
Abstract
Background:
Underdiagnosis and undertreatment pose major barriers to optimal management of chronic obstructive pulmonary disease (COPD) in China.
Objective:
The REAL trial was performed to generate reliable information on real-world COPD management, outcomes and risk factors among Chinese patients. Here, we present study outcomes related to COPD management.
Design:
It is a 52-week, prospective, observational, multicentre study.
Methods:
Outpatients (aged ⩾40 years) enrolled from 50 secondary and tertiary hospitals across six geographic regions of China were followed up for 12 months, with two onsite visits and by telephone every 3 months following baseline.
Results:
Between June 2017 and January 2019, 5013 patients were enrolled and 4978 included in the analysis. Mean [standard deviation (SD)] age was 66.2 (8.9) years, the majority of patients were male (79.5%) and mean (SD) time since COPD diagnosis was 3.8 (6.2) years. The most common treatments at each study visit were inhaled corticosteroids/long-acting beta-agonists (ICSs/LABAs; 28.3–36.0%), long-acting muscarinic antagonists (LAMAs; 13.0–16.2%) and ICS/LABA + LAMA (17.5–18.7%), but up to 15.8% of patients at each visit received neither ICS nor long-acting bronchodilators. The use of ICS/LABA, LAMA and ICS/LABA + LAMA differed across regions and hospital tiers; up to fivefold, more patients received neither ICS nor long-acting bronchodilators in secondary (17.3–25.4%) versus tertiary hospitals (5.0–5.3%). Overall, rates of nonpharmacological management were low. Direct treatment costs increased with disease severity, but the proportion of direct treatment costs incurred due to maintenance treatment decreased with disease severity.
Conclusion:
ICS/LABA, LAMA and ICS/LABA + LAMA were the most frequently prescribed maintenance treatments for patients with stable COPD in China, although their use differed between region and hospital tier. There is a clear need for improved COPD management across China, particularly in secondary hospitals.
Registration:
The trial was registered on 20 March 2017 (ClinicalTrials.gov identifier: NCT03131362; https://clinicaltrials.gov/ct2/show/NCT03131362).
Plain language summary
Keywords
Introduction
Chronic obstructive pulmonary disorder (COPD) is characterized by persistent respiratory symptoms and airflow limitation. 1 Despite being a preventable and treatable disease, 1 COPD is predicted to fourth leading cause of death globally by 2040. 2 In 2013, the mortality rate associated with COPD was higher in China compared with other countries [age-standardized mortality rate per 100,000 people (95% uncertainty interval) = 79.44 (71.48–88.79) in China 3 versus 50.7 (45.4–55.6) globally]. 4 In 2018, the estimated prevalence of COPD in China in those aged >40 years was reported to be 13.6–13.7%,5,6 which was higher than the estimations reported 10 years prior (8.2%). 7
The Chinese Thoracic Society recommends that physicians follow the Global Initiative for Chronic Obstructive Lung Disease (GOLD) evidence-based strategy document guidelines to manage patients with COPD (definitions of severity are consistent between the 2017 document and updated 2021 version).1,8 As per the GOLD strategy document, 1 both pharmacological and nonpharmacological treatments are key elements in the long-term management of stable COPD. Appropriate management of COPD is vital for patients, as more severe disease is associated with a greater risk of mortality. 9 We and others, however, have shown that real-world treatment patterns may differ from treatment guidelines.10–13
China comprises multiple geographic regions with a three-tier healthcare system (in general, primary hospitals provide general care in the community, secondary hospitals provide comprehensive care for regions, including referrals from primary care, while tertiary hospitals also provide specialist services, serve wider/multiple regions and are more often located in urban areas); therefore, understanding the current status of COPD management across these different geographic regions and hospital tiers is fundamental in developing strategies to improve the long-term management of patients with COPD. At the time of study initiation, there was a substantial lack of large-scale, real-world studies on the clinical management of patients with stable COPD in China. The REALizing and improving management of stable COPD in China (REAL) trial (NCT03131362) was a 52-week, prospective, observational, multicentre study designed to obtain reliable information on COPD management, outcomes and risk factors among a representative sample of patients with COPD in China across different hospital tiers. 14 Baseline 15 and primary outcomes 16 have been previously reported. Here, we report secondary and exploratory outcomes from the REAL trial.
Methods
Study design and population
Details of the study design and population have been previously published. 14 Briefly, the REAL study (NCT03131362) was conducted at 50 tertiary and secondary hospitals across six geographic regions in China. Hospitals were selected using a multistage, cluster sampling approach, and patients were consecutively enrolled during routine clinical visits between 30 June 2017 and 29 January 2019. Key inclusion criteria were (1) outpatients, (2) aged ⩾40 years, (3) clinically diagnosed with COPD [based on presence of chronic cough, sputum, wheeze and a history of exposure to harmful factors, and confirmed spirometry postbronchodilator forced expiratory volume in 1 s (FEV1)/forced vital capacity <0.7 as per the 2016 GOLD strategy document] 17 and (4) provision of informed consent. Patients were required to have stable COPD; those with an acute exacerbation within 4 weeks prior to enrolment were excluded.
