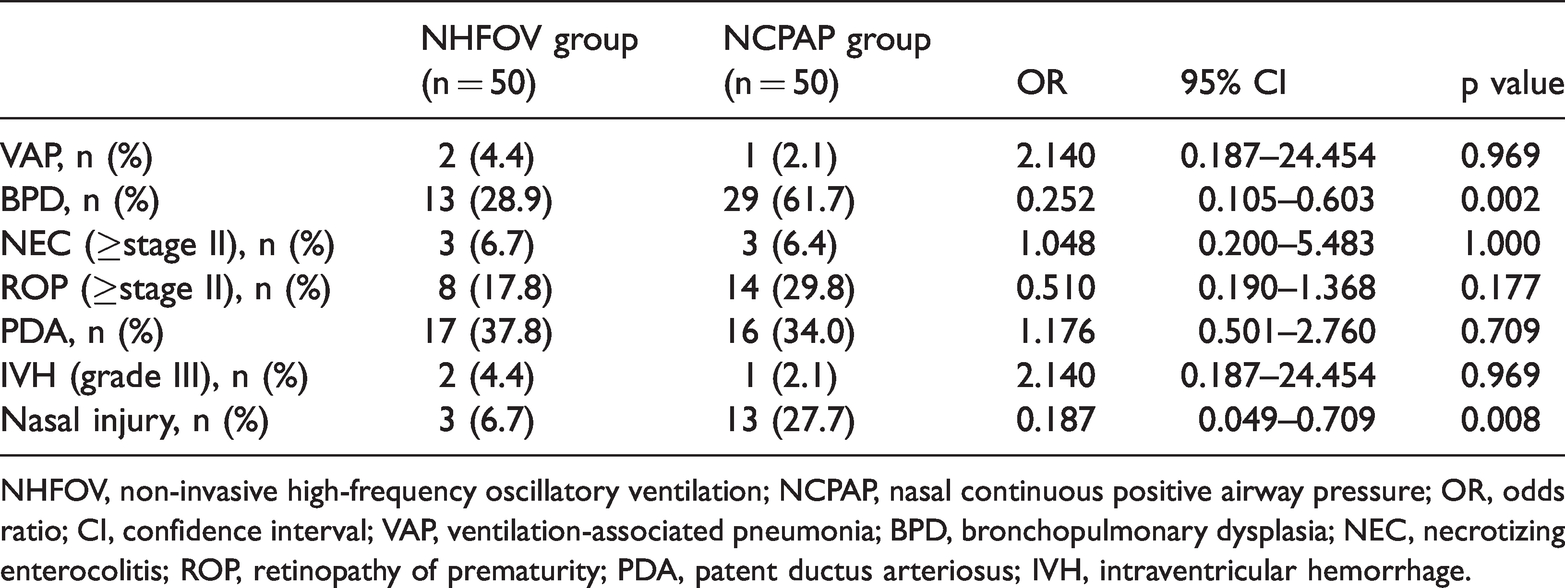
NHFOV, non-invasive high-frequency oscillatory ventilation; NCPAP, nasal continuous positive airway pressure; OR, odds ratio; CI, confidence interval; VAP, ventilation-associated pneumonia; BPD, bronchopulmonary dysplasia; NEC, necrotizing enterocolitis; ROP, retinopathy of prematurity; PDA, patent ductus arteriosus; IVH, intraventricular hemorrhage.
Morbidities in the NIPPV versus NCPAP groups.
