
Abstract
Bronchiolitis obliterans (BO) is in general a rare and life-threatening form of non-reversible obstructive lung disease in which the bronchioles are compressed and narrowed by fibrosis and/or inflammation. The purpose of this study was to evaluate the clinical features of BO in pediatric patients and explore its risk factors. The medical records of 35 pediatric patients with BO at Guangzhou Women and Children’s Medical Center were evaluated. The age at onset of symptoms was 2–42 months (mean 13.3 ± 8.9 months), with age at diagnosis of 5 months–4 years (mean 17.8 ± 9.0 months). High-resolution computed tomography findings included mosaic pattern (100%), atelectasis (37.1%), air trapping (31.4%), and bronchiectasis (20.0%). Three patients received lung biopsies and mainly exhibited an inflammatory process surrounding the lumen of bronchioles. BO predominantly resulted from post-infectious causes (91.4%) which were primarily caused by adenovirus (50%), followed by Mycoplasma pneumoniae (46.7%) and influenza (20%). Pulmonary function tests (PFTs) showed severe and fixed airflow obstruction, decreased compliance, and increased resistance. No significant difference was found between before and after steroid treatment (P > 0.05). Two patients died owing to severe pulmonary complications, one of whom had inherent immunodeficiency. Our study suggests that the occurrence of BO, especially post-infectious BO, in China is relatively high and might result from primary immunodeficiency diseases in severe cases. Recurrent aspiration pneumonia caused by congenital dysplasia of the larynx and vaccination not on schedule might be potential risk factors for persistent and recurrent BO.
Introduction
Bronchiolitis obliterans (BO) is a rare and life-threatening form of non-reversible obstructive lung disease in which the bronchioles (small airway branches) are compressed and narrowed by fibrosis (scar tissue) and/or inflammation. Histologically, BO is characterized by the presence of intraluminal granulation tissue (i.e. peribronchial fibrosis) in the airways and/or inflammation-induced lumen narrowing, which gives rise to scarring and obstruction. 1 The most common form of BO is irreversible and caused by progressive infection in the lower respiratory tract induced by viral infections. The disease has also been found and reported worldwide in children with its severity and outcome dependent upon the geographic area.2–4 Much less is known about its incidence, causes, and outcomes, although there have been a growing number of pediatric cases during the last decades in China.3,5,6 In this study, we analyzed 35 pediatric patients diagnosed with BO in China. The purpose of this study was to evaluate the clinical features of BO in pediatric patients and explore its risk factors.
Materials and methods
Clinical data
This study included 35 patients diagnosed with BO who were followed up at Guangzhou Women and Children’s Medical Center from May 2011 to September 2015. A diagnosis of BO was made using criteria previously reported as follows:1,7,8 (1) persistent obstructive symptoms with wheezing that do not respond to bronchodilator administration for more than 6 weeks after the first symptom and (2) high-resolution chest tomography (HRCT) findings of a mosaic pattern. Patients with other diagnoses, such as severe asthma, pulmonary tuberculosis, bronchopulmonary dysplasia, foreign body in bronchus, cystic fibrosis, and congenital heart disease, were excluded in accordance with routine inpatient service and clinical and laboratory evaluations during follow-up. This study was conducted in accordance with the Declaration of Helsinki. This study was conducted with approval from the Ethics Committee of Guangzhou Women and Children’s Medical Center, Guangzhou Medical University. Written informed consent was obtained from all participants’ guardians.