Data collection
Patients were followed for 12 months, with two onsite visits (V0: at baseline; V1: at 1 year) and a telephone contact (TC) follow-up every 3 months following V0 (TC1–3). Baseline data were collected using case report forms (CRFs) at V0; symptoms, drug treatment, nondrug treatment, exacerbations, comorbidities, complications and direct costs were collected via CRFs at V0, V1 and TC1–3. Spirometry was performed as per usual clinical practice and was collected if available during study visits. Disease severity was assessed by measurement of airflow limitation (postbronchodilator FEV1) and assessment of symptoms/risk of exacerbations (GOLD 2016 and GOLD 2017 A/B/C/D classification).
Outcomes
The primary objective was to observe the 1-year clinical outcomes of patients with COPD under routine clinical treatment. Secondary and exploratory outcomes addressed in this report included the distribution of COPD maintenance therapy by disease severity, geographic region and hospital tier, the distribution of pharmacological and nonpharmacological treatments at each follow-up visit and mean total direct cost of COPD management over 1 year.
Statistical analysis
Statistical analysis was performed on the full analysis set (FAS), including all patients who fulfilled eligibility criteria and were successfully enrolled. Sample size calculation has been published previously. 14 Data analysis was primarily descriptive in nature; for continuous variables, mean, median, standard deviation (SD) and range were calculated, and for categorical variables, percentages were calculated. Patients lost to follow-up were withdrawn from the study and the reasons for withdrawal or discontinuation were determined. No imputation of missing data was used; all statistical analyses were carried out on nonmissing data only. Statistical analysis was performed using SAS version 9.4.
Results
Patient demographics and baseline characteristics
Between 30 June 2017 and 29 January 2019, 5097 patients were screened, of whom 5013 were enrolled, with 4978 patients included in the FAS. Patients originated from six geographic regions: north-east: N = 623 (12.5%), north: N = 1005 (20.2%), east: N = 1248 (25.1%), south-central: N = 904 (18.2%), north-west: N = 602 (12.1%) and south-west: N = 596 (12.0%). Approximately half the patients were recruited from tertiary hospitals (N = 2597, 52.2%) and the other half from secondary hospitals (N = 2381, 47.8%). Among the 4978 patients included in the FAS, a total of 772 withdrew from the study due to lost to follow-up (n = 565), withdrawal of consent (n = 117), death (n = 58) or other reasons (n = 32); the number of patients who dropped out of TC1, TC2, TC3 and V1 visits were 308 (6.2%), 423 (8.5%), 505 (10.1%) and 739 (14.8%), respectively.
Baseline patient demographics and characteristics for the overall cohort have been previously published. 15 Briefly, the mean (SD) age was 66.2 (8.9) years and the majority of patients were male (79.5%) (Table 1). Mean (SD) time since COPD diagnosis was 3.8 (6.2) years. Respiratory symptoms at baseline included shortness of breath (57.6%), wheezing (66.3%), chest tightness (66.8%), cough (81.1%) and purulent mucus (80.6%).
Patient demographics and clinical characteristics at baseline.

BMI, body mass index; COPD, chronic obstructive pulmonary disease; SD, standard deviation.
All percentages were calculated based on patients with available data.
Patient demographics and baseline characteristics according to geographic region and hospital tier are presented in Supplementary Table S1. Mean age was similar between regions (63.1–67.7 years) and hospital tiers (65.7–66.7 years). The proportion of males varied between regions (65.0–89.2%), but was consistent between hospital tiers (79.0–80.0%). The mean time since COPD diagnosis varied across regions (2.3–4.2 years) and was longer in secondary (4.5 years) compared with tertiary (3.1 years) hospitals.
According to disease severity assessed by airflow limitation, 10.1%, 41.7%, 34.5% and 13.6% of patients had mild, moderate, severe and very severe disease, respectively. Per GOLD 2016 combined assessment classification, 11.4%, 22.0%, 12.0% and 54.6% of patients were in groups A, B, C and D, respectively; per GOLD 2017 combined assessment, 16.4%, 41.9%, 7.3% and 34.4% of patients were in groups A, B, C and D, respectively (Table 2). A larger proportion of patients in secondary versus tertiary hospitals had high disease severity (severe versus very severe airflow limitation: 52.0% versus 44.4%; GOLD 2016 group C versus group D: 74.9% versus 58.6%; GOLD 2017 group C versus group D: 52.7% versus 31.6%) (Supplementary Table S2). Compared with other regions, the north had the highest proportion of patients with mild or moderate COPD and the lowest proportion of patients with severe or very severe COPD, regardless of disease severity assessment method (Supplementary Table S2).
COPD disease severity classified by airflow limitation, GOLD 2016 and GOLD 2017.

COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; V0, baseline visit; V1, visit at 1 year.
All percentages were calculated based on patients with available data.
