
Abstract
Bronchial lipoma is a rare benign tumor of the lung, which is often misdiagnosed due to concomitant pulmonary diseases. In addition, the coexistence of endobronchial lipoma and lung cancer is extremely unusual. To date, no related computed tomography (CT) images have been reported. The patient was a 53-year-old man, who was admitted to our hospital with cough, yellow phlegm, and fever for 1 week. The CT image showed an irregular mass in the medial segment of the right middle lobe (B4a) with surrounding ground glass opacity, and another solid nodule in the right lower lobe (B6b). Unfortunately, after 2 weeks of anti-inflammatory treatment, the bronchial invasion of the B4a nodule did not decrease significantly, so further bronchoscopy was carried out and tumor resection was performed using endoscopic mucosal resection with a ligation device (EMR-L). During the follow-up 4 months, it was found that the B6b nodule was marked enlargement and then removed. The lesions of the B4a and B6b were confirmed as endobronchial lipoma and squamous cell carcinoma (T1aN0M0) by histopathology and immunohistochemical staining, respectively, and no postoperative radiotherapy or chemotherapy was performed. Regrettably, after 29 months of follow-up, we observed recurrence and slow enlargement of the lipoma in its original location, progressive emphysema in both lungs, and solitary chest wall metastasis from the B6b squamous cell carcinoma that had been resected. Therefore, endobronchial endoscopy resection should be carefully selected for larger endobronchial lipoma. If it is accompanied by early squamous cell carcinoma (T1aN0M0), we still recommend active postoperative chemoradiotherapy.
Introduction
Endobronchial lipoma is a kind of benign tumor with a very low incidence, which mainly occurs in middle-aged male patients. It is commonly found in subcutaneous tissues with extremely rich adipocytes, and rarely occurs in the lung. In this context, bronchial lipoma involving lung cancer is extremely rare, with only four related literatures and another one referring recurrence.1–5 So far, there has been no literature report of bronchial lipoma accompanied by lung cancer and recurrence. In other related reports, bronchial lipoma neither coexisted with lung cancer nor recurred, and there was no support from laboratory, endoscopic and imaging data, and the results were only expressed in brief text. This is the first case report that the recurrent endobronchial lipoma complicated with lung cancer was definitely diagnosed by completing clinical data including imaging finding, laboratory examination, pathological diagnosis, endoscopic characteristics, and follow-up data.
The reporting of this study conforms to the CARE guidelines. 6 The CARE checklist is available in the Supplemental Material. In this report, a case report of endobronchial lipoma with rare concomitant disease and unusual prognosis was reported. The diagnosis and treatment process of the patient were analyzed and summarized in detail, and a wealth of relevant computed tomography (CT) imaging manifestations and pathological data were provided to improve the level of understanding of the disease among clinicians and radiologists.
Case presentation
A 53-year-old man was admitted to our hospital with cough, yellow phlegm, and fever for 1 week. He had other chest symptoms, such as right chest wall pain, chest tightness, and shortness of breath. His clinical records showed dyspnea without any wheeze, moist rales could be heard in the right lower lung, and other signs were normal. The patient has a history of hypertension and diabetes, but denies any history of underlying diseases such as heart, lung, liver, or kidney disease and has no history of smoking, alcohol, and surgery. With regard to laboratory tests, blood routine and high-sensitive C-reactive protein (hs-CRP) examination revealed that leukocyte count, neutrophil count, and hs-CRP levels were slightly increased: 11.99 ± 10 E9/L, 76%, 10.9 mg/L, respectively. In terms of tumor markers, only ferritin value was significantly increased to 613.72 ng/mL.
The patient was initially diagnosed with pneumonia after being consulted by a clinician, and then underwent a comprehensive CT examination. Under the lung window setting, the CT scan demonstrated an irregular mass in the medial segment of the right middle lobe (B4a) with surrounding ground glass opacity; under the soft tissue window setting, the lesion showed obvious heterogeneous enhancement, and multiple linear low-attenuation areas implied internal mucoid impaction (size, 10–20 mm; CT attenuation value, −82.7 HU) [Figure 1(a)], which was then misdiagnosed as bronchial mucocele with inflammatory atelectasis [Figure 1(b)]. Besides, another solid nodule was detected in the right lower lobe (B6b) [Figure 1(c)]. After 2 weeks of anti-inflammatory treatment, a CT scan was performed again and it was found that the lesion had not been absorbed.