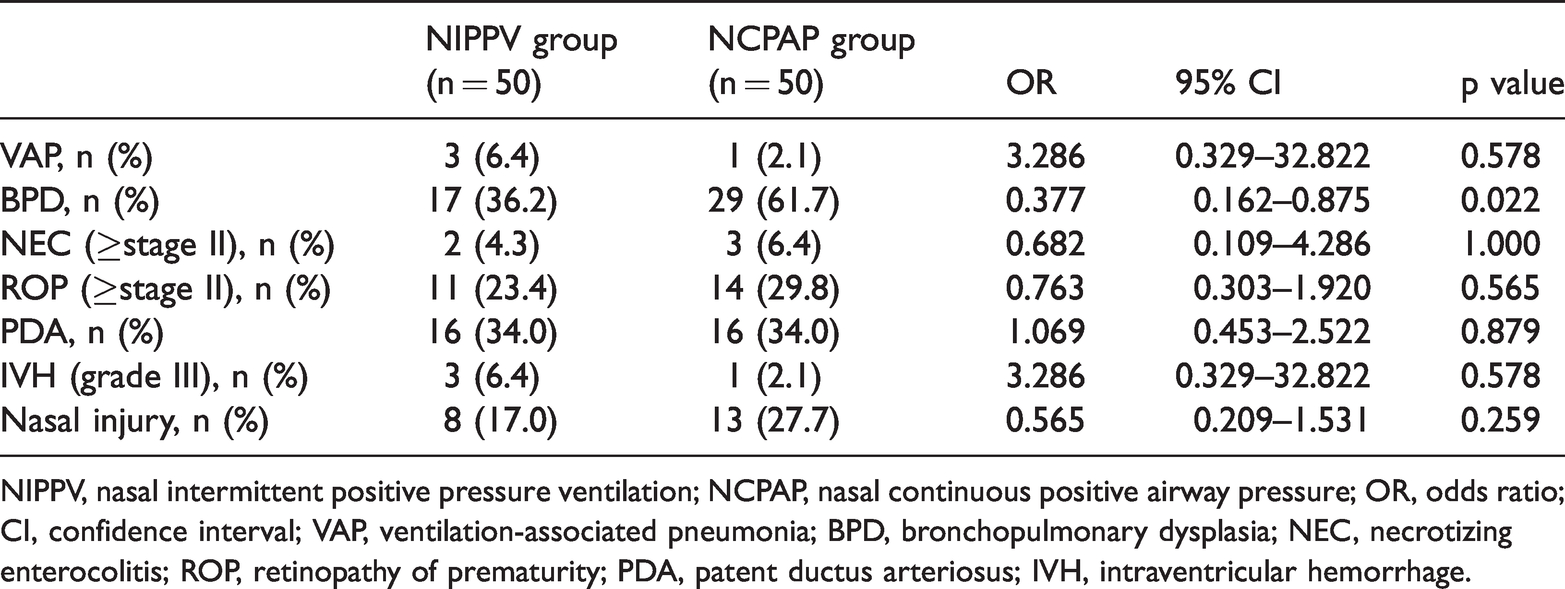
NIPPV, nasal intermittent positive pressure ventilation; NCPAP, nasal continuous positive airway pressure; OR, odds ratio; CI, confidence interval; VAP, ventilation-associated pneumonia; BPD, bronchopulmonary dysplasia; NEC, necrotizing enterocolitis; ROP, retinopathy of prematurity; PDA, patent ductus arteriosus; IVH, intraventricular hemorrhage.