Treatment of the patients
For each patient, demographic data, clinical presentation, imagenological characteristics, pulmonary function tests (PFTs), laboratory data, treatment, response to therapy, bronchoalveolar lavage (BAL) findings, and outcome were collected. Oxygen saturation was measured using digital oximetry. HRCT was performed in all patients, and 18 cases underwent PFT. All patients underwent indirect immunofluorescence viral testing of nasopharyngeal secretions during the acute phase of the disease to identify adenovirus, respiratory syncytial virus (RSV), influenza, parainfluenza virus, rhinovirus, bocavirus, or human metapneumovirus positivity. Blood cultures were obtained for suspected bacterial infection, Mycoplasma pneumoniae, or fungal infection. All patients underwent echocardiography to rule out heart disease and determine pulmonary artery pressure indirectly. Oxygen therapy was used for patients whose oxygen saturation levels were below 94% to correct hypoxemia and prevent pulmonary hypertension development. Persistent and severe cases received an empirical course of low-dose systemic corticosteroids during the acute phase, and bronchodilators were used during pulmonary exacerbations. (We used systemic corticosteroid therapy with intravenous/oral methylprednisolone 2 mg/kg one to two times per day for 3–5 consecutive days. The application was then halved thereafter for 2–5 days.) An inhaled corticosteroid (budesonide) and oral macrolides were administered during the remission phase. (Inhaled budesonide was applied 0.5 mg + NS2 mL/every time, two times per day, for 3–6 months. The same application was then halved for 5 and 26 months. Oral azithromycin was given with 5 mg/kg one time per day, thrice weekly. The treatment period for the azithromycin therapy ranged between 1 and 3 months.)
The patients were followed up periodically in the out-patient department. In all, 29 patients received follow-up HRCT scans at a mean interval of 3–6 months (range 7 days–4 years), and 13 were followed up by PFT at a mean interval of 3–6 months (range 1 month–1 year).
Statistical analysis
SPSS24.0 was used for the statistical analysis. The measurement data were expressed as
Results
Characteristics of patients
The study group consisted of 21 boys and 14 girls (male:female ratio = 1.5:1.0). The length of medical history ranged from 45 days to 2 years. The age at the onset of symptoms was 2–42 months (mean = 13.3 ± 8.9 months), with age at diagnosis of 5 months to 4 years (mean = 17.8 ± 9.0 months; Figure 1). No seasonal or yearly variation in BO frequency was detected. At the time of onset, 32 patients (91.4%), who were previously healthy, had acute bronchiolitis or severe pneumonia. All patients exhibited persistent or intermittent wheezing or rales on auscultation. Other common clinical findings were crackles/wheezing, exercise intolerance, tachypnea, and dyspnea. The clinical characteristics of the cases are summarized in Figure 2.
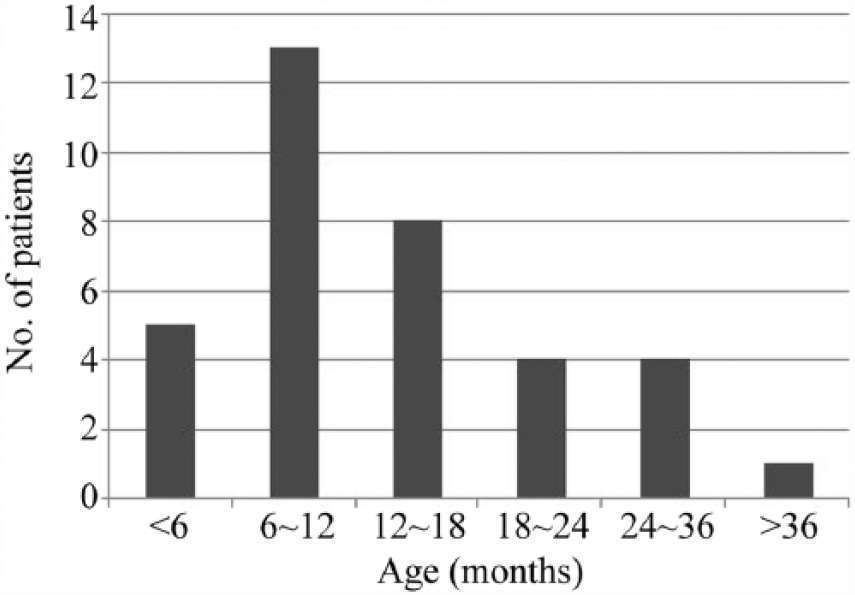
Age distribution of 35 children at the onset of BO.

Clinical presentations in pediatric patients with BO at the time of diagnosis.
Imaging findings at diagnosis
Regardless of age, all patients underwent HRCT. Frequent HRCT findings included the following: mosaic pattern (35/35, 100%; Figure 3(a) and (b)), peribronchial thickening (13/35, 37.1%), atelectasis (13/35, 37.1%; Figure 3(c)), air trapping (11/35, 31.4%), and bronchiectasis (7/35, 20.0%; Figure 3(d)). Most patients exhibited unilateral abnormalities (21/35, 60.0%). Of 15 patients who were oxygen dependent, 3 had mild pulmonary hypertension at diagnosis.