CT showing an irregular mass with surrounding ground glass opacity in the right B4a (a). The lesion contents a focal area of homogenous fat attenuation (a) and multiple areas of associated mucoid impaction secondary to bronchial obstruction (b). Furthermore, a solid nodule was detected in the right B6b (
The patient underwent further bronchoscopy, which revealed a smooth, multilobulated, yellowish polypoid tumor at the bronchial opening of the right lower lobe (B4a), which completely obstructed the bronchial lumen [Figure 2(a)]. Therefore, the clinician removed the tumor by endoscopic mucosal resection with a ligation device (EMR-L) and cryosurgery, and postoperative pathology confirmed that the B4a tumor was an endobronchial lipoma [Figure 2(b) and (c)]. Final diagnosis of endobronchial lipoma was achieved based on histopathology and immunohistochemical stains. The histopathology revealed a large amount of mature adipose tissue accompanied with focal fibrous hyperplasia tissue, inflammatory cell infiltration, and mucus background in some areas [Figure 3(a) and (b)]. Immunohistochemical staining results were as follows: S-100(+), CD68(+), CD163(+), Ki-67(+, 1%), CD31 (+, vessel), CD34 (+, vessel); The special staining result was as follows: AB(+) [Figure 3(c) and (d)]. In addition, this patient did not take any special treatment except basic anti-inflammatory treatment after surgery.

Bronchoscopy detected a yellowish multilobulated and smooth polypoid tumor located in the right B4a (a), and it was resected by endoscope bandaging and cryosurgery (b and c).
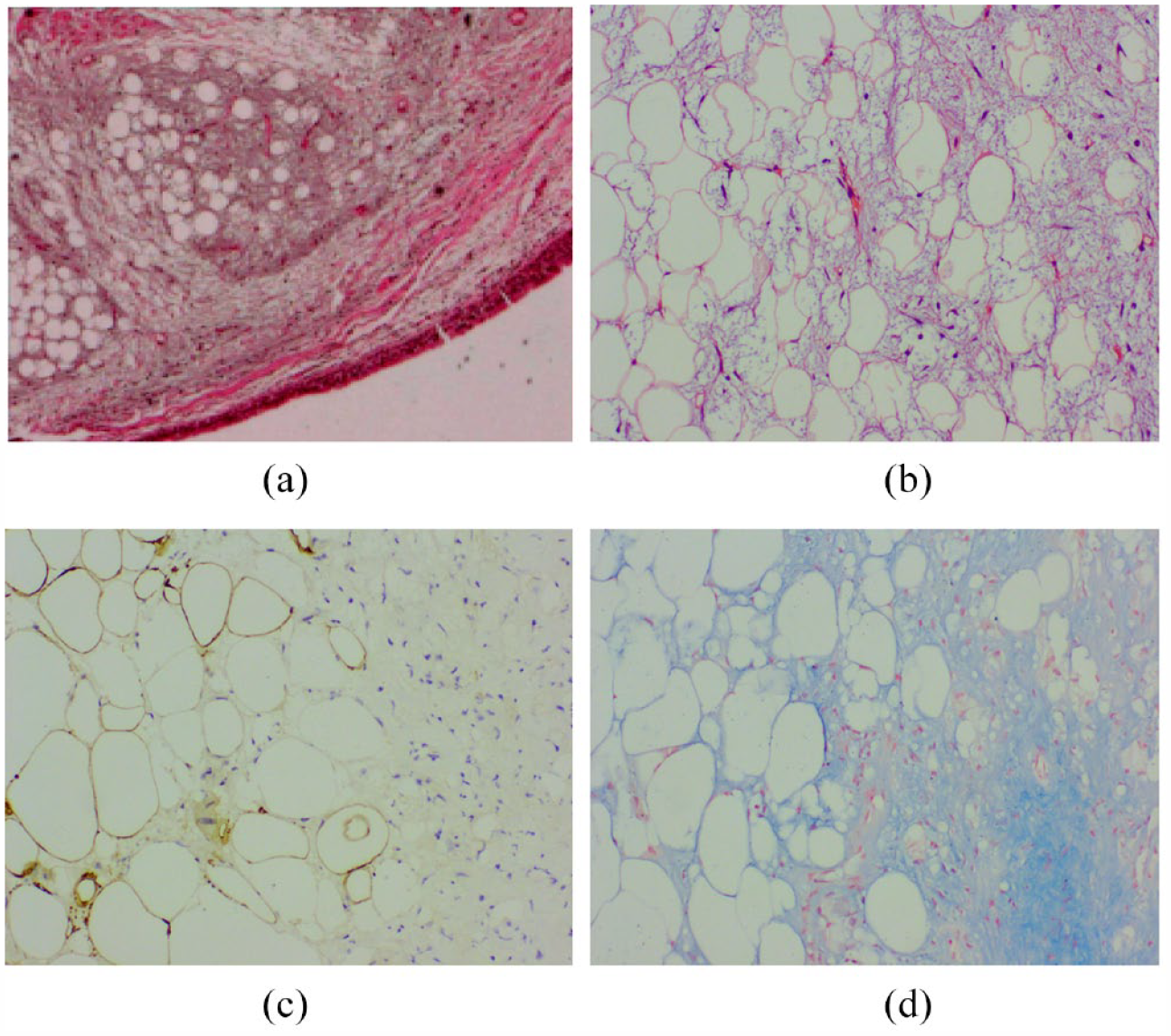
Histopathology revealed a large amount of mature adipose tissue accompanied by focal fibrous hyperplasia tissue, inflammatory cell infiltration, and mucus background (HE ×10, a; HE ×100, b). Immunohistochemical staining results (S-100 ×100, c). The results of special staining are displayed. The mucoid degeneration zone is blue (AB ×100, d).
