
Abstract
Background:
A few studies have reported the medium-sized and small airway morphological abnormalities of bronchiolitis. Whether spirometry or impulse oscillometry (IOS) is correlated with airway remodeling of bronchiolitis remains unclear.
Objectives:
Aiming to demonstrate the airway morphological abnormalities of bronchiolitis obliterans (BO) and diffuse panbronchiolitis (DPB) assessed by endobronchial optical coherence tomography (EB-OCT), and elucidate whether spirometric and IOS parameters have correlation with the airway remodeling of bronchiolitis.
Methods:
We recruited 18 patients with bronchiolitis (BO, n = 9; DPB, n = 9) and 17 control subjects. Assessments of clinical features, St. George’s respiratory questionnaire (SGRQ), chest computed tomography (CT), spirometry, IOS, and EB-OCT were performed in all enrolled subjects. The correlation between EB-OCT and lung function parameters was studied and analyzed.
Results:
The magnitude of abnormalities of spirometric and IOS parameters was significantly greater in patients with bronchiolitis than that in control subjects (p < 0.05). Patients with BO had notably lower forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), FEV1/FVC, maximal mid-expiratory flow (MMEF)% pred and higher resonant frequency (Fres), and area of reactance (AX) than those with DPB (p < 0.05). The EB-OCT measurement among patients with bronchiolitis and between the bronchus in the left and the right lung demonstrated a heterogeneous distribution of airway calibers, presenting a high intra- and inter-individual variability. Patients with bronchiolitis had notably greater airway wall area (p < 0.05) compared with control, while BO presented greater magnitude of airway abnormalities than DPB. Fres and the difference in airway resistance at 5 and 20 Hz (R5–R20) correlated negatively with medium-sized and small airway inner area, and correlated positively with airway wall area (p < 0.05), whose correlation coefficients were higher than those of spirometric parameters.
Conclusion:
Bronchiolitis, BO and DPB, manifested a heterogeneous distribution of airway calibers with significant intra- and inter-individual variability. IOS parameters, rather than spirometry, correlated better with medium-sized and small airway remodeling in bronchiolitis assessed by EB-OCT measurement.
Keywords
Introduction
Bronchiolitis, a general term that used to designate inflammatory injury in small airways, is ordinarily associated with pulmonary infection, connective tissue disease, allotransplantation, inhalation injury, or gastroesophageal reflux.1–4 Bronchiolitis obliterans (BO), diffuse panbronchiolitis (DPB), and follicular bronchiolitis (FB) are the major histologic patterns of bronchiolitis. 5 BO and DPB commonly present with cough, tachypnea, and dyspnea due to deteriorated airflow obstruction.6,7 It would be of great importance in illustrating the airway morphological abnormalities of bronchiolitis to determine appropriate treatment and improve clinical outcomes. The current challenge in clinical practice is, however, to detect the small airway remodeling of bronchiolitis and evaluate the severity of disease in terms of airway structural characteristics and clinical investigations.
High-resolution computed tomography (HRCT) plays a pivotal role in delineating airway structural changes and assessing the extent and progression of lung disease.8,9 Lung volume measurements and paired inspiratory/expiratory computed tomography (CT) are commonly used to detect low-attenuation areas and evaluate air trapping. 10 HRCT, however, might have a limitation in serving as an accurate detection of small airway morphology (up to the seventh generation or more distal airways) 11 due to the finite resolution measurement.12,13 Furthermore, the inspiratory/expiratory CT might expose patients to additional radiation. Spirometry, provides the overall lung function evaluation, is currently delayed in surveying of small airway disorders with its low sensitivity and forced expiratory maneuver. 14 Generally, airflow obstruction on spirometry do not occur until small airways disorder is widespread and lesions are inclined to be irreversible. 15 Hence, whether the airway morphological abnormalities are synchronous with lung function impairment in bronchiolitis remains elusive.