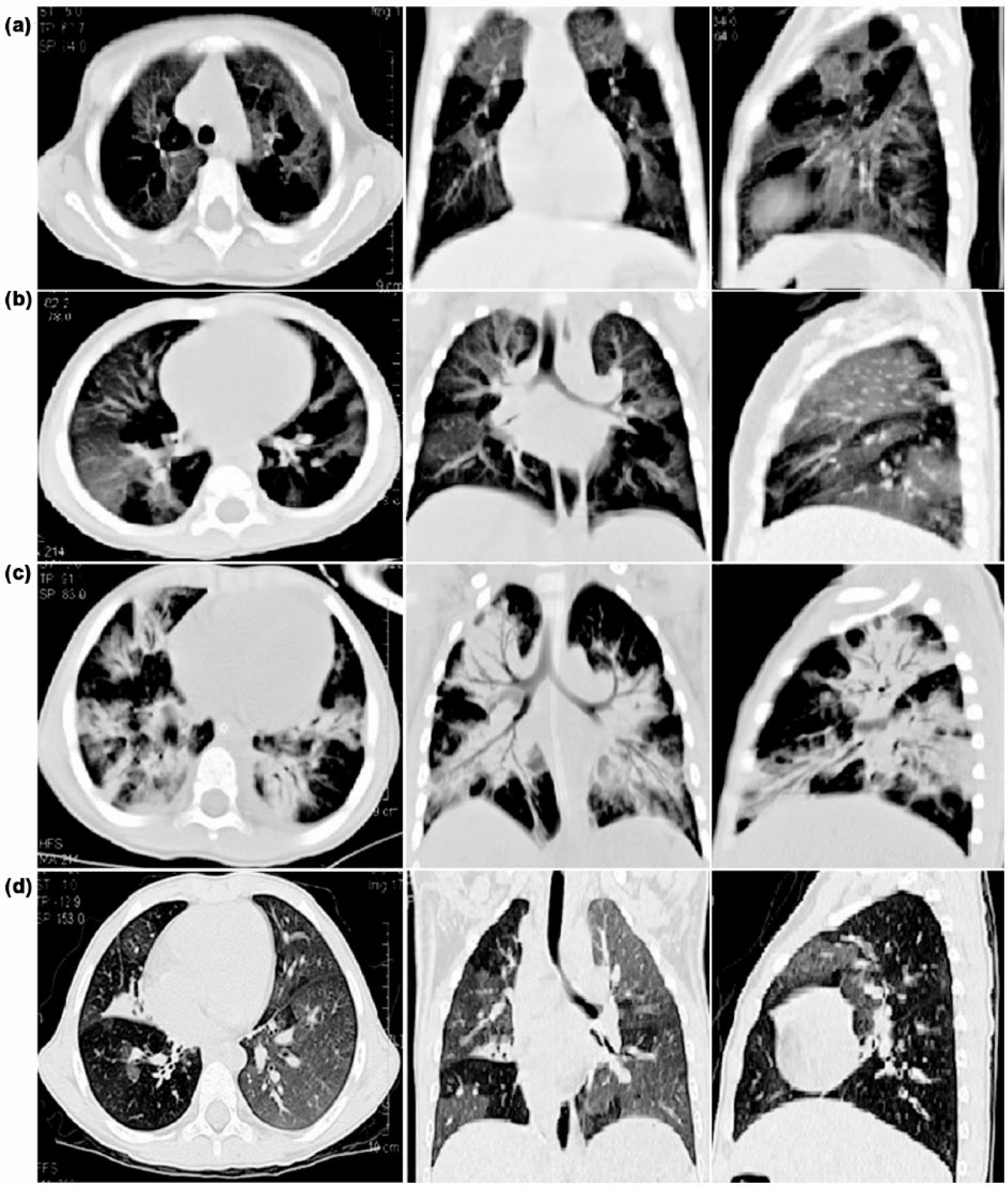
(a) High-resolution CT scan of the chest shows bilateral mosaic ground-glass patterns with air trapping in a 27-month-old child with BO after allogeneic hematopoietic stem cell transplantation. (b) High-resolution CT scan of the chest shows bilateral mosaic ground-glass patterns with air trapping in a 19-month-old child with post-infectious BO. (c) High-resolution CT scan of the chest shows pulmonary atelectasis on both lungs in a 20-month-old child with post-infectious BO. (d) High-resolution CT scan of the chest shows bilateral mosaic ground-glass patterns with air trapping and bronchiectasis at the level of the lower lobes in a 20-month-old child with post-infectious BO.