After 4 months of follow-up, we observed that the B6b solid nodule in the right lower lobe was significantly enlarged (from 5 to 12 mm in size) [Figure 4(a) and (c)] and the lipoma reappeared at the original location [Figure 4(b)]. One week later, the solid nodule of B6b was surgically removed and histopathologically examined. Histopathologic evaluation showed that the nodule was a moderately differentiated squamous cell carcinoma (SCC). Immunohistochemical staining and monoclonal antibodies evaluation were as follows: CK7(+), TTF-1(−), NapsinA(−), CK5/6(+), P63(+), P40(+), CD56(−), CD68(−), P53(−), Ki-67(+, 50%), and ALK(1A4)(−). Incisal margin and all lymph nodes were negative (T1aN0M0), and there was no postoperative chemotherapy.

Atelectasis basically disappeared (red ↑, a). Endobronchial lipoma was recurrent (↑, b). The solid nodule in the right B6b was significantly enlarged (white ↑, a, c). CT showed the reappeared lipoma with slow enlargement (↑, d) and a pathologically confirmed metastatic nodule in the right chest wall (↑, e) during the 29 month follow-up. The solid nodule was pathologically proven to be SCC by puncture biopsies (HE×100, f).
At the follow-up of 29 months, the recurrent lipoma slowly increased in size [Figure 4(d)] and the extent of emphysema gradually increased, but more unfortunately, metastasis occurred in the right chest wall [Figure 4(e)], which was confirmed as SCC by needle biopsy [Figure 4(f)]. After that, we performed radical radiotherapy for the SCC that metastasized to the right pleura, and at 2 months of follow-up, the lesion shrunk considerably but developed extensive radiation pneumonitis around the metastatic lesion. With termly radiotherapy, the radiation pneumonitis was gradually absorbed, and the patient’s symptoms were significantly improved (Supplemental Figures S1–S3). Figure 5 shows the diagnosis, treatment and prognosis evolution of the lesion in detail.