The majority of patients (95%) received ⩾1 concomitant medication for respiratory diseases, including drugs for obstructive airway diseases (93.5%), cough and cold preparations (36.8%), unspecified herbal and traditional Chinese medicine (TCM, 25.6%), antibacterials for systemic use (25.5%) and corticosteroids for systemic use (10.1%) (Supplementary Table S3). Other concomitant medications received by ⩾1% of patients included calcium channel blockers (9.7%), agents acting on the renin–angiotensin system (7.0%), drugs used in diabetes (4.3%), antithrombotic agents (3.7%) and unspecified herbal and TCM (3.3%) (Supplementary Table S4).
Patients receiving pharmacological maintenance therapy
Distribution of prescribed stable COPD maintenance therapies by follow-up visit
Throughout the study, inhaled corticosteroids (ICSs)/long-acting beta-agonists (LABAs) (28.3–36.0%), long-acting muscarinic antagonists (LAMAs) (13.0–16.2%) and ICS/LABA + LAMA (17.5–18.7%) were the most frequently prescribed maintenance therapies. Overall, 1.7–4.4% patients received methylxanthines, 16.9–19.0% patients received mucolytics and 1.7–3.6% patients received TCM during the study. Notably, 11.6–15.8% of patients received neither ICS nor long-acting bronchodilators at each visit (Table 3). A full list of pharmacological treatments at baseline and 1 year can be found in the REAL baseline 15 and final outcomes 16 publications.
Distribution of prescribed COPD maintenance therapies at baseline, telephone contact follow-ups and at 1 year.
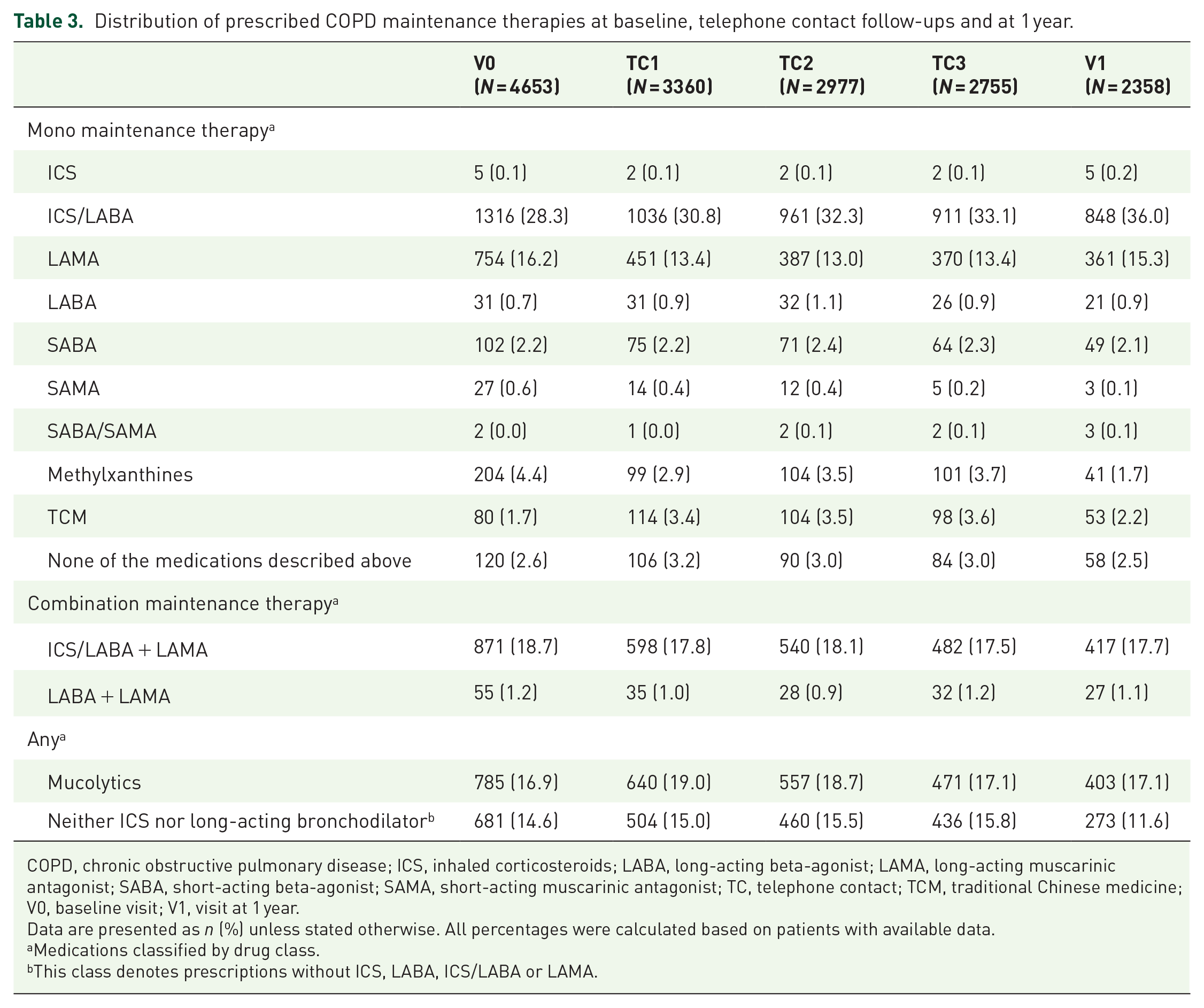
COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroids; LABA, long-acting beta-agonist; LAMA, long-acting muscarinic antagonist; SABA, short-acting beta-agonist; SAMA, short-acting muscarinic antagonist; TC, telephone contact; TCM, traditional Chinese medicine; V0, baseline visit; V1, visit at 1 year.
