
Abstract
Background:
Chronic obstructive pulmonary disease (COPD) management in China is inadequate and there is a need to improve care and outcomes for patients nationwide.
Objectives:
The REAL study was designed to generate reliable information on COPD management from a representative sample of Chinese patients with COPD. Here, we present study outcomes related to acute exacerbations.
Design:
A 52-week, multicentre, prospective, observational study.
Methods:
Outpatients (aged ⩾ 40 years) enrolled from 25 tertiary and 25 secondary hospitals across six geographic regions in China were followed for 12 months. Risk factors for COPD exacerbation and disease severity by exacerbation were assessed using multivariate Poisson and ordinal logistic regression models, respectively.
Results:
Between June 2017 and January 2019, 5013 patients were enrolled, with 4978 included in the analysis. Mean (standard deviation) age was 66.2 (8.9) years. More patients presented with exacerbations in secondary versus tertiary hospitals (59.4% versus 40.2%) and in rural versus urban areas (53.2% versus 46.3%). Overall exacerbation rates differed across regions (range: 0.27–0.84). Patients from secondary versus tertiary hospitals had higher rates of overall exacerbation (0.66 versus 0.47), severe exacerbation (0.44 versus 0.18) and exacerbation that resulted in hospitalisation (0.41 versus 0.16). Across regions and hospital tiers, the rates of overall exacerbation and exacerbations that resulted in hospitalisation were highest in patients with very severe COPD (based on the severity of airflow limitation or GOLD 2017 combined assessment). Strong predictors of exacerbation included demographic and clinical characteristics, modified Medical Research Council scores, mucus purulence, exacerbation history and the use of maintenance mucolytic treatment.
Conclusion:
COPD exacerbation rates varied across regions and were higher in secondary compared with tertiary hospitals in China. Understanding the factors associated with COPD exacerbation may facilitate improved management of COPD exacerbations in China.
Registration:
The trial was registered on 20 March 2017 (ClinicalTrials.gov: NCT03131362; https://clinicaltrials.gov/ct2/show/NCT03131362).
Plain language summary
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is characterised by airflow limitation and chronic respiratory symptoms, 1 and is one of the leading causes of morbidity and mortality globally. 2 In China, COPD is one of the top five leading causes of mortality and disability-adjusted life-years, with a mortality rate of 68 per 100,000 individuals. 3 In 2015, it was estimated that 100 million people in China (13.7% of adults aged ⩾ 40 years) had COPD. 4 COPD exacerbations are part of the natural course of the disease and characterised by acute worsening of respiratory symptoms that may result in additional therapy.1,5 They are one of the greatest risk factors for increased mortality in patients with COPD, and decline in lung function and impaired quality of life. 6 In China, patients with COPD experience 0.5–3.5 episodes of exacerbations annually, 7 with mean per capita expenditure for the treatment of exacerbations increasing from US$3472 to US$4538 between 2009 and 2017. 8 In the REALising and improving management of stable COPD in China (REAL) study (NCT03131362), the annual rate of COPD exacerbations per patient was 0.56 [95% confidence interval (CI): 0.54–0.58]. 9 To improve disease prognosis, better management of COPD exacerbations is crucial. 10 The Chinese Thoracic Society 11 recommends that physicians use the Global Initiative for Chronic Obstructive Lung Disease (GOLD) evidence-based strategy document guidelines for the management of COPD and COPD exacerbations. 1 However, adherence to the guidelines appears to be poor in real-world clinical practice in China.9,12–14
China comprises multiple geographic regions (each consisting of both urban and rural areas) and a three-tier healthcare system; 13 it is important to characterise the clinical outcomes of patients with COPD at the regional and institutional level. There was a substantial lack of large-scale, real-world studies on COPD management across China at the time of study initiation. The REAL study was a 52-week, multicentre, prospective, observational study designed to gather reliable information on COPD management, clinical outcomes and risk factors from a representative sample of patients with COPD in China. 15 Baseline 13 and primary outcomes 9 have been previously reported, as have treatment patterns in patients with stable COPD by geographic region and hospital tier. 14 Here, we report exploratory outcomes and post hoc analyses relating to acute exacerbations in the REAL study.