The diagram shows the diagnosis, treatment and prognosis evolution of endobronchial lipoma with SCC in this case.
Discussion
Endobronchial lipoma is an extremely rare benign lung tumor, accounting for 0.1–0.5% of all lung tumors.7,8 Endobronchial lipomas occur predominately in men aged 50–80 years old, but rarely in women.1–5,7–10 Clinical symptoms in the vast majority of patients include cough, expectoration, hemoptysis, asthma, fever, and dyspnea, but there is no typical symptom.1,9,10 It is well known that smoking and obesity are risk factors, but neither of these factors is found in our patient. 9 However, our patient had a history of hypertension and diabetes, which has also been reported in three articles. As to whether their clinical value is related to endobronchial lipoma, it needs to be confirmed by further research.10–14
Endobronchial lipoma is very rare and has no specific clinical symptom. It can be easily missed or misdiagnosed as pneumonia, atelectasis, or chronic obstructive pulmonary disease by conventional X-ray examination. It usually takes several years to make a definite diagnosis, which may bring heavy burden to patients’ physical and mental health. Besides, most of the laboratory tests are negative, and only a few hs-CRP may be elevated.15,16 Moreover, the pulmonary function tests often detect mild-to-moderate respiratory dysfunction, no matter whether the patient has obstructive pneumonia, atelectasis, or emphysema.10,17
Endobronchial lipoma usually appears as a yellowish, smooth, or multilobulated polypoid mass obstructing the trachea or bronchi.14,16–18 As a commonly used medical device, bronchoscopy can be used not only for the observation of bronchial lesions, biopsy sampling, and cytological examination but also for polypectomy and other in vivo surgery. However, this examination is invasive and occasionally difficult to make a definite diagnosis because of insufficient samples. In addition, some tumors are difficult to be completely removed because of their invasion into the deep bronchus or their lager size.
With high sensitivity and specificity, CT is an ideal tool for the diagnosis of endobronchial lipoma, but it may be misdiagnosed as asthma or infection when the tumor is small. For tumors that are lager, surrounding inflammation or atelectasis should not interfere with the radiologist’s ability to detect gross fat in these lesions. However, the presence of mucous pneumonia may obscure lesions of variable size, although this should be a very rare clinical situation. Endobronchial lipomas are usually solitary and possess a very low CT attenuation value (range: −50 to −150 HU). 19 They are predominantly located in the lower lobes of both lungs and the upper right lung and are extremely rare in the right middle lung. It may be a completely solitary tumor or accompanied by pneumonia, atelectasis, aspergillosis, emphysema, and bronchiectasis.1,10–13,20,21 There is no calcification and soft tissue components in this tumor, which is significantly different from that of the fat-containing hamartoma.
Endobronchial lipoma is a benign tumor that can coexist with other lung diseases such as pulmonary tuberculosis and lung cancer, but such occurrence is relatively rare.1–4,15 At present, only seven cases of bronchial lipoma coexisting with lung cancer (including this case) have been reported, six cases of which were SCC, and only one case was adenocarcinoma, and all of them were male.1–4 Relative to the other six cases (ages ranged from 64 to 82 years), the patient in our case is the youngest, and the similar cases have two common features – male predominance and poor prognosis (Table 1).1–4 Moreover, the other six cases did not provide imaging data, only written records. This phenomenon should be scrutinized carefully that four of five patients with SCC died, and one patient developed metastasis during 3-year follow-up; it may be related to the abnormal proliferation of the squamous epithelial cells of bronchial mucosa stimulated by the growth of lipoma. Therefore, we suggest that patients with these conditions should take more active treatment measures after surgery.
Clinicopathologic features of seven cases of endobronchial lipoma complicated with lung carcinoma.