Data are presented as n (%) unless stated otherwise. All percentages were calculated based on patients with available data.
Medications classified by drug class.
This class denotes prescriptions without ICS, LABA, ICS/LABA or LAMA.
Distribution of prescribed stable COPD maintenance therapies at baseline and 1 year according to geographic region and hospital tier
At baseline, more patients in the north-west received ICS/LABA (36.2%) than in other regions (22.9–34.0%), and more patients in the east received LAMA (24.8%) or ICS/LABA + LAMA (25.9%) compared with other regions (LAMA: 8.7–16.0%; ICS/LABA + LAMA: 7.1–21.8%). Except for a large increase in the proportion of patients receiving ICS/LABA monotherapy in the north-east (34.0–54.0%), the distribution of maintenance therapies was largely similar between baseline and 1-year assessments (Table 4). Approximately one-quarter (24.5–27.0%) of patients in the north-east and south-west regions received neither ICS nor long-acting bronchodilator therapy at baseline. At 1 year, this proportion was the highest in the north (25.7%) (Table 4).
Distribution of stable COPD maintenance medication by geographic region and hospital tier.

COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroids; LABA, long-acting beta-agonist; LAMA, long-acting muscarinic antagonist; V0, baseline visit; V1, visit at 1 year.
All percentages were calculated based on patients with available data.
Subjects prescribed one and only mono or combination of medications on display, with no prohibition of being prescribed mucolytic and others at the same time.
ICS, ICS/LABA, LABA, LAMA, ICS/LABA + LAMA and LABA + LAMA not prescribed.
Overall, 27.7–35.4% of patients in tertiary hospitals and 28.9–36.4% of patients in secondary hospitals received ICS/LABA; LAMA monotherapy and ICS/LABA + LAMA were received by 18.3–19.5% and 22.1–24.6% of patients in tertiary hospitals, and 12.5–12.6% and 12.2–13.7% of patients in secondary hospitals, respectively (Table 4). At baseline, 25.4% of patients in secondary hospitals and 5.0% of patients in tertiary hospitals received neither ICS nor long-acting bronchodilators. At 1 year, this had decreased to 17.3% in secondary hospitals, while it remained consistent in tertiary hospitals (5.3%) (Table 4).
Distribution of prescribed stable COPD maintenance therapies at baseline and 1 year according to disease severity at baseline
Per GOLD 2017 combined assessment criteria, the proportion of patients receiving ICS/LABA maintenance therapy increased slightly with disease severity (GOLD groups A/B/C/D: 26.2%, 25.4%, 36.0% and 31.3%, respectively), while the proportion of patients receiving LAMA maintenance therapy decreased as disease severity increased (GOLD A/B/C/D: 24.5%, 16.4%, 17.5% and 11.7%, respectively). The proportion of patients receiving ICS/LABA + LAMA maintenance therapy was similar across disease severity groups (GOLD A/B/C/D: 19.9%, 18.1%, 17.2% and 19.3%, respectively) (Table 5), although ICS/LABA + LAMA use rose with increasing disease severity when severity was assessed by airflow limitation (10.9% mild, 15.7% moderate, 21.7% severe, 26.4% very severe). Overall, the proportions of patients receiving ICS/LABA, LAMA or ICS/LABA + LAMA (according to disease severity at baseline) were largely consistent between baseline and 1-year assessments (Table 5).
Distribution of prescribed COPD maintenance therapies by disease severity at baseline and at 1 year.

COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICS, inhaled corticosteroids; LABA, long-acting beta-agonist; LAMA, long-acting muscarinic antagonist; SABA, short-acting beta-agonist; SAMA, short-acting muscarinic antagonist; TCM, traditional Chinese medicine.
Data are presented as n/N (%) unless stated otherwise. All percentages were calculated based on patients with available data.
Medications classified by drug class.
This class denotes prescriptions without ICS, LABA, ICS/LABA or LAMA.
Few patients received short-acting beta-agonists (SABAs), short-acting muscarinic antagonists (SAMAs), SABA/SAMA or LABA + LAMA maintenance therapies for stable COPD, regardless of disease severity and severity assessment method (airflow limitation or GOLD 2016/2017 criteria) (Table 5). In general, more patients with group D disease as per GOLD 2017 combined assessment received SABA monotherapy (up to 4%) than those with group A, B or C disease. LABA + LAMA combination was received by 0.7–1.7% of patients throughout the study. At baseline, methylxanthines and TCM were used regardless of disease severity, and this trend was similar at the 1-year follow-up. Use of mucolytics was also similar across disease severity groups. Overall, there was a substantial proportion of patients who received neither ICS nor long-acting bronchodilators (no trend across severity groups) at baseline and 1 year (Table 5), despite increased symptoms and risk of exacerbation in patients with more severe disease.