Methods
Study design and population
The REAL study protocol has been previously published. 15 Between June 2017 and January 2019, patients (male and female) were consecutively screened and enrolled during routine clinical visits at 50 hospitals (25 tertiary and 25 secondary) across six geographic regions in China. A multi-stage, stratified, cluster sampling method was used to select these hospitals as a nationally representative population. Eligible patients were outpatients aged ⩾ 40 years, clinically diagnosed with COPD [based on the presence of chronic cough, sputum, wheeze, a history of exposure to harmful factors and confirmed spirometry post-bronchodilator forced expiratory volume in 1 s (FEV1)/forced vital capacity < 0.7 as per GOLD 2016 criteria], who provided informed consent. Exclusion criteria included participation in any interventional trials (within 30 days prior to enrolment) and occurrence of acute exacerbation of COPD (within 4 weeks prior to enrolment).
Data collection
Patients were followed for 12 months with two prespecified onsite visits [at baseline (V0) and end of the study (V1)] and a telephone contact (TC) follow-up every 3 months after V0 (TC1–3). At V0, baseline and demographic data were collected. At V0, V1, and TC1–3, data for symptoms, comorbidities, complications and exacerbations were collected, and patient-reported outcome questionnaires were completed by the patients before performing other procedures. Spirometry, chest computed tomography imaging, induced sputum and laboratory test data were collected if available. All data were collected using case report forms. The assessment of disease severity has been previously described. 15
Outcomes
The primary objective was to evaluate the 1-year clinical outcomes of patients with COPD in current clinical practice in China. Exploratory outcomes addressed here include exacerbations by geographic region, hospital tier and residence area, and risk factors for COPD exacerbation. Mild exacerbations were defined as those requiring an increase in rescue medication ⩾ 3 puffs/day for ⩾ 2 consecutive days; moderate exacerbations were those requiring systemic glucocorticosteroids and/or antibiotics; severe exacerbations were those requiring hospitalisation or emergency room visit, or if leading to death.
Statistical analysis
Statistical analysis was performed on the full analysis set (FAS), which included all enrolled patients who fulfilled eligibility criteria. Sample size calculation has been published previously. 15 Data analysis was primarily descriptive in nature. For continuous variables, mean, median, standard deviation (SD) and range were calculated. For categorical variables, frequency counts and percentages were calculated. Annual exacerbation rates and corresponding 95% CI were estimated using the Poisson distribution model. Weighted summaries of annual exacerbation rates were estimated using the proportions of the region/site and total populations (if applicable) to minimise any regional/site bias. 15 Risk factors for exacerbations were analysed using univariate and multivariate Poisson regression models, and risk factors for disease severity by exacerbations were analysed using ordinal logistic regression models. Data were presented as relative risk (RR) and odds ratio (OR), with the corresponding 95% CI. Variables achieving a p-value of less than 0.15 in the univariate model were entered into the multivariate model; stepwise regression was used to construct the final multivariable model with an inclusion threshold of p-value less than 0.05. Patients lost to follow-up were withdrawn from the study and reasons for withdrawal or discontinuation were determined. There was no imputation of missing data; all statistical analyses were carried out on non-missing data only. Statistical analysis was performed using Statistical Analysis System version 9.4.
Results
Patient demographics and baseline characteristics
Between 30 June 2017 and 29 January 2019, 5097 patients were screened, of whom 5013 were enrolled and 4978 were included in the FAS. A total of 772 patients withdrew from the study; reasons for study withdrawal included loss to follow-up (n = 565), withdrawal of consent (n = 117), death (n = 58) or other reasons (n = 32). At TC1, TC2, TC3 and the V1 visit, 308 (6.2%), 423 (8.5%), 505 (10.1%) and 739 (14.8%) patients, respectively, dropped out of the study.
Baseline patient demographics and characteristics for the overall population have been previously reported. 13 Mean ± SD age was 66.2 ± 8.9 years, and most patients were male (79.5%). Mean ± SD time since COPD diagnosis was 3.8 ± 6.2 years. Patients were almost equally sampled from urban and rural areas and from secondary and tertiary hospital tiers. There were more patients sampled from the east (25.1%) and north (20.2%) regions compared with other regions (range: 12.0–18.2%). Respiratory symptoms at baseline were shortness of breath (57.6%), wheezing (66.3%), chest tightness (66.8%), cough (81.1%) and purulent mucus (80.6%). According to disease severity assessed by airflow limitation, 10.1%, 41.7%, 34.5% and 13.6% of patients had mild, moderate, severe and very severe disease, respectively. Per GOLD 2016 combined assessment, 11.4%, 22.0%, 12.0% and 54.6% of patients were in groups A, B, C and D, respectively, while per GOLD 2017 combined assessment, 16.4%, 41.9%, 7.3% and 34.4% of patients were in the corresponding groups (Table 1). A greater proportion of patients from secondary versus tertiary hospitals (59.4% versus 40.2%) and rural versus urban area (53.2% versus 46.3%) experienced exacerbations in the previous 12 months. Mean ± SD number of exacerbations in the previous 12 months was 0.8 ± 1.56 in tertiary hospitals, 1.1 ± 1.38 in secondary hospitals, 0.9 ± 1.41 in urban areas and 1.0 ± 1.56 in rural areas (Table 2).