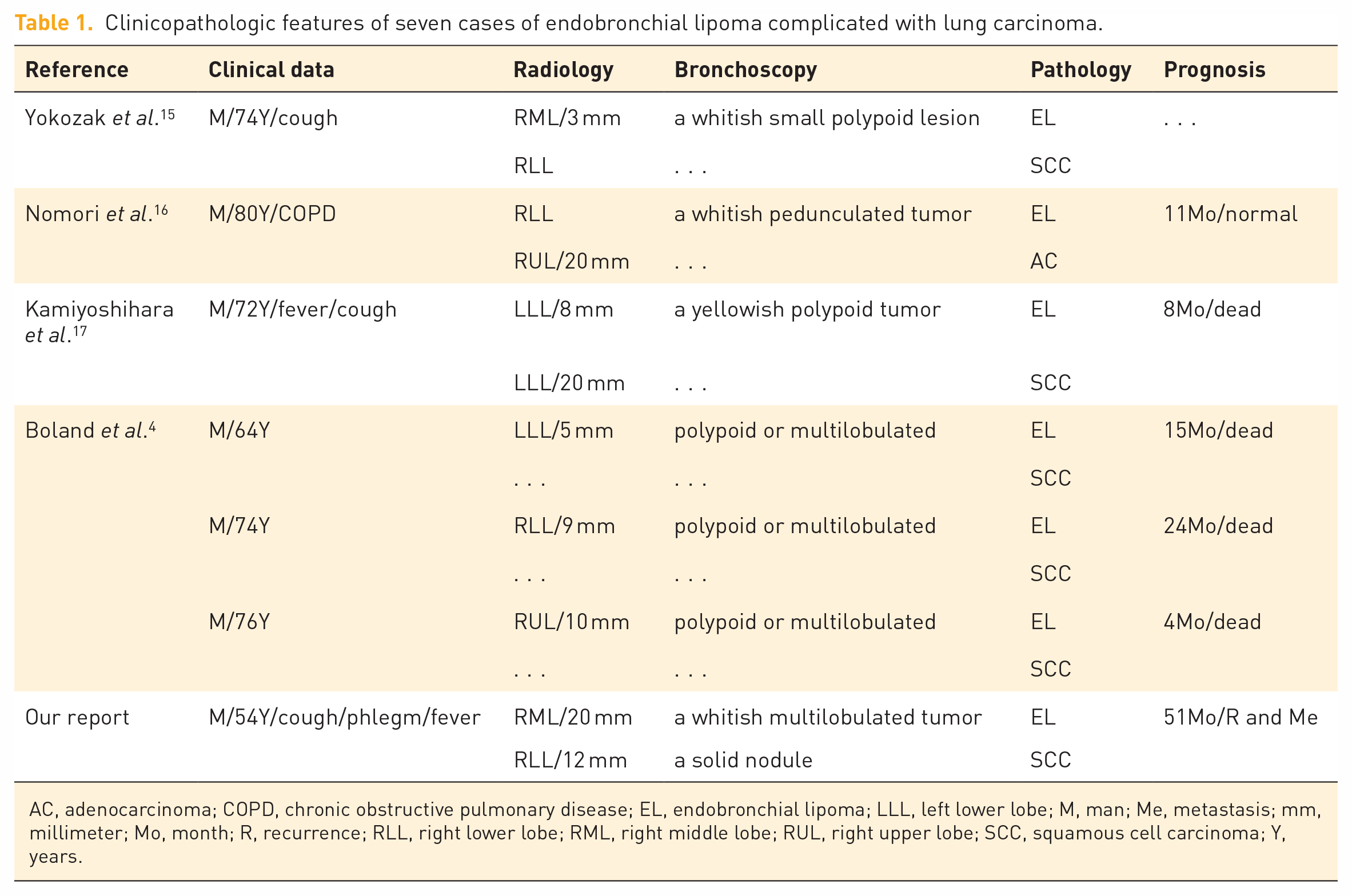
AC, adenocarcinoma; COPD, chronic obstructive pulmonary disease; EL, endobronchial lipoma; LLL, left lower lobe; M, man; Me, metastasis; mm, millimeter; Mo, month; R, recurrence; RLL, right lower lobe; RML, right middle lobe; RUL, right upper lobe; SCC, squamous cell carcinoma; Y, years.