Patients receiving nonpharmacological treatment
COPD health education was the most common nonpharmacological treatment at each study visit (89.0–95.6%), followed by lip reduction breathing (36.7–43.4%) and abdominal breathing (27.8–34.9%). At baseline, quitting smoking (16.8%) was the fourth most common nonpharmacological treatment, replaced by smoking reduction in subsequent follow-up visits (9.5–13.0%). Smoking cessation treatment (including quitting, reduction and no change) was provided in only 38.8%, 24.5%, 21.3%, 20.0% and 18.6% of patients at V0, TC1–3 and V1, respectively. At each visit, 1.6–6.8% of patients received vaccination for pneumonia, while 2.7–7.3% of patients received vaccination for influenza (Table 6).
Distribution of prescribed nonpharmacological therapies at baseline, telephone contact follow-ups and at 1 year.
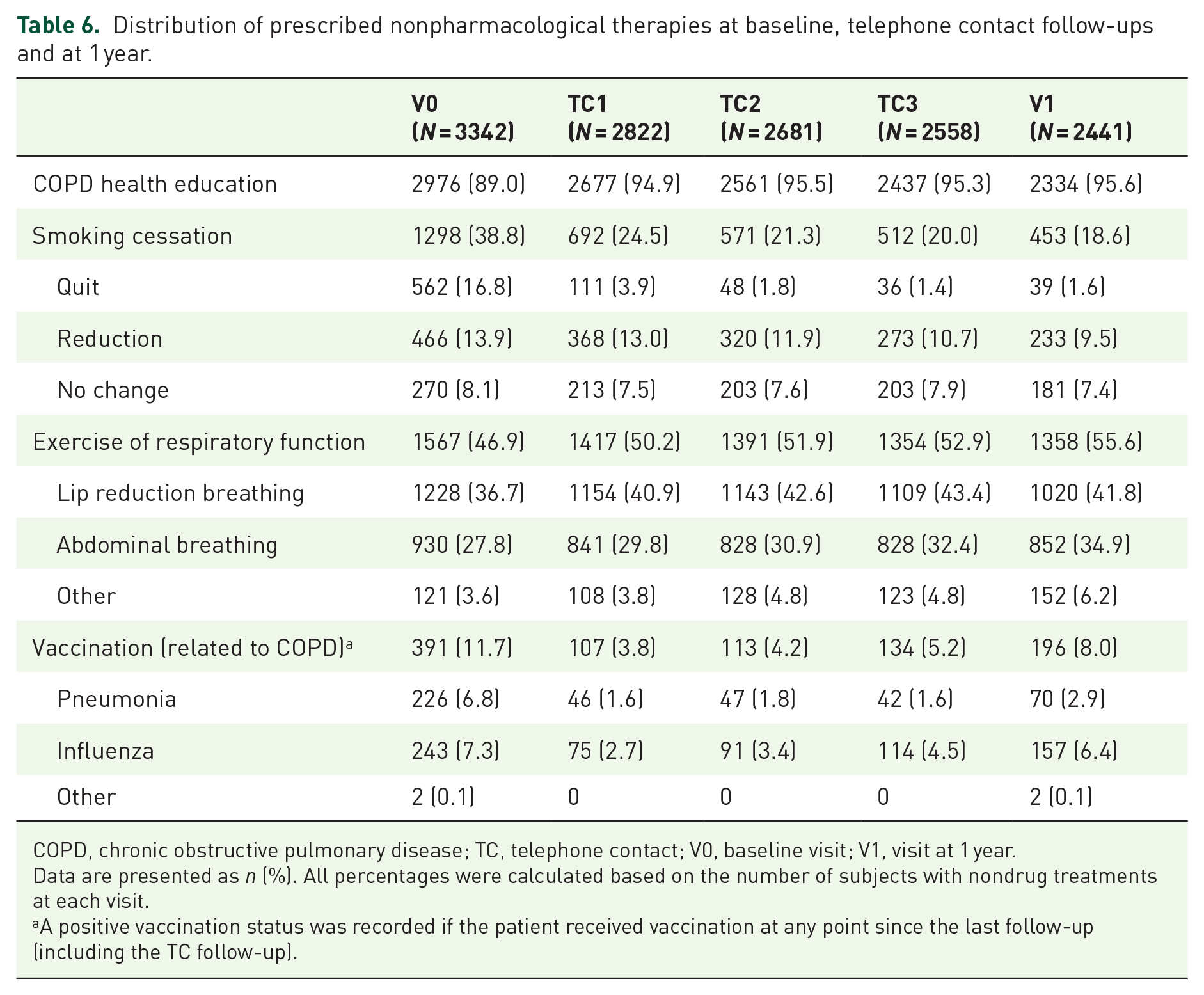
COPD, chronic obstructive pulmonary disease; TC, telephone contact; V0, baseline visit; V1, visit at 1 year.
Data are presented as n (%). All percentages were calculated based on the number of subjects with nondrug treatments at each visit.
A positive vaccination status was recorded if the patient received vaccination at any point since the last follow-up (including the TC follow-up).
