
Abstract
Background:
Idiopathic pulmonary fibrosis (IPF) is a known risk factor for venous thromboembolism (VTE). However, it is currently unknown which factors are associated with an increase of VTE in patients with IPF.
Objectives:
We estimated the incidence of VTE in patients with IPF and identified clinical characteristics related to VTE in patients with IPF.
Design and methods:
De-identified nationwide health claim data from 2011 to 2019 was collected from the Korean Health Insurance Review and Assessment database. Patients with IPF were selected if they had made at least one claim per year under the J84.1 [International Classification of Diseases and Related Health Problems, 10th Revision (ICD-10)] and V236 codes of rare intractable diseases. We defined the presence of VTE as at least one claim of pulmonary embolism and deep vein thrombosis ICD-10 codes.
Results:
The incidence rate per 1000 person-years of VTE was 7.08 (6.44–7.77). Peak incidence rates were noted in the 50–59 years old male and 70–79 years old female groups. Ischemic heart disease, ischemic stroke, and malignancy were associated with VTE in patients with IPF, with an adjusted hazard ratio (aHR) of 1.25 (1.01–1.55), 1.36 (1.04–1.79), and 1.53 (1.17–2.01). The risk for VTE was increased in patients diagnosed with malignancy after IPF diagnosis (aHR = 3.18, 2.47–4.11), especially lung cancer [hazard ratio (HR) = 3.78, 2.90–4.96]. Accompanied VTE was related to more utilization of medical resources.
Conclusion:
Ischemic heart disease, ischemic stroke, and malignancy, especially lung cancer, were related to higher HR for VTE in IPF.
Introduction
Idiopathic pulmonary fibrosis (IPF) is the most common idiopathic interstitial pneumonia. Occurring primarily in older adults and without any known cause, it is characterized by a chronic, progressive, and fibrotic interstitial lung disease. 1
Venous thromboembolism (VTE), which encompasses deep venous thrombosis (DVT) and pulmonary embolism (PE), causes cardiovascular death and disability with a high disease burden.2,3 Previous studies, primarily conducted in Western populations, have illustrated IPF as a risk factor in the development of VTE.4,5 Despite VTE being a more common disease in Western populations than in Asia,2,6 there are not currently any well-designed studies investigating the prevalence and incidence of VTE in Asian patients with IPF. Moreover, little is known about risk factors and the clinical impact of VTE in patients with IPF. Contrastingly, cancer is a common comorbidity in patients with IPF 7 and a well-known risk factor for developing VTE. 8 There is currently no definitive evidence as to how malignancy affects the development of VTE in patients with IPF, especially regarding malignancies other than lung cancer.
Therefore, the aim of the present study was to estimate the incidence of VTE in patients with IPF in data from the Korean Health Insurance Review and Assessment Service (HIRA) database. We also identified clinical characteristics, risk factors, association with cancer, and clinical impacts of VTE in patients with IPF.
Material and methods
Ethics
The Institutional Review Board at Asan Medical Center, Seoul, South Korea, approved this study (No. 2021–0847). Informed consent of the individual patients was waived due to the only use of de-identified data and the retrospective nature of the study.
Data sources
In South Korea, the entire population is covered by the National Health Insurance (NHI) system, in which all health claims data are recorded. Furthermore, the NHI initiated a rare intractable disease (RID) registration program that provides a 90% total payment reduction for patients with RIDs, including IPF. To register into the RID system, patients must meet uniform criteria with physician certification for diagnoses. Each case is subsequently thoroughly reviewed by the NHI system. Therefore, the data in the RID system are considered to be accurate and reliable. These methods were used and validated in several studies using nationwide health claim data in South Korea.9–11
The Health Insurance and Review Agency (HIRA) is a government-affiliated organization whose data are primarily based on the NHI system. We collected de-identified nationwide health claims data from the HIRA database ranging between January 2011 and December 2019. These data included demographic characteristics, both outpatients’ and inpatients’ health service utilization, diagnosis, prescriptions, procedures for diagnoses or treatments, and medical costs.
Study population and design
Between January 2011 and December 2019, patients with IPF were identified from the de-identified health claims database using both the International Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) code of IPF (J84.1) and the RID registration system code of IPF (V236). To ensure the accuracy of the diagnosis, only patients with at least one visit with an IPF-related code within a year were selected.
VTE cases were defined using both the ICD-10 code for VTE, which included codes for DVT and PE, and concurrent medication codes for VTE. The codes for DVT included I80.2 [DVT, not otherwise specified (NOS)] and I80.3 (embolism or thrombosis of the lower extremity, NOS). The codes for PE included I26 (pulmonary thromboembolism), I26.0 (PE with mention of acute cor pulmonale), and I26.9 (PE, NOS). Medication codes for VTE included unfractionated heparin (UFH), low-molecular-weight heparin (LMWH: enoxaparin, dalteparin, and nadroparin), warfarin, and direct oral anticoagulants (DOACs: rivaroxaban, apixaban, edoxaban, and dabigatran).
Individuals who had any diagnostic code for VTE prior to IPF were excluded from the analysis. For each selected patient, demographic characteristics (age and sex), comorbidities [chronic obstructive pulmonary disease (COPD), asthma, diabetes mellitus (DM), hypertension, congestive heart failure, ischemic heart disease (IHD), ischemic stroke, neurodegenerative diseases, chronic liver diseases, chronic kidney disease, lung cancer, and any malignancy other than lung cancer], medication use for IPF (pirfenidone) and VTE (UFH, LMWH, warfarin, and DOAC), and thrombolytic agents (urokinase, streptokinase, and alteplase), procedures for IPF and VTE (mechanical ventilation, thrombectomy, and inferior vena cava filter insertion), use of hospital utilization [hospitalization, emergency room (ER) visit, and intensive care unit (ICU) admission], and the medical costs associated with VTE and IPF were all collected for the analysis. Because nintedanib was not covered by national insurance in South Korea, pirfenidone was only included in this study as antifibrotic agent.
Statistical analysis
Continuous variables are presented as means with standard deviations, or medians with interquartile ranges (IQRs), depending on the distribution of the data. Categorical data are presented as frequencies and percentages. Student’s t-test or Mann–Whitney test was used to assess intergroup differences in continuous variables, and the chi-square test or Fisher’s exact test was used to compare categorical variables.
To estimate the incidence rate, the date of the earliest IPF claim was defined as the index date, and the patient was considered to be an incident case. Thereafter, the incidence rates of VTE were calculated by dividing the number of incident cases by the total observation period. These were then presented as occurrences per 1000 person-years. Patients identified in 2011 were excluded for the clearance period for incident calculation, while patients identified in 2019 were also excluded due to an insufficient follow-up period. Kaplan–Meier curves were used to describe the cumulative incidence for VTE according to age, sex, and malignancy before the log-rank test was used to assess intergroup differences. The Extended Cox regression analysis was implemented to identify the clinical factors associated with the development of VTE in patients with IPF. Any malignancy appearing from the time of the IPF diagnosis was considered as a time-varying variable. The multivariable model included age and sex, alongside the variables from the univariate analysis expressed as p < 0.1. The proportional hazards assumption was checked graphically. p < 0.05 was considered to represent statistical significance. All statistical analyses were performed using the SAS Enterprise Guide software (7.1 version, SAS Institute, Inc., Cary, NC, USA) and R version 3.5.1.
Results
Incidence of VTE in patients with IPF
IPF was identified in 17,012 patients between January 2012 and December 2018. A total of 16,691 patients were included in the final analysis following the exclusion of 321 patients, who had been diagnosed with VTE before IPF. During the follow-up period, 446 (2.7%) patients were diagnosed with VTE (Figure 1).