Patient demographics and baseline characteristics.

BMI, body mass index; COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; SD, standard deviation.
Missing data: n = 6 for tertiary hospitals in the north.
Missing data: n = 3.
Exacerbations in the previous 12 months by hospital tier and residence area.
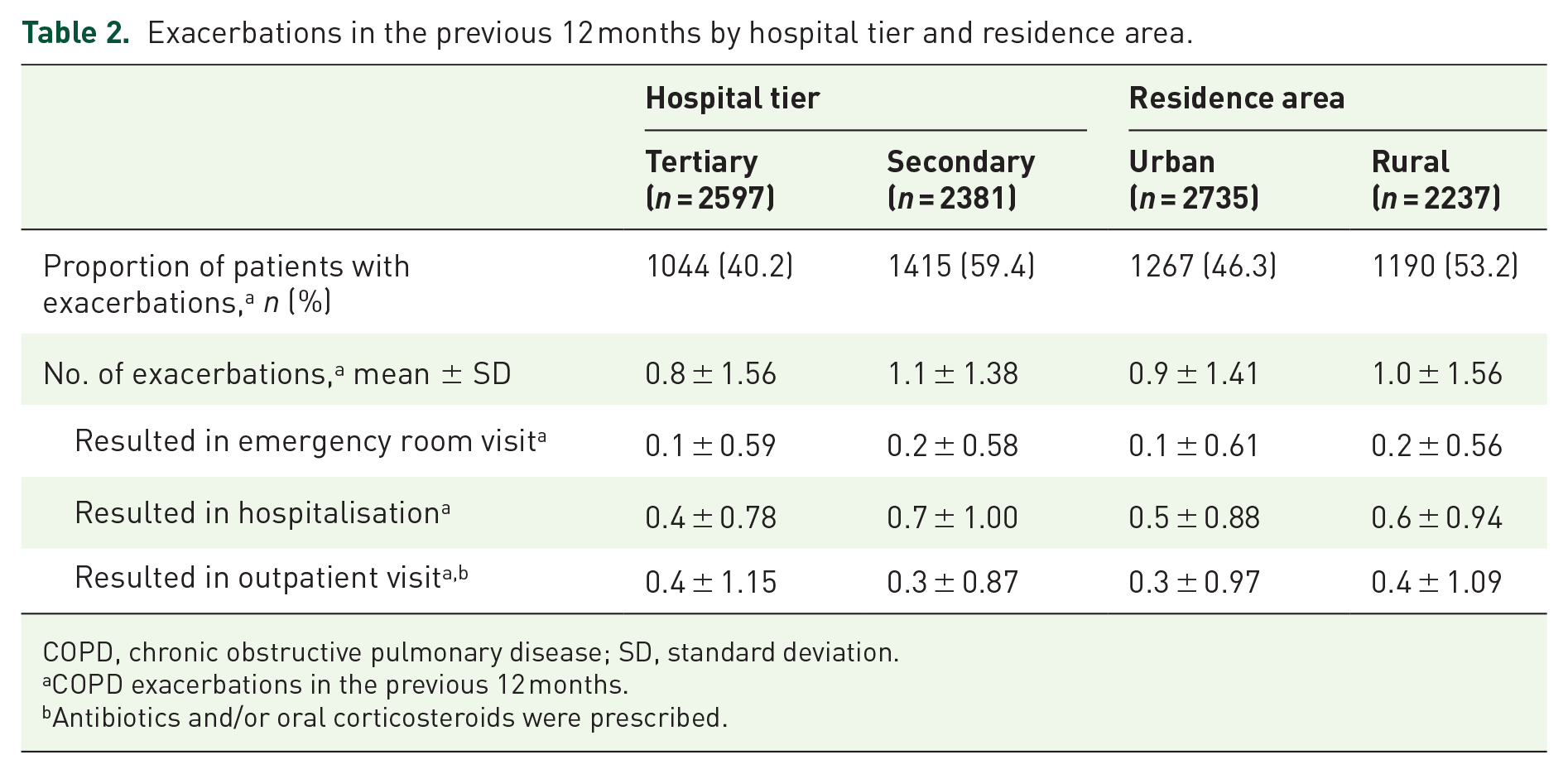
COPD, chronic obstructive pulmonary disease; SD, standard deviation.