Direct costs associated with COPD
Over the course of the study, the proportion of patients incurring any direct COPD cost was similar across disease severity categories at baseline (airflow limitation: 96.1–96.9%, GOLD 2016: 93.5–97.7%, GOLD 2017: 94.3–98.0%) (Table 7). The proportion of patients with maintenance treatment expenses was also similar across disease severity categories (airflow limitation: 95.4–96.9%, GOLD 2016: 92.5–97.2%, GOLD 2017: 93.5–97.7%) (Table 7). The median total direct cost and median treatment expenses, however, increased with worsening disease severity, and this trend was consistent regardless of the method of disease severity classification. The proportion of total direct COPD costs that were attributed to COPD maintenance treatment expenses reduced as disease severity increased (Table 7).
COPD costs by baseline COPD severity classified by airflow limitation, GOLD 2016 and GOLD 2017.

COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; RMB, renminbi.
Data are presented in RMB unless stated otherwise. All values were calculated based on patients with available data.
Discussion
REAL is the first nationwide study to collect prospective longitudinal real-world data on the management and clinical outcomes of a large cohort of Chinese outpatients with stable COPD. Here, we report treatment patterns among patients from six different geographic regions treated in secondary or tertiary hospitals, as well as treatment patterns by COPD severity. In addition, we report rates of nonpharmacological treatment and costs relating to treatment, to provide a deeper understanding of current COPD management across China.
Overall, a substantial proportion of patients enrolled in the REAL study had high disease severity; similar findings have been reported in three other multicentre, observational studies of patients with COPD in China.10,13,18 Final outcomes of the REAL study showed that a substantial proportion of patients with severe disease experienced exacerbations. 16 Supporting this, other multicentre, observational studies of patients with COPD in China showed that there is a positive correlation between disease severity and annual exacerbation rate.18,19 These data highlight the ongoing gap between the goals of COPD treatment 1 and real-world clinical outcomes of patients with COPD in China.
In the REAL study, which included a large, nationally representative sample of patients with COPD in China, ICS/LABA, LAMA and ICS/LABA + LAMA were the most frequently prescribed maintenance medications for stable COPD. These treatment patterns are similar to two previous observational studies in China, which reported that LAMA (34.8% and 39.1%), ICS/LABA (9.9% and 14.4%) and ICS/LABA + LAMA (39.4% and 39.0%) were the top three pharmacological treatments used.10,13 A real-world prospective longitudinal study that was carried out in 12 hospitals in China from 2016 to 2021 also reported similar proportions of patients with COPD who received LAMA (24.3%), ICS/LABA (10.4%) and ICS/LABA + LAMA (35.3%). 20
ICS/LABA was prescribed at a similar rate across disease severity groups, while LAMA monotherapy use decreased as disease severity increased. As the mean time from diagnosis in the REAL study was 3.8 years, this latter trend may be explained by nature of patients with a higher baseline disease severity having already had their treatment escalated beyond LAMA. Of note, LAMA monotherapy was consistently preferred over LABA monotherapy, which is consistent with GOLD strategy document. 1 On the other hand, it appears that physicians in China more often escalated treatment to ICS/LABA rather than the preferred LABA + LAMA combination. 1 In line with findings from Zeng et al., 13 LABA + LAMA use throughout the REAL study was consistently low (⩽1.7% regardless of disease severity), although it is worth noting that fixed-dose combination LABA/LAMA therapy was not available in China at the time of the study (LABA/LAMA therapy was included in the medical insurance catalogue in China at the end of 2019). 21 LABA/LAMA therapy has been shown to improve lung function and reduce exacerbation rates without an increase in adverse effects,21,22 but among patients with severe stable COPD treated with fixed-dose combination LABA/LAMA therapy, correct use was only reported in approximately 60%. 23 In the REAL study, ICS/LABA + LAMA use was higher in patients with more severe disease, although not when disease severity was categorized according to GOLD 2017. This suggests that the physician’s decision to step-up to triple therapy was driven by severity of lung function rather than acute exacerbation risk. On the other hand, Cui et al. 10 and Zeng et al. 13 reported a trend for increased use of ICS/LABA + LAMA with increasing disease severity as per GOLD 2017 combined assessment. Their studies enrolled patients from one and two geographic regions in China, respectively, whereas the REAL study enrolled patients from six different regions and found discrepancies in treatment use between the regions, which could account for the differences observed in prescription patterns between these studies.