Endobronchial optical coherence tomography (EB-OCT), provides a high resolution imaging of medium-sized and small airway structure, has emerged as a novel modality for evaluating the airway remodeling in vivo. 16 EB-OCT has good correlations with CT imaging and histopathological findings17,18 for distinguishing epithelial epithelium, lamina propria, and airway cartilage structure. 19 In this study, we investigated the airway morphological abnormalities of bronchiolitis by EB-OCT imaging, and furthermore, assessed whether pulmonary function test [spirometry and impulse oscillometry (IOS)] was associated with medium-sized and small airway structural abnormalities in bronchiolitis.
Methods
We conducted a prospective observational study with cross-sectional design in the First Affiliated Hospital of Guangzhou Medical University from May 2017 to January 2022. The clinical diagnosis of bronchiolitis was made mainly on the basis of medical history, lung function test, and pathological findings.20,21 All the patients were recruited in clinically stable condition, presenting ground-glass opacity and diffuse centrilobular tree-in-bud appearance assessed by chest CT imaging. Patients with acute pulmonary infection within 6 weeks, pre-existing respiratory conditions [chronic obstructive pulmonary disease (COPD), asthma, etc.], end-stage lung disease manifested as evident bronchiectasis, and age less than 20 years were excluded from the study. Whereas, as mentioned in our previous report, 11 patients with normal lung function and small peripheral pulmonary nodules (<3 cm in diameter) who received bronchoscopy were recognized as control subjects. All subjects enrolled in this study received evaluations of spirometry, IOS, St. George’s respiratory questionnaire (SGRQ), erythrocyte sedimentation rate (ESR), and EB-OCT imaging.
We performed spirometry and IOS (Jaeger, Hoechberg, Germany) based upon the international guideline. 22 Pulmonary function test was conducted on the day before the CT and EB-OCT examination. The spirometric parameters forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), maximal mid-expiratory flow (MMEF), and IOS parameters respiratory impedance at 5 Hz (Z5), resonant frequency (Fres), airway resistance at 5 Hz (R5), airway resistance at 20 Hz (R20), the difference in airway resistance at 5 and 20 Hz (R5–R20), reactance at 5 Hz (X5), and area of reactance (AX) were tested and compared.
EB-OCT scan was conducted using Lightlabs C7XR OCT system (St. Jude Medical, St. Paul, MN, USA). The OCT catheter (0.9 mm in diameter) was advanced to the bronchus under the guidance of flexible bronchoscope (B260F, Olympus, Japan). The airway structure was detected upon breath hold at the end of full inspiration. EB-OCT scans were performed from the third to ninth generation bronchus of bilateral lower lobe (RB7, RB8, RB9, RB10 and LB7, LB8, LB9, LB10 segments, respectively). The inner luminal area (Ai), airway wall area (Aw), and percentage of airway wall area [denoted as: Aw% = [Aw/(Ai + Aw) × 100%]] were measured and analyzed. The EB-OCT measurement from the third to sixth generation and that from the seventh to ninth generation of bronchi was, respectively, averaged to reflect the magnitude of structural changes of the medium-sized and small airways.
Statistical analysis was performed using SPSS version 22.0 (SPSS Inc., Chicago, IL, USA). Normally distributed data were expressed as mean value ± standard deviation. Differences among groups were analyzed using one-way analysis of variance. The Bland–Altman analysis was conducted to demonstrate the concordance of EB-OCT measurement between the bronchus in the left and the right lung. The association between EB-OCT and lung function parameters was determined with Pearson’s or Spearman’s correlation model when appropriate. The p value < 0.05 was considered to indicate a significant difference unless otherwise stated.
Results
Demographic characteristics
The study cohorts consisted of 18 patients with bronchiolitis (9 cases with BO and 9 cases with DPB) and 17 control subjects. The majority of patients with bronchiolitis suffered from a persistent cough and progressive shortness of breath. There was no significant among-group difference in terms of age and body mass index (BMI) (all p > 0.05, Table 1). Whereas, there were more female patients and longer course of disease in BO group than those in DPB group. Patients with BO had higher SGRQ score but lower ESR than those with DPB, whereas these did not achieve statistical difference (p = 0.221 and p = 0.357, respectively).