The overall flow of the study analyses.
The overall incidence rate per 1000 person-years of VTE was 7.08 [95% confidence interval (CI), 6.44–7.77] and it was lower in males (7.07, 95% CI = 6.30–7.90) than females (7.12, 95% CI = 5.98–8.42) (Table 1). With the exception of two cases in the 30–39 years old group, the peak incident rates were noted in the 50–59 years old male (7.89, 95% CI = 5.43–11.08) and the 70–79 years old female groups (9.13, 95% CI = 7.11–11.56). The peak incident rate was noted in the group of 50–59 year olds in the total population study (7.88, 95% CI = 5.87–10.36).
Incidence of venous thromboembolism in Korea idiopathic pulmonary fibrosis patients according to age and sex.

IPF, idiopathic pulmonary fibrosis; VTE, venous thromboembolism.
We presented the number of patients and incidence rate per 1000 person-year with a 95% confidence interval.
Clinical characteristics between with and without VTE
The baseline clinical characteristics of the 16,691 patients are presented in Table 2. There was a mean age of 70.8 ± 9.8 years old, while 4933 (29.6%) patients were identified as females. Compared with patients with IPF without VTE, those with VTE had a lower proportion of DM [7164 (44.1%) versus 165 (37.0%), p = 0.003] and a higher proportion of ischemic strokes [1751 (10.8%) versus 62 (13.9%), p = 0.037]. At the time of IPF diagnosis, 2053 (12.3%) presented malignancies, which was similar in both groups [1987 (12.2%) versus 66. (14.8%), p = 0.104]. Other comorbidities were similar in both groups.
Characteristics of patients with idiopathic pulmonary fibrosis and combined venous thromboembolism.

COPD, chronic obstructive pulmonary disease; IPF, idiopathic pulmonary fibrosis; NTM PD, nontuberculous mycobacteria pulmonary disease; VTE, venous thromboembolism.
Data are presented as number (%) or mean ± standard deviation. Since the cost of pirfenidone has been covered by the National Health Insurance Service in Korea since October 2015, we investigated pirfenidone users in 8653 IPF patients after 2016.
Risk factors for the development of VTE among patients with IPF
Among the identified clinical characteristics, IHD, ischemic stroke, and malignancies were categorized as risk factors for developing VTE in patients with IPF, with an adjusted hazard ratio (aHR) of 1.25 (95% CI, 1.01–1.55), 1.36 (95% CI, 1.04–1.79), and 1.53 (95% CI, 1.17–2.01), respectively (Table 3). Conversely, DM was associated with a lower risk of developing VTE in patients with