At baseline, the proportion of patients who received LAMA or ICS/LABA + LAMA was the highest in the east region (24.8% or 25.9%, respectively) compared with other regions (8.7–16.0% or 7.1–21.8%, respectively); there were more patients at tertiary hospitals who received LAMA (19.5%) or ICS/LABA + LAMA (24.6%) compared with those at secondary hospitals (12.5% or 12.2%, respectively). This may be explained by the relative proportion of patients residing in the urban or rural areas across different geographic regions or hospital tiers. The east region has the highest proportion of patients from urban areas (62.0%) compared with other regions (35.4–60.6%). Most patients at tertiary hospitals were from urban areas (64.7%), whereas the majority of patients at secondary hospitals reside in rural areas (55.5%). A previous study has shown that patients from rural areas were less likely to seek medical advice and reported lower medication use compared with patients from urban areas. 24 In the study by Zeng et al., 13 in which patients were recruited from two provinces in the south-central/south region of China, there were more patients who received LAMA (39.1%) or ICS/LABA + LAMA (39.0%), compared with ICS/LABA (14.4%). In our study, however, there were less patients in the south-central region who received LAMA (8.7%) or ICS/LABA + LAMA (7.1%), compared with ICS/LABA (26.6%) at baseline. A community-based survey of approximately 25,000 participants across 10 regions in China revealed that Sichuan (south-west region) had the highest prevalence of COPD, but the lowest reported use of any COPD medication (10.3%). 24 While we did not observe this in this study, the south-west region had one of the highest proportions of patients who received neither ICS nor long-acting bronchodilators.
Overall, up to 15.8% of patients at each visit received neither ICS nor long-acting bronchodilators, although this was as high as 15.2–16.3% in patients with the most severe disease and reached >25% in some regions. A large observational study of COPD treatment patterns in Germany (N = 250,723) reported that 65.4% of patients were not prescribed inhaled maintenance treatment. 12 This sizable difference in inhaled therapy prescription between the studies may be due to (1) differences in time of data collection relative to COPD diagnosis; in the REAL study, mean time from diagnosis at study initiation was 3.8 years, whereas in the German study, data were collected from the date of first recorded COPD diagnosis and many patients were newly diagnosed and (2) differences in the hospital tiers included in the study; in the REAL study, patients were treated at secondary and tertiary hospitals, whereas in the German study, data were collected from medical records of patients treated in primary and secondary care. 12 We additionally observed a fivefold increase in the number of patients in secondary compared with tertiary hospitals that did not receive ICS or long-acting bronchodilators. These apparent differences in COPD management practices may result from disparities in the quantity and quality of respiratory services between hospital tiers in China.18,25,26 Hospital tier has been previously reported as a risk factor for acute exacerbation. 18 Moreover, a lack of formal gatekeeping in the hospital care system in China means that patients can access the system at any level and may not be referred to a more appropriate hospital tier if required.18,27 Tertiary hospitals in China, however, are responsible for treating more uncommon and complex respiratory illnesses than secondary hospitals, which may limit their capacity to accommodate patients with common chronic diseases such as COPD. 18 Tertiary hospitals in China are also often located far away from rural areas. In this study, we showed that the majority of tertiary hospitals were located in urban versus rural areas (64.7% versus 35.3%), and others have shown that patients prefer to access a local hospital when they have an acute exacerbation. 28 In the REAL study, there were more patients with severe disease in secondary versus tertiary hospitals, and together with our data on treatment patterns, this indicates that many patients may not have received adequate treatment. Vogelmeier et al. 12 reported that just over half the patients with one moderate baseline exacerbation and over one-third (36.9%) of patients with one severe baseline or multiple baseline exacerbations were not prescribed inhaled maintenance treatment at diagnosis, underscoring the importance of timely and appropriate prescription of pharmacological treatment in patients with stable COPD.
In addition to pharmacological treatment, nonpharmacological treatment in the form of education and self-management should be a major component of the long-term management of chronic diseases such as COPD. 1 Others have previously reported the benefits of nonpharmacological management, such as smoking intervention, pulmonary rehabilitation, breathing exercises and education programmes in reducing symptoms and mortality, as well as improving lung function and health-related quality of life in patients with COPD.29–36 In this study, COPD education was provided to almost all patients, but optimal self-management behaviour was evident in a much smaller proportion. Moreover, COPD knowledge was poor. We observed low uptake of respiratory function exercises, which are an important part of nonpharmacological treatment for COPD and contribute to pulmonary rehabilitation.1,37 REAL included the two most common breathing exercises that have been shown to reduce breathing frequency, improving chest wall tidal volume and exercise capacity in patients with COPD.31,37,38 We also found low levels of vaccination, with only 2.7–7.3% receiving influenza vaccination at each visit over the 12-month follow-up period. This was consistent with a 2022 cross-sectional study (1.7–10.9%) that recruited patients with COPD from eight hospitals across different tiers in China (tertiary, secondary or community hospitals). 18 The same study also showed that influenza vaccination in the previous year and pneumococcal vaccination in the previous 5 years were associated with reduced risk of acute exacerbation. 18 Other studies have also reported that influenza vaccination can effectively reduce the risk of acute exacerbation.39–41 In addition, influenza vaccination is recommended annually for all patients with COPD, 1 and thus, these data suggest an insufficient rate of vaccination in a vulnerable population. A recent study reported that patients treated for COPD in community hospitals had higher vaccination rates than those treated in secondary or tertiary hospitals, and that this might be due to physicians having more time to educate patients about the importance and benefits of vaccination. 18 Cultural factors (such as the traditional Chinese concept of visiting the hospital only when one is sick) may result in Chinese patients placing less importance on vaccination, which in turn may contribute to low vaccination rates. 18 As influenza vaccination is not included in the national immunization programme in China, patients are required to pay themselves and this may contribute to the low uptake of vaccinations. 42 Economically developed regions in China (e.g. Beijing) have started to offer free influenza vaccinations to individuals aged >60 years, and this has improved vaccination rates among eligible patients in the region. 42 Of note, Zeng et al. 13 also reported underprescription of nonpharmacological therapies among patients with COPD in China. Current evidence suggests low levels of COPD knowledge among clinicians, including respiratory physicians 43 ; therefore, the quality of COPD-related health education provided to patients in routine clinical visits should be further investigated.