Demographic characteristics.

All: BO + DPB; BMI, body mass index; BO, bronchiolitis obliterans; DPB, diffuse panbronchiolitis; ESR, erythrocyte sedimentation rate; SGRQ, St. George’s respiratory questionnaire.
p value denoted the comparison between BO group and DPB group and between bronchiolitis group and control group, respectively.
Spirometry and IOS examination in bronchiolitis
The magnitude of abnormalities of spirometric and IOS parameters was greater in patients with bronchiolitis than that in control subjects (all p < 0.05, Table 2). Furthermore, patients with BO had notably lower FEV1, FVC, FEV1/FVC, MMEF% pred and higher Fres, and AX compared with DPB (all p < 0.05), whereas R5–R20 and X5 were comparable between these two groups (both p > 0.05).
Comparison of spirometry and IOS in BO and DPB.

All: BO + DPB; AX, area of reactance; BO, bronchiolitis obliterans; DPB, diffuse panbronchiolitis; FEV1, forced expiratory volume in1 s; Fres, resonant frequency; FVC, forced vital capacity; MMEF, maximal mid-expiratory flow; R5, airway resistance at 5 Hz; R20, airway resistance at 20 Hz; R5–R20, the difference in airway resistance at 5 and 20 Hz; X5, reactance at 5 Hz; Z5, respiratory impedance at 5 Hz.
p value denoted the comparison between BO group and DPB group and between bronchiolitis group and control group, respectively.Data in boldface indicated the comparison with statistical significance.
Airway morphological abnormalities of bronchiolitis assessed by EB-OCT
The Bland–Altman analysis revealed a modest concordance of EB-OCT measurement (Ai3–6 and Ai7–9) between the bronchus in the left and the right lung (Figure 1), indicating a heterogeneous distribution of airway caliber in the varied basal segment.

The Bland–Altman analysis for EB-OCT measurement (Ai3–6 and Ai7–9) between the bronchus in the left and the right lung (n = 18).
Compared with control subjects, patients with bronchiolitis presented notably greater airway wall area (Aw%7–9 and Aw%3–9) (both p < 0.05), whereas the mean airway luminal area (Ai3–6 and Ai7–9) was comparable between these two groups (Table 3), which might be attributed to the heterogeneous distribution of airway luminal calibers with intra- and inter-individual variability (Figures 2 and 3). Moreover, patients with BO had greater magnitude of airway abnormalities compared with those with DPB, but only Ai7–9 exhibited significant difference between these two groups (2.23 ± 0.92 versus 3.11 ± 0.84, p = 0.049).