COPD exacerbations in the previous 12 months.
Antibiotics and/or oral corticosteroids were prescribed.
COPD exacerbation across geographic regions, hospital tiers and residence areas
Annual exacerbation rates across geographic regions, hospital tiers and residence areas are summarised in Table 3. Across geographic regions, moderate, severe and overall exacerbation rates ranged 0.01–0.35, 0.13–0.45 and 0.27–0.84, respectively. Overall exacerbation rate was highest in the south-central region (0.84, 95% CI: 0.78–0.90), where both moderate (0.35, 95% CI: 0.31–0.39) and severe (0.41, 95% CI: 0.37–0.45) exacerbation rates were high. Overall exacerbation rate was lowest in the north (0.27, 95% CI: 0.24–0.31), where both moderate (0.04, 95% CI: 0.03–0.05) and severe (0.13, 95% CI: 0.11–0.16) exacerbation rates were low. In general, approximately half of overall exacerbations in most regions were severe, except in the northwest region, where most exacerbations were severe (overall exacerbation: 0.47; severe exacerbation: 0.45). A substantial proportion of exacerbations was severe across the two hospital tiers, although rates for both overall and severe exacerbations were higher in secondary versus tertiary hospitals (overall: 0.66 versus 0.47; severe: 0.44 versus 0.18). Similarly, a substantial proportion of exacerbations was severe across both rural and urban areas, with severe exacerbation rates of 0.30 and 0.32, respectively. Annual exacerbation rates were highest in patients with very severe COPD (based on the severity of airflow limitation or GOLD 2017 combined assessment) across different geographic regions and hospital tiers (Table 4).
Annual exacerbation rate by geographic region, hospital tier and residence area.

CI, confidence interval.
Rate and CI are estimated using the Poisson distribution model.
Annual exacerbation rate by disease severity by geographic region and hospital tier.

CI, confidence interval; GOLD, Global Initiative for Chronic Obstructive Lung Disease.
Rate of exacerbation that resulted in hospitalisation was the highest in the northwest region (0.45, 95% CI: 0.40–0.51) and lowest in the north (0.12, 95% CI: 0.10–0.14). Rates of exacerbation that resulted in hospitalisation were 0.41 and 0.16 in secondary and tertiary hospitals, respectively, and 0.29 and 0.27 in rural and urban areas, respectively (Table 3). Rates of exacerbations that resulted in hospitalisation were highest in patients with very severe COPD (based on the severity of airflow limitation or GOLD 2017 combined assessment) across different geographic regions and hospital tiers (Table 5).
Annual rate of exacerbation that resulted in hospitalisation by disease severity, by geographic region and hospital tier.

CI, confidence interval; GOLD, Global Initiative for Chronic Obstructive Lung Disease.
A substantial proportion of patients experienced respiratory symptoms due to COPD exacerbation regardless of exacerbation severity. Cough (range: 90.4–95.4%) and mucus purulence (range: 88.5–93.1%) were the most common symptoms across the mild, moderate and severe exacerbation groups (Supplementary Table S1).
Risk factors for COPD exacerbation
To identify patient variables that may predict risk of future exacerbations, we performed an exploratory analysis of factors associated with COPD exacerbations in the REAL study. Two univariate analysis models were constructed, one for lung function and laboratory tests and vaccination related to COPD, and another for demographic and clinical characteristics, lung function tests, questionnaire scores, symptoms, maintenance medications and exacerbations in the previous 12 months.
In the first univariate model, several lung function and laboratory tests showed a predictive trend for exacerbation (Supplementary Table S2), but these factors were not incorporated into the multivariate model due to substantial missing values or unsuitability for multivariate regression.