Overall, we observed substantial variations in the use of pharmacological and nonpharmacological treatments for stable COPD across regions and hospital tiers in China, plus notable discrepancies between the real-world treatment patterns among patients with stable COPD in China and treatment guidelines for clinical practice. 1 These discrepancies may be due to several reasons. First, dual bronchodilation and triple therapy (which are recommended by the GOLD guidelines for the treatment of COPD) were not included in the medical insurance catalogue in China until recent years. 21 Second, tertiary hospitals are less accessible to patients living in rural areas in China. These patients tend to seek treatment at secondary hospitals, which should have the necessary skills and resources to treat COPD exacerbations. 28 Third, the lack of COPD knowledge among Chinese patients 16 may prevent them from seeking appropriate treatment and rehabilitation guidance. Finally, Chinese patients may prefer to combine TCM with pharmacological treatment, as shown in a recent survey on treatment preference among patients with COPD in China, 44 and this could be due to TCM being more affordable, especially to patients living in rural areas. 28
The REAL study additionally collected data on COPD-related costs, including those incurred from treatment. We found that patients with COPD have a high burden of COPD-related direct costs, particularly as a result of maintenance treatment, with costs increasing as disease severity increased. Maintenance treatment costs, however, represented a lower proportion of overall direct costs in patients with higher disease severity (59.7–76.4%) versus those with milder disease (80.8–93.7%). As reported in the final outcomes of the REAL study, patients with more severe disease experienced a higher rate of exacerbations. 16 This may have contributed to the disproportionate increase in additional direct costs for patients with higher disease severity. These data further support the importance of appropriate and timely management of stable COPD.
This study has several limitations. First, because step-up and step-down of treatment could be performed following improvement/worsening of disease severity, but the grouping of treatments prescribed at TC1–3 and V1 are presented by disease severity at baseline, we are unable to evaluate the association between treatment sequence and change in disease severity. As such, it is possible that the apparent association between treatment use and disease severity throughout the study does not accurately reflect real-world clinical practice. Given that the overall distribution of disease severity and treatment patterns (by disease severity) remained largely consistent across all follow-up assessments, however, we are confident that these data provide a good estimate of the current state of COPD management across China. Second, even though patients were classified by GOLD A/B/C/D groups throughout the study, these assessments can only be considered an indicator for actual disease severity. As per the GOLD strategy document,8,17 A/B/C/D groups are used to guide initial pharmacological treatment in clinical practice; in the REAL study, however, patients were not necessarily newly treated patients with COPD. Third, baseline data on maintenance medications were collected retrospectively and included both initial and follow-up treatments; therefore, nonadherence to the GOLD recommendations cannot be precisely estimated. Finally, implementation of the national hierarchical medical system allowed some patients to obtain their prescription medications from a community hospital, potentially influencing the reporting of treatment patterns as these prescriptions would not be recorded at the secondary or tertiary hospitals included in this study.
Conclusion
The majority of patients in the REAL study had moderate-to-severe disease, suggesting that this level of disease may be prevalent among patients with COPD who attend regular outpatient visits in secondary or tertiary hospitals in China. The most common treatment regimens prescribed to patients with stable COPD in this study were ICS/LABA, LAMA and ICS/LABA + LAMA, and our results indicate that lung function may be the primary indicator for treatment escalation in patients with COPD in China. In terms of nonpharmacological management, rates of respiratory function training, smoking intervention and vaccination administration require improvement. Overall, our results indicate that there may be inconsistencies between treatment guidelines and current clinical practice across China, reflecting a need to improve the long-term management of stable COPD nationwide, although particularly in secondary hospitals. We hope that better adherence to current treatment guidelines may improve disease-related outcomes and the financial burden on patients.
Supplemental Material
sj-docx-1-tar-10.1177_17534666231158283 – Supplemental material for Treatment patterns in patients with stable COPD in China: analysis of a prospective, 52-week, nationwide, observational cohort study (REAL)
Supplemental material, sj-docx-1-tar-10.1177_17534666231158283 for Treatment patterns in patients with stable COPD in China: analysis of a prospective, 52-week, nationwide, observational cohort study (REAL) by Ting Yang, Baiqiang Cai, Bin Cao, Jian Kang, Fuqiang Wen, Yahong Chen, Wenhua Jian and Chen Wang in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
The authors acknowledge Alice Carruthers BSc (Hons), PhD of Nucleus Global Asia Pacific for editorial assistance and AstraZeneca China for the funding in accordance with Good Publication Practice (GPP3) guidelines.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.