Airway morphological abnormalities of BO and DPB.
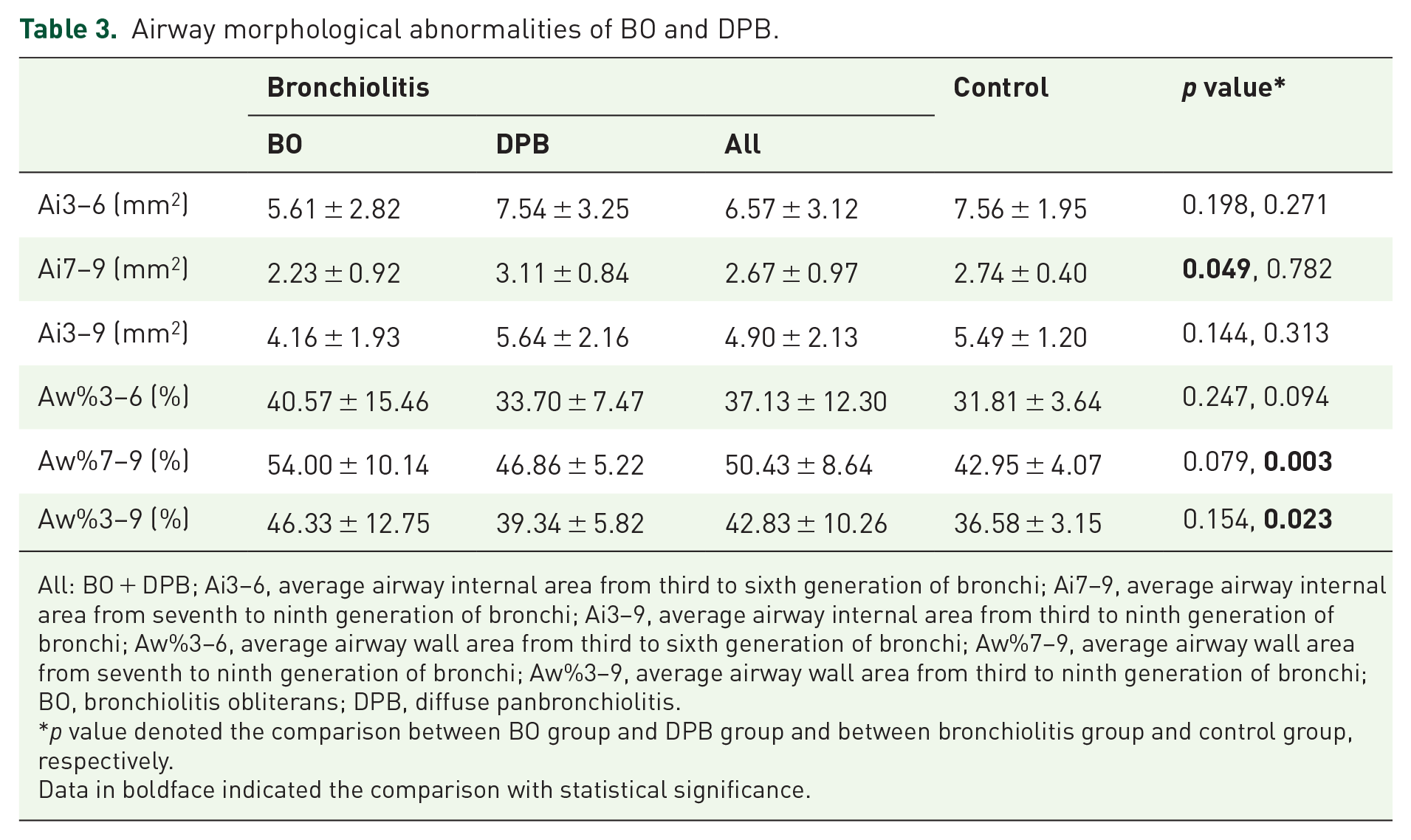
All: BO + DPB; Ai3–6, average airway internal area from third to sixth generation of bronchi; Ai7–9, average airway internal area from seventh to ninth generation of bronchi; Ai3–9, average airway internal area from third to ninth generation of bronchi; Aw%3–6, average airway wall area from third to sixth generation of bronchi; Aw%7–9, average airway wall area from seventh to ninth generation of bronchi; Aw%3–9, average airway wall area from third to ninth generation of bronchi; BO, bronchiolitis obliterans; DPB, diffuse panbronchiolitis.
p value denoted the comparison between BO group and DPB group and between bronchiolitis group and control group, respectively.Data in boldface indicated the comparison with statistical significance.

Heterogeneous distribution of airway calibers with high inter-individual variability in bronchiolitis. Airway inner area from the third to ninth generation of bronchi in bronchiolitis group (a, 18 cases) and control group (b, 17 cases). Each line represented the trend of airway inner area changes from the third to ninth generation bronchi in one case. The line chart of bronchiolitis group (a) displayed greater dispersion than that of control group (b).

Heterogeneous distribution of airway calibers with high intra-individual variability in bronchiolitis. Longitudinal section of airway morphology from the third to ninth generation of bronchi in RB8 (a) and LB8 (b) segment of bronchiolitis, assessed by EB-OCT. (a) Airway narrowing was detected in the eighth and ninth generation of bronchi, but focal bronchiectasis was shown in the sixth and seventh generation; (b) focal bronchiectasis was demonstrated in the eighth and ninth generation of bronchi, while airway constriction was found from the fifth to seventh generation of bronchi.