Discussion
This study showed that the reintubation rate in the NHFOV group was significantly lower than that in the NIPPV and NCPAP groups. Previous studies have reported that when infants with BPD have difficulty in extubation, NHFOV is more effective than other modalities in reducing the risk of reintubation.22,23 One study showed that 89% of participants successfully avoided intubation or reintubation after using NHFOV, and there was a significant decrease in the incidence of apnea and desaturation when using NHFOV as rescue therapy. 24 Chen et al. 25 reported that NHFOV was superior to NCPAP in preventing reintubation of infants with respiratory distress syndrome (RDS). Our study also showed that NHFOV improved the OI and respiratory acidosis at post-extubation in preterm infants. Klotz et al. 26 studied 26 premature infants with a GA of 27±2 weeks after extubation or non-invasive surfactant treatment. These infants were treated with 4 hours of NHFOV and 4 hours of NCPAP in a cross-over design. This previous study did not show increased carbon dioxide clearance with NHFOV compared with NCPAP. Malakian et al. 14 reported that, in infants with RDS, NHFOV did not reduce the requirement for mechanical ventilation, but the duration of non-invasive ventilation in the NHFOV group was significantly shorter than that in the NCPAP group. There were some differences between the two studies mentioned above and our study. One probable reason for these differences was the cause of respiratory failure. The study population in these two previous studies was premature infants who were diagnosed with RDS. RDS is primarily restrictive in the acute phase, and therefore, high-frequency oscillation combined with CPAP does not lead to any benefit. In our study, the duration of non-invasive ventilation and the length of hospital stay were shorter in the NHFOV and NIPPV groups than in the NCPAP group, but there was no difference between the NHFOV and NIPPV groups. Zhang et al. 27 reported that the duration of non-invasive ventilation was significantly shorter in the NHFOV group than in the NIPPV group. Further studies regarding a reduction in duration of respiratory support using NHFOV or NIPPV are required.
Our study showed that the NHFOV and NIPPV groups had a lower incidence of BPD than that in the NCPAP group, while the incidence of BPD was similar in the NHFOV and NIPPV groups. Zhu et al. 28 performed a randomized trial that compared NHFOV and NCPAP treatment after surfactant therapy. These authors found that the NHFOV group had a lower rate of BPD than that in the NCPAP group, but the difference was not significant. In Zhang et al.’s retrospective study, 27 42 infants received NHFOV or NIPPV treatment, and the incidence of BPD was similar in the two groups, which is consistent with our study. When using NHFOV, attenuation of intra-tracheal pressure leads to low alveolar pressure. This maintains the end-expiratory volume at a normal level without causing atelectatic trauma in lung parenchyma, thus reducing the risk for BPD. 29 In our study, use of NHFOV resulted in avoiding more times of reintubation than the other two groups, and preterm infants who received NHFOV were weaned off non-invasive support sooner. The finding that respiratory support was shorter in the NHFOV group might also have contributed to the reduction in BPD.
We did not find any significant difference in the incidence of NEC, ROP, PDA, or IVH, or changes in abdominal girth among the three treatment arms. No pneumothorax occurred in any of the preterm infants. Previous studies showed similar results, and no study has shown an increase in brain injury, NEC, ROP, or air leakage related to NHFOV.22,30 Our study showed a significant reduction in nasal trauma in the NHFOV group compared with the NCPAP group. Malakian et al. 14 reported that there was no difference in nasal trauma between the NHFOV and NCPAP groups. The reason for this difference between studies might be the shorter treatment duration in the NHFOV group in Malakian et al.’s 14 study than in our study.
The major limitations of the present study are as follows. 1) This was a single-center study with a small sample size. 2) We did not match MAP between modalities. The settings and subsequent adjustments of respiratory support followed the clinical protocol of our center. Therefore, a high MAP may have mitigated the results more than the modality of non-invasive ventilation itself. 3) We used only one type of ventilator to deliver NHFOV, which might limit generalizability of our results. These limitations might have induced potential bias, including a restricted scope of application.
In conclusion, when using post-extubation respiratory support in preterm infants, NHFOV has a lower reintubation rate compared with NCPAP and NIPPV, without increasing complications. NHFOV is a mode of non-invasive respiratory support with great potential in treating premature infants. However, more studies regarding this topic are required in the future.
Footnotes
Author contributions
Drs. Yan Li, Qiufen Wei, Danni Zhong, and Xinnian Pan contributed to conception and design of the study. Drs. Yan Li, Liping Yao, Lingxiao Li, Wei Tan, Jiayan Yao, and Wei Dai prepared materials, and performed data collection and analysis. The first draft of the manuscript was written by Drs. Yan Li, Dan Zhao, and Yan Mo, and all authors provided comments on the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received funding from Beijing RenZe Foundation and Guangxi Medical and Health Key Discipline Construction Project.