Hematological findings at diagnosis
Data extracted from the patients at diagnosis included routine blood testing, biochemical parameters, coagulation function, serum immunoglobulin (Ig), and lymphocyte subset results. The most common laboratory observation was leukocytosis (20/35, 57.1%). Serum biochemical examinations showed elevated lactate dehydrogenase levels (18/35, 51.4%) and C-reactive protein levels (17/35, 48.6%). Three patients also exhibited high IgE levels (310–1660 IU/mL). Only one patient exhibited decreased total T- and natural killer (NK)-cell counts.
Histopathological findings
Three patients received lung biopsies. Two of them exhibited an inflammatory process surrounding the lumen of bronchioles and alveolus, which gives rise to scarring and obstruction (Figure 4).

(a) Lung biopsy showed the wall of terminal bronchioles and alveolus stretch, hyperplasia of granulation tissue and focal hemorrhage (HE staining 400×). (b) Lung biopsy showed an inflammatory process surrounding the lumen of terminal bronchioles and a lot of transudate in it (HE staining 200×).
PFT
PFT was performed in 18 of the 35 patients, and the results showed severe and fixed airflow obstruction, decreased compliance, and increased resistance with a slight response to bronchodilators. No significant difference was found between before and after steroid treatment (all P > 0.05, Table 1). The average duration of the treatment is 7.3 months.
Baseline anthropometric and spirometric data.

FVC: forced vital capacity; FEV1: forced expiratory volume in 1 s; PEF: peak expiratory flow rate; VT: tidal volume; TPTEF/TE: ratio of time to reach peak tidal expiratory flow to total expiratory time; VPEF/VE: volume to peak expiratory flow to total expiratory volume; RR: respiratory rate; TEF50: tidal expiratory flow at 50% of tidal volume; TIF: tidal inspiratory flow; PEF: peak expiratory flow; TEF75: tidal expiratory flow at 75% of tidal volume; TEF25: tidal expiratory flow at 25% of tidal volume; FRC: functional residual capacity; Crs/kg: respiratory system compliance per kilogram; Rrs: respiratory system resistance.
Etiology
The predominant cause of BO was post-infectious (32 cases, 91.4%), while only three cases occurred after bone marrow transplantation. Among post-infectious bronchiolitis obliterans (PIBO) patients, the etiology of 30 cases was determined. Adenovirus, Mycoplasma pneumoniae, influenza, and RSV were detected in 50.0% (15/30), 46.7% (14/30), 20.0% (6/30), and 10.0% (3/30) of patients at diagnosis, respectively. Polyinfection was detected in 18 cases (Table 2). Enterococcus faecium, Haemophilus influenzae, Staphylococcus hominis, and Staphylococcus epidermidis comprised the microbiota of patients with BO.
The pathogenies of infection in 30 cases at diagnosis.

Ad: adenovirus; RSV: respiratory syncytial virus; CMV: cytomegalovirus; MP: mycoplasma pneumonia.
Treatment
Treatments varied and were individualized. At the time of diagnosis, 21 patients had oxygen saturation levels below 95%, and 11 had arterial oxygen pressure levels below 60 mmHg and were oxygen dependent. All patients received systemic corticosteroids (methylprednisolone or prednisone) during the acute phase. A total of 11 (11/35, 31.4%) patients required mechanical ventilation because of acute respiratory distress syndrome. Continuous or intermittent home oxygen therapy was prescribed for these seven patients to maintain saturation of peripheral oxygen (SpO2) levels above 90%. Subsequent clinical improvement led to complete weaning of oxygen in most cases for a median period of 3 months. An inhaled corticosteroid (budesonide) was administered to all patients.