Correlation between EB-OCT and spirometric and IOS parameters in bronchiolitis
FEV1, FVC, and FEV1/FVC had partially positive correlation with airway caliber (Ai3–6 and Ai7–9), but not with airway wall thickening in patients with bronchiolitis (all p > 0.05, Table 4). It was noteworthy that IOS parameters, Fres and R5–R20, correlated negatively with medium-sized and small airway inner area (Ai3–6: r = −0.637, p = 0.009 and r = −0.693, p = 0.009; Ai7–9: r = −0.764, p = 0.002 and r = −0.660, p = 0.014, respectively), and positively with airway wall area (Aw%3–6: r = 0.610, p = 0.027 and r = 0.619, p = 0.024; Aw%7–9: r = 0.681, p = 0.010 and r = 0.707, p = 0.007, respectively), whose correlation coefficients were higher than those of spirometric parameters. Whereas X5 and AX correlated with small airway structural abnormalities of bronchiolitis (Ai7–9: r = 0.645, p = 0.017 and r = −0.703, p = 0.007; Aw%7–9: r = −0.438, p = 0.134 and r = 0.571, p = 0.041, respectively). While Ai3–6 and Ai7–9, rather than Aw%3–6 and Aw%7–9, had significant correlation with SGRQ score (r = −0.642, p = 0.004 and r = −0.721, p = 0.001, respectively).
Correlation between OCT, spirometry, IOS, and SGRQ in bronchiolitis.
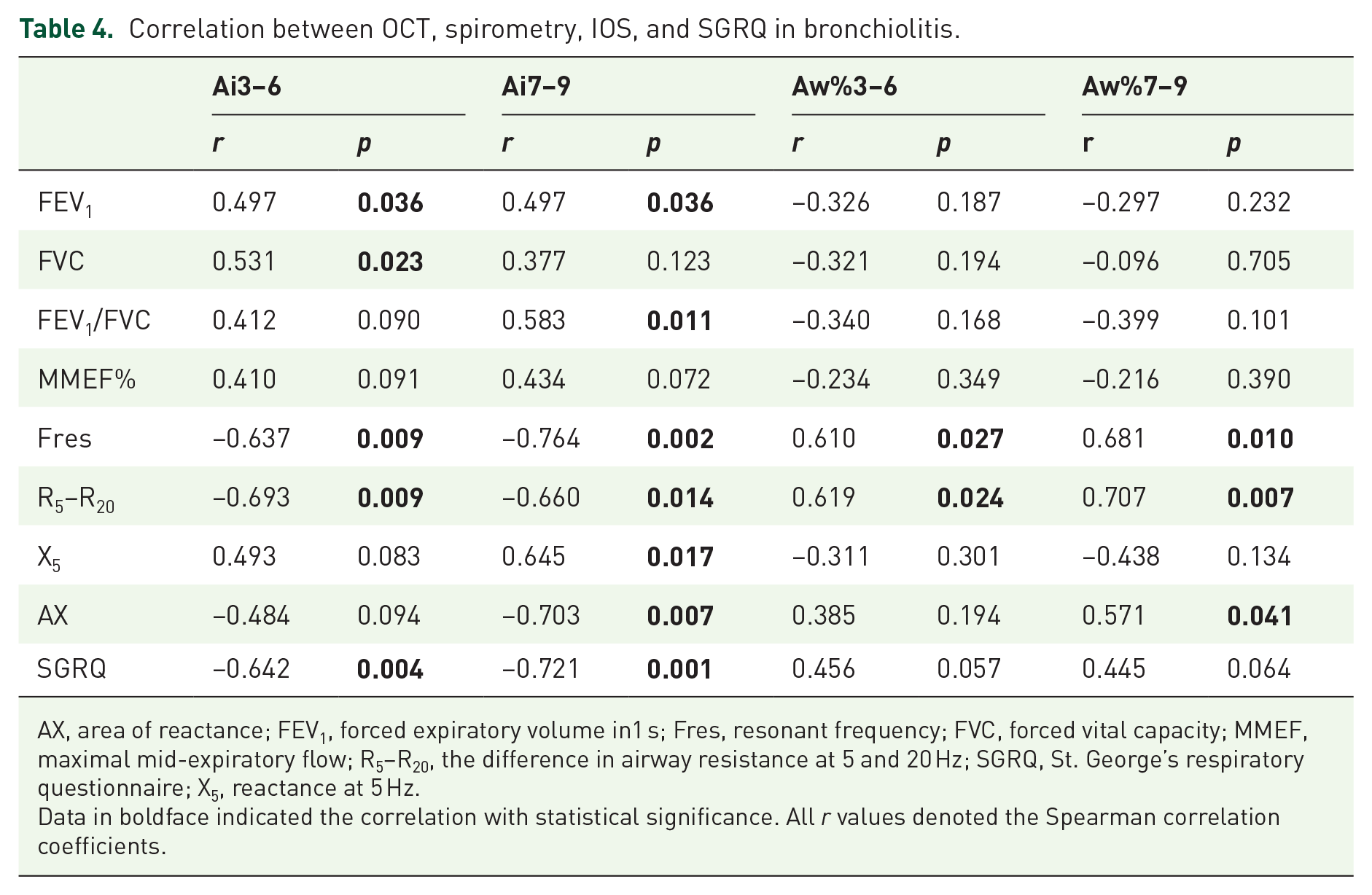
AX, area of reactance; FEV1, forced expiratory volume in1 s; Fres, resonant frequency; FVC, forced vital capacity; MMEF, maximal mid-expiratory flow; R5–R20, the difference in airway resistance at 5 and 20 Hz; SGRQ, St. George’s respiratory questionnaire; X5, reactance at 5 Hz.
Data in boldface indicated the correlation with statistical significance. All r values denoted the Spearman correlation coefficients.
Discussion
This was the first study that reported the medium-sized and small airway morphological abnormalities of bronchiolitis assessed by EB-OCT. We had demonstrated the airway structural characteristics of BO and DPB, and elucidated their association with spirometric and IOS parameters. The results revealed that patients with bronchiolitis presented notable airway wall thickening and heterogeneous ventilation. Furthermore, IOS parameters Fres and R5–R20, rather than spirometry, had significant correlation with medium-sized and small airway remodeling of bronchiolitis (airway luminal narrowing and airway wall thickening).