For endobronchial lipoma, bronchoscopy is not only a method of examination but also a means of treatment. It is widely used in clinical treatment because it is less traumatic than other treatments. We recommend bronchoscopy as the first choice of surgical treatment for patients without severe obstructive pneumonia and atelectasis because peripheral obstructive changes in lipoma may affect the effect of endoscopic resection, as indicated by the reappeared lipoma in the previous location of this case. After nearly 3 years of follow-up, the volume of the reappeared lipoma increased at a very slow rate, indicating that the previous lipoma had not been completely resected, rather than a recurrence. Alazemi et al. reported a recurrence of endobronchial lipoma at first time in 2010. 5 Pathologically, multilobulated polypoid tumors are uncommon. In this case report, regarding the reasons for the recurrence of the bronchial mucous lipoma in the middle lobe of the right lung due to incomplete resection, we have the following hypotheses: First, the choice of surgical method may be unreasonable, and the resection range is not large enough. Second, the lipoma is irregular and multilobulated, with a large volume, and the peritumor was rich in inflammatory cells and a large amount of mucus components. These factors would affect the exposure of the operating field during bronchoscopy, making the field of vision blurred, causing the operation more difficult for the surgeon, and not conducive to the complete resection of the tumor tissue.
On pathological tissue specimen, endobronchial lipoma manifests like a yellow or yellowish, smooth or multilobulated polypoid mass. Histopathological studies show that the lipoma contains a large number of mature adipocytes, fibrous tissue or surrounded by fibrous tissue; the fibrolipoma consists of fibrous tissue, adipose tissue, and mucous tissue; and the hamartoma has the adipose tissue with a little of microcalcification. It is worth mentioning that in addition to pure lipoma, there is a specific type of endobronchial lipomas, the fibrous type. Due to a large amount of mucus component in this case, whether the presence of mucinous type of lipoma remains to be investigated and reported. For limitations, although the coexistence of bronchial lipoma and lung cancer is rare and not critical in most cases, further research on its pathogenesis, risk factors and optimal management is needed. In addition, accumulating more similar cases is necessary for clinicians and radiologists to improve their understanding of the disease and evaluate its prognosis.
Conclusion
Endobronchial lipoma is a rare benign tumor. It can easily be misdiagnosed if the tumor is small or obscured by other low attenuation lesions. Endoscopic mucosal resection is a safe and effective method, but it should be chosen with great caution for high-risk patients (lesions with severe obstructive atelectasis or multilobulated polypoid or large volume). Furthermore, when there is accompanied with SCC, postoperative radiotherapy and chemotherapy should be actively performed.
Supplemental Material
sj-png-1-tar-10.1177_17534666231208575 – Supplemental material for An unexpected encounter and outcome between endobronchial lipoma and carcinoma: a case report and literature review
Supplemental material, sj-png-1-tar-10.1177_17534666231208575 for An unexpected encounter and outcome between endobronchial lipoma and carcinoma: a case report and literature review by Yang Yang, Jun Liu, Songkuan Chen, Guangzhao Yang, Guoqun Mao, Xiaoyu Han and Jian Wang in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-png-2-tar-10.1177_17534666231208575 – Supplemental material for An unexpected encounter and outcome between endobronchial lipoma and carcinoma: a case report and literature review
Supplemental material, sj-png-2-tar-10.1177_17534666231208575 for An unexpected encounter and outcome between endobronchial lipoma and carcinoma: a case report and literature review by Yang Yang, Jun Liu, Songkuan Chen, Guangzhao Yang, Guoqun Mao, Xiaoyu Han and Jian Wang in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-png-3-tar-10.1177_17534666231208575 – Supplemental material for An unexpected encounter and outcome between endobronchial lipoma and carcinoma: a case report and literature review
Supplemental material, sj-png-3-tar-10.1177_17534666231208575 for An unexpected encounter and outcome between endobronchial lipoma and carcinoma: a case report and literature review by Yang Yang, Jun Liu, Songkuan Chen, Guangzhao Yang, Guoqun Mao, Xiaoyu Han and Jian Wang in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.