In the second univariate model, the following factors were entered into the multivariate model based on the cut-off value p < 0.15 (Supplementary Table S3): demographic and clinical characteristics [age, sex, heart rate, body mass index (BMI), smoking status, comorbidities or complications], lung function tests (FEV1% predicted, FEV1, peak expiratory flow, airway limitation, bronchodilator reversibility test), questionnaire scores [COPD assessment test (CAT) total score, modified Medical Research Council (mMRC) score], symptoms (shortness of breath, cough, and mucus purulence), COPD maintenance medication (mucolytics) and exacerbations in the previous 12 months.
Factors retained in the multivariate Poisson regression model (Table 6) were heart rate (RR = 1.41, p < 0.001), mMRC score (RR = 1.33, p = 0.002), mucus purulence (RR = 1.61, p < 0.001), maintenance mucolytic treatment (RR = 4.22, p = 0.002) and exacerbation in the previous 12 months (RR = 2.66, p < 0.001).
Multivariate analysis of risk factors for COPD exacerbation.

CI, confidence interval; COPD, chronic obstructive pulmonary disease; mMRC, modified Medical Research Council; RR, relative risk.
Risk factors for disease severity by exacerbations
Similar analyses were conducted to identify patient variables that may predict disease severity by exacerbation (defined by 0, 1 or ⩾ 2 exacerbations). In the first univariate model, several lung function and laboratory tests, exacerbation history and smoking status showed a predictive trend for disease severity by exacerbation (Supplementary Table S4), but these factors were not incorporated into the multivariate model due to substantial missing values or unsuitability for multivariate regression.
In the second univariate model, the following factors were entered into the multivariate model based on the cut-off value p < 0.15 (Supplementary Table S5): demographic and clinical characteristics (age, sex, heart rate, BMI, smoking status, comorbidities or complications), lung function tests (FEV1% predicted, FEV1 peak expiratory flow, airway limitation, bronchodilator reversibility test), questionnaire scores (CAT total score, mMRC score), symptoms (shortness of breath, wheezing, cough, mucus purulence), mucolytic maintenance treatment and exacerbations in the previous 12 months.
Factors retained in the multivariate regression model (Table 7) were mMRC score (OR = 1.54, p = 0.003), mucus purulence (OR = 1.85, p < 0.001) and exacerbation in the previous 12 months (OR = 2.77, p < 0.001).
Multivariate analysis of risk factors for disease severity by exacerbation.

CI, confidence interval; mMRC, modified Medical Research Council; OR, odds ratio.
We also performed a post hoc univariate analysis to understand the association between factors related to exacerbations in the previous year and exacerbation severity (Supplementary Table S6). Factors showing a predictive trend for increased risk of moderate, severe and overall exacerbations (all p < 0.05) were having ⩾ 1 exacerbation(s) in the previous year that led to outpatient treatment, emergency room visit or hospitalisation; having ⩾ 2 exacerbations in the previous year (including those that led to hospitalisation) and having ⩾ 3 exacerbations in the previous year (including those that led to hospitalisation).
Discussion
REAL is the first nationwide study to collect prospective longitudinal real-world data on the management and clinical outcomes of a large cohort of outpatients with COPD in China. Overall, we observed substantial differences in COPD exacerbation rates across regions and hospital tiers, and additionally reported exploratory and post hoc analyses of the risk factors that may help predict future acute exacerbations.
There is substantial burden of severe exacerbation across hospital tiers and residence areas, with high rates of severe exacerbation (up to 0.44) and exacerbations that resulted in hospitalisation (up to 0.41). We have previously reported a substantial burden of severe exacerbation in the overall study population (more than half of overall exacerbations were severe). 9 Previous large retrospective studies have reported that 42.6–49.8% of patients with COPD had exacerbations annually, with up to 25% of patients experiencing severe exacerbations that resulted in hospitalisation.16,17 Across studies conducted in different countries, severe exacerbation rates ranged from 0.3 to 1.4,16–19 while in the ECLIPSE study, the rate of exacerbation that resulted in hospitalisation was 0.22. 20
The proportion of patients with exacerbations in the previous 12 months, and rates of overall exacerbation and exacerbation that resulted in hospitalisation were higher in secondary hospitals compared with tertiary hospitals, which is likely due to the higher annual rate of severe exacerbations in secondary hospitals. Final outcomes of the REAL study revealed that disease severity is positively correlated with annual exacerbation rate. 9 In addition, we found that patients with severe/very severe COPD had higher exacerbation rates and rates of exacerbation that resulted in hospitalisation than those with mild/moderate COPD regardless of hospital tier. Similarly, in the ECLIPSE study, exacerbations became more frequent and severe (i.e. requiring hospitalisation) as the severity of COPD increased. 20 We have previously reported that secondary hospitals had a greater proportion of patients with very severe COPD compared with tertiary hospitals, 14 which may have contributed to the differences in exacerbation rates across hospital tiers.