BO, characterized by progressive fibrinous obliteration of small airways and persistent spirometric airflow obstruction, 4 is mostly correlated with chronic graft-versus-host disease due to solid organ transplantation or hematopoietic stem cell transplantation.1,23,24 Bronchiolar inflammation and peribronchiolar fibrosis-induced airway luminal obliteration are considered as the hallmarks of pathological features in BO. 25 Comparatively, DPB, associated with chronic airway inflammation and immune dysfunction,26,27 is characterized by inflammatory infiltration involved the airway wall and fine yellowish nodules in the parenchymal area, which could lead to airway narrowing and bronchiectasis occurs as the disease progression.28–30 HRCT findings reveal that bronchiolar diseases commonly represent as air trapping (mosaic pattern or ground-glass attenuation) and small airway wall thickening (centrilobular nodules with tree-in-bud appearance).31–34 Pathologically, the tree-in-bud appearance indicates lymphocytic infiltration involved the thickened airway wall or bronchiolar luminal impaction with mucous, while mosaic pattern and ground-glass attenuation represent granulation tissue and scar foci patchily encroach on the bronchiolar lumen. 35
The previous studies suggested that the peripheral airway is the major site of airway obstruction in BO and DPB. 36 Spirometric parameter FEV1 reveals the large- and medium-sized airway caliber, while MMEF% pred is reportedly implemented to represent the small airways function.37,38 In this study, FEV1, FVC, FEV1/FVC, and MMEF% pred were significantly reduced in BO compared with those in DPB, which were in accordance with the course of disease and SGRQ score. The forced oscillation technique has been introduced to measure airway function at varied oscillation frequency.39,40 Generally, Fres indicates the inertial properties of airways and the capacitance of lung periphery, respiratory resistance (Rrs) reflects the airway luminal caliber and ventilation heterogeneity,41,42 whereas airway obstruction and heterogeneous distribution of airway caliber might increase Xrs, which represents respiratory system stiffness. In this regard, this study demonstrated that IOS parameters in patients with BO were more inferior than those with DPB, suggesting that BO might had greater magnitude of airway remodeling (luminal narrowing and airway wall thickening) compared with DPB. Hence, it was therefore plausible that the correlation of pulmonary function test and airway morphological measurement would be conducive to the differential diagnosis and optimizing management of bronchiolar diseases.
The recent study has reported the small airway dilation in chronic lung allograft dysfunction (CLAD) assessed by EB-OCT, which would be a potential diagnostic indicator for CLAD and CLAD phenotype (BO syndrome and restrictive allograph syndrome). 43 In this study, the EB-OCT measurement demonstrated a heterogeneous distribution of airway calibers in BO and DPB (presented as focal airway narrowing and/ bronchiectasis), which correspondingly manifested as ground-glass opacity and diffuse centrilobular tree-in-bud appearance assessed by chest CT imaging.31–34 The large range of airway luminal area in the medium-sized and small airways reflects high intra- and inter-individual variability, which in part might lead to the absence of significant correlations with spirometric parameters. Taking this into account, the proximal medium-sized airway might have limited predictive power to reflect the distal small airway caliber in bronchiolitis. In this regard, the heterogeneous ventilation and airway modeling in bronchiolitis might vary from those in obstructive lung disease (COPD, asthma, etc),14,44 which is characterized by wedge-shaped airway abnormalities from the segmental airways to the periphery.
Based upon the EB-OCT imaging, patients with bronchiolitis presented notably greater airway wall area compared with control subjects, whereas BO had greater magnitude of small airway wall thickening than DPB, which was congruent with spirometric and IOS measurement. Furthermore, although FEV1 and FVC generally assess the airflow limitation, we found that the greater magnitude of abnormality of IOS parameters could sensitively represent more severe airway remodeling in bronchiolitis. Fres and R5–R20, rather than spirometric parameters, had better correlation luminal area and airway wall area assessed by EB-OCT measurements. In this study, we attempted to investigate a sensitive lung function parameter to correlate with the airway morphological abnormalities in bronchiolitis, which might act as a potential surrogate marker for evaluating the therapeutic effect of bronchiolitis.
Some limitations should be acknowledged. First, this cross-sectional study was performed in a single center with small sample sizes, which might limit the statistical power. The large-scale investigation on airway morphology is warranted to further validate the diagnostic and assessed value of EB-OCT for varied subtype of bronchiolitis. Second, patients recruited in this study irrespective of disease severity grading, which could lead to subjective bias. Nevertheless, this study was not conducted to determine the diagnostic accuracy of EB-OCT in bronchiolitis, but demonstrate the airway morphological abnormalities of BO and DPB, and their correlation with spirometric and IOS assessment. Third, the EB-OCT probe could only reach the ninth to tenth generation bronchi because of technical constraints, our results might not accurately reflect the whole peripheral small airways. Forth, the lack of comparative analysis of inflammatory markers expression might limit the comprehensive understanding of relationship between inflammatory pathogenesis and airway morphological abnormalities. Hence, the clinical utility and prognostic value of IOS and EB-OCT measurement in bronchiolitis require further validation by subsequent investigation of airway inflammation and airway structural follow-up observation.
In conclusion, bronchiolitis (both BO and DPB) manifests a heterogeneous distribution of airway calibers with significant intra- and inter-individual variability. IOS parameters Fres and R5–R20, rather than spirometry, correlate better with medium-sized and small airway remodeling in bronchiolitis assessed by EB-OCT measurement.