Follow-up
The majority of patients improved during follow-up, although some cases had persistent respiratory symptoms. Some patients experienced exacerbated pulmonary conditions during follow-up and required readmission to hospital care. Two patients died as a result of severe pulmonary complications. Both of them had co-morbidities and complications, such as bronchiectasis or lobar collapses, and one also had inherent immunodeficiency.
Discussion
BO is a rare and severe form of chronic lung disease characterized by fixed airway obstruction. BO may occur in a number of forms, such as viral or bacterial infections, gastric content aspiration, inhalation of toxins, collagen diseases, and lung or bone marrow transplant.1,2 Our results showed that the occurrence of BO was greater among male infants and PIBO, especially after severe viral infection, was the most common cause, consistent with previous reports.2–4,6 The majority of our patients showed persistent symptoms and noticeable signs, such as wheezing, tachypnea, and hypoxemia, which are also similar to those reported.2–6 There is no evidence to suggest that BO cases that occur after bone marrow transplantation differ from PIBO though both types of BO exhibit similar clinical presentation. However, the clinical presentation of these patients appeared to be milder and they recover much faster than PIBO patients; thus, the reason is not clear. This may be owing to a different pathogenesis or the application of immunosuppressive therapy. The diagnoses of our cases were mainly made according to clinical and HRCT findings. Clinical and HRCT findings are currently accepted as sufficient data to confirm a diagnosis of BO.2,7,9 Lung biopsy was only performed in three patients in this study. According to previous reports, the absence of characteristic changes in the fragment analyzed does not rule out PIBO, and biopsies may not diagnose PIBO in up to 30% of cases.9,10 Of the three cases that underwent lung biopsy, only two showed consistent BO pathology. One biopsied specimen indicated bronchiolar epithelial inflammation. Therefore, considering the limitations described above and the risks of complications, our results also cast doubt on the effectiveness and need for lung biopsies in the diagnosis of BO.
In this study, viruses were predominantly associated with the development of PIBO. Adenovirus infection was the most common cause of PIBO, followed by influenza. RSV has previously been detected in patients who developed PIBO at an incidence of up to 30%. 11 However, PIBO is considered to be a rare complication of influenza with only a few cases reported in infancy and early childhood. Among our cases, only three patients had RSV infection, while six patients had influenza infection. Potential explanations for these differences may strongly dependent on the prevalent serotype in different regions. Mycoplasma pneumoniae was also a common cause of PIBO in our cohort; however, it was mostly detected as a coinfection with other pathogens. Simultaneous infection by both adenovirus and Mycoplasma pneumoniae was the most common cause of PIBO in this study. Such coinfection appeared to lead to more severe lung damage because it was associated with severe cases and the worst outcomes in our patients. Adenovirus might play a predominant role because only one case with Mycoplasma pneumoniae infection developed PIBO in this study. Nevertheless, we also cannot conclude whether bacterial infection led to PIBO because all bacterial infections were coinfections. One of the patients was diagnosed with primary immunodeficiency disease with severe recurrent symptoms and a poor prognosis. Thus, the exact causes of PIBO are likely heterogeneous and may involve subtle host immune dysregulation, pathogenic factors, or a combination. So, we advise a systematic approach to immunological evaluations in pediatric patients with BO.
HRCT provides information about small bronchial lesions and has sufficient sensitivity to detect airway and parenchymal abnormalities occurring in BO. The most distinctive sign of BO on HRCT is a mosaic perfusion pattern, which is used to differentiate it from other diseases.2,7,12 Some cases exhibited the characteristic mosaic perfusion pattern with disease durations of more than 6 weeks. However, we excluded BO according to respiratory symptoms and radiological status improvement within after therapy. Therefore, we believe that only with typical chest radiographic changes and the duration of more than 6 weeks are not sufficient to diagnose BO. Among our patients, atelectasis was most commonly presented in pre-diagnosis lung imaging. Thus, clinicians must be aware of atelectasis after lung infection and subsequent PIBO. It may be associated with lung sequelae caused by a delayed diagnosis. PFT is an important supplementary tool for the diagnosis and follow-up of patients with BO and can provide information on the functional status of children with BO. 13 The typical spirometry finding in our patients with BO was a severe obstructive disorder with no response to bronchodilators, and no significant difference was found between before and after treatment. It illustrates that BO is a chronic lung disease with irreversible airway obstruction. Some studies have considered that the diagnosis of BO should include not only a suggestive clinical history and abnormal HRCT findings but also evidence of a severe to moderately severe obstructive impairment.14,15 Therefore, they have suggested that children with mild or moderate ventilation disorders should not be diagnosed with BO. We considered that ventilation disorders only reflect disease severity because of some cases with mild ventilation disorders. Further studies are needed to clarify these issues.