Disparities in the level of respiratory care and expertise between different hospital tiers (77.8% of tertiary hospitals and 38.8% of secondary hospitals have independent respiratory departments) 21 may impact COPD management and, thus, the rate of exacerbations. In addition, differences in medical coverage policies may have also contributed to the observed differences in exacerbation rates across hospital tiers. Not all patients are eligible for medical reimbursements in China (e.g. immigrants who have left their hometown). 22 At the time of the study, COPD was not included in the scope of outpatient medical reimbursement in all regions of China. 23 The lack of reimbursement has been shown to be associated with increased hospitalisation costs, 22 which in turn may deter patients from seeking treatment, promoting disease progression.
Differences in the distribution of hospitals across rural and urban areas may have also contributed to the difference in exacerbation rates. We have reported that the majority of patients at secondary hospitals in the REAL study were from rural areas, whereas patients at tertiary hospitals were more frequently from urban areas. 14 Patients from rural areas have limited disease awareness, reported lower medication use and are less likely to seek medical advice despite a higher proportion of them reporting more severe conditions compared with patients from urban areas. 24 Other studies have shown that patients from rural areas experience greater COPD burden (including hospitalisation, disability and worsened health).25,26 Our analysis showed that patients from rural areas had higher rates of exacerbation that led to hospitalisation despite having slightly lower exacerbation rates compared with those from urban areas. This may reflect poorer disease awareness and management in rural compared with urban areas.
Given the potential impact of residence area (rural versus urban) on disease burden, this may also partly explain the difference in exacerbation rates observed across geographic regions in China. In the REAL study, the northwest region had the highest proportion of rural residents (64.6%) 14 and also the highest rate of exacerbation that resulted in hospitalisation, while the north and east were among regions with the highest proportion of urban residents (59.9–62.0%) 14 and with the lowest rate of exacerbation that resulted in hospitalisation. The lack of high-level medical institutions in rural areas may limit access to specialist medical services and optimal COPD management. 27 As such, patients residing in rural areas may tend to postpone or forego seeking treatment from respiratory physicians, which in turn may increase the risk of hospitalisation and promote disease progression.28,29 In contrast, regions with more developed economies have higher local fiscal revenue to invest in health and medical resources, which are therefore more abundant. 30 The lower rate of exacerbation that resulted in hospitalisation in the north could also be a reflection of the fewer patients in that region having severe/very severe COPD at baseline. 14 Across different regions, patients with severe/very severe COPD had higher exacerbation rates than those with mild/moderate COPD. Notably, the south-central region had one of the highest rates of severe and overall exacerbations, despite having a similar proportion of patients with severe/very severe disease compared with other regions. 14 This may be due to the higher proportion of patients who did not receive inhaled corticosteroids or long-acting bronchodilator therapy in the south-central region compared with most other regions. 14 However, due to limited patient numbers across geographic regions in this study, these findings should be interpreted with caution. Additional studies are required to confirm how these factors influence exacerbation rates.
To contribute to wider efforts to improve management of COPD exacerbations, we performed multivariate analyses of potential risk factors associated with COPD exacerbation and disease severity by exacerbation (defined by 0, 1 or ⩾ 2 exacerbations). Strong predictors of COPD exacerbation and disease severity by exacerbation included symptoms (mMRC score and mucus purulence) and exacerbation in the previous 12 months. Other factors that were also strong predictors for COPD exacerbation included patient characteristics (heart rate) and maintenance mucolytic treatment. Based on the post hoc univariate analysis, having exacerbations in the previous year increased the risk of overall, moderate and severe exacerbations; having only one exacerbation that led to hospitalisation increased the risk of overall exacerbations, but having only one exacerbation that led to outpatient treatment or emergency room visit did not.
Our findings are consistent with those from the ECLIPSE study, 20 as well as a recent Danish contemporary population-based cohort study, 31 in which airway obstruction, mMRC dyspnoea score ⩾ 2 and having ⩾ 1 exacerbation in the previous year were factors associated with COPD severity (GOLD stage II–IV) and increased risk of subsequent exacerbations. An observational cohort study in Germany revealed that patients who had a severe exacerbation (which resulted in hospitalisation or emergency room visit) or multiple exacerbations (regardless of severity) at baseline experienced more than three times the number of exacerbations during the first 3 years of follow-up, compared with those who had moderate or no exacerbations at baseline. 32 With regard to other variables that we identified as strong predictors of exacerbation, a previous study showed that patients with higher resting heart rate had increased risk of exacerbation, 33 but this was not the case in another study, which demonstrated that resting heart rate is a risk factor for mortality in COPD but not for exacerbations. 34 Mucolytics tend to be prescribed in patients who do not receive inhaled maintenance treatment, which are the mainstay of COPD treatment and are associated with reduced exacerbation. 1 Although mucolytics are potentially useful for COPD management, there is a lack of consensus on the ideal target patient population for their use 1 and a paucity of data comparing the efficacy of different mucolytic agents in reducing the risk of exacerbations. The RESTORE study demonstrated that while erdosteine (a mucolytic agent) reduced overall exacerbation rates, this effect was driven by a reduction in the rate of mild exacerbation (reported by patients on their home symptom diary cards), whereas the rate of moderate/severe exacerbations was 15% higher in the group treated with erdosteine compared with placebo. 35 Based on the univariate analysis in this study, current smokers appear to have a slightly lower risk of exacerbation compared with non-smokers. This may be due to potential confounding effects from other variables (e.g. age, comorbidities, respiratory disease history, medication use) that were not accounted for in the univariate analysis. The patient and disease variables that we identified as strong predictors for COPD exacerbation and disease severity by exacerbation can be collected in routine clinical practice and may facilitate improved management of COPD exacerbations in China, although further research is required to confirm these findings.
An understanding of common symptoms associated with exacerbations may additionally help physicians to diagnose exacerbations and provide patients with timely medical intervention. We found that mucus purulence and cough were the most common symptoms associated with exacerbations, regardless of disease severity. Mucus purulence due to bacterial infections is common during exacerbations. 36 These symptoms are reported in only 30% of patients with stable COPD, 1 but > 85% of patients with exacerbation displayed these symptoms in our study.
Several limitations should be considered when interpreting the results. Only patients who visited the outpatient respiratory department of tertiary and secondary hospitals who were diagnosed with COPD were enrolled into the study; patients with early-stage COPD and with few or mild symptoms were underrepresented. The 2019 coronavirus disease pandemic may have discouraged patients with COPD from presenting to hospital, which may have also contributed to under-reporting of outcomes. Finally, data were confined to examinations and tests performed in routine clinical practice; thus, not all assessment data were available.
Conclusion
There is a substantial burden of severe COPD exacerbation across hospital tiers and residence areas in China. COPD exacerbation rates differed across geographic regions and hospital tiers; patients from rural areas had a slightly higher rate of exacerbation leading to hospitalisation, which likely reflects reduced disease awareness and poorer management. Our findings highlight that there is a need to improve clinical care, particularly in secondary hospitals and for rural patients. We identified several patients and disease factors that had a strong predictive trend for COPD exacerbation, such as symptoms and exacerbation in the previous 12 months, which may facilitate improved management of COPD exacerbations in China in the future.
Supplemental Material
sj-docx-1-tar-10.1177_17534666231167353 – Supplemental material for Exacerbation in patients with stable COPD in China: analysis of a prospective, 52-week, nationwide, observational cohort study (REAL)
Supplemental material, sj-docx-1-tar-10.1177_17534666231167353 for Exacerbation in patients with stable COPD in China: analysis of a prospective, 52-week, nationwide, observational cohort study (REAL) by Ting Yang, Baiqiang Cai, Bin Cao, Jian Kang, Fuqiang Wen, Yahong Chen, Wenhua Jian and Chen Wang in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
Editorial assistance was provided by Liting Hang BSc (Hons), PhD and Alice Carruthers BSc (Hons), PhD of Nucleus Global Asia Pacific, which was funded by AstraZeneca China in accordance with Good Publication Practice (GPP3) guidelines.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.