Potential risk factors for BO have been described and include adenovirus infection, hospitalization for longer than 30 days, multifocal pneumonia, viral–bacterial coinfection, elevated IgE levels, hypercapnia, and the need for mechanical ventilation.3,9,16–19 A study found that up to 20% of patients had some degree of malnutrition during follow-up and consequently suggested that malnutrition has an impact on the efficiency of respiratory muscles. 1 Two indigenous populations of children in New Zealand and South America were reported to be particularly susceptible to developing PIBO, suggesting that BO may be associated with a genetic predisposition. 20 Therefore, the prognosis of BO is variable and may be associated with multiple factors. We did not compare the patients who died after the treatment with those who are still alive because only two patients died during follow-up. In our study, three cases exhibited high IgE levels and malnutrition at diagnosis. However, none presented with severe respiratory symptoms or a poor prognosis, and in two cases, the serum IgE levels returned to normal during follow-up. Patients with congenital immune deficiency and complication of bronchiectasis exhibited a poor prognosis in this study. Some cases had congenital dysplasia of the larynx (found through laryngoscopes or bronchoscopy) and inspired repeatedly, leading to aspiration pneumonia and persistent and recurrent respiratory symptoms. Perhaps some of the patients were associated with gastroesophagitis reflux disease. We nevertheless did not check whether or not this is the case because our patients were too young. Thus, aspiration pneumonia, which is another aspect of BO management, requires particular attention. Although our study found that mechanical ventilation was a significant risk factor for PIBO, our results did not indicate whether it causes injury to the lung and therefore increases the risk of developing PIBO or merely serves as an indicator of disease severity. Vaccination against potential infectious agents should be a priority in BO including pneumococcal, influenza, and H1N1 vaccines, which are not routinely included in national vaccination programs. In fact, most of our patients could not receive vaccination because of recurrent respiratory symptoms, such as a cough or gasp.
At present, there is no evidence on the efficacy of anti-inflammatory or immunosuppressive agents for controlling BO. Current treatments aim for inflammation control because of the role of the immunological response in the physiopathology of this disease. 20 Some studies have analyzed the role of macrolides in the treatment of BO and showed reduced inflammatory markers in the BAL and improved pulmonary function.6,21,22 In this study, 11 patients received mechanical ventilation in the initial phase. Short- and long-acting bronchodilators, inhaled anticholinergic agents, and systemic corticosteroids were also used during pulmonary exacerbations. Azithromycin and inhaled corticosteroids were used during paracmasis for varying durations. Although pulmonary functional and radiological improvements were not observed, most patients in our study showed clinical improvement during follow-up; oxygen dependence disappeared and pulmonary hypertension was reversed. Such improvement is likely because of the physiologic increase in peripheral airway conductance as a consequence of normal lung growth. Further studies should define the role of corticosteroids and macrolides in inflammation in BO, as well as their capacity to prevent disease progression.
Despite possible ethnic or geographic differences, our study suggested that the clinical, radiological, and functional findings from our pediatric patients were very similar to that in previous reports. The occurrence of BO, especially PIBO, in China is relatively high and might result from primary immunodeficiency diseases in severe cases. Recurrent aspiration pneumonia caused by congenital dysplasia of the larynx and vaccination not on schedule might be potential risk factors for persistent and recurrent BO. Further investigations concerning diagnostic criteria, immunological aspects, and therapeutic approach are needed to improve the prevention and treatment of BO.
Footnotes
Acknowledgements
L.H. and Y.X. contributed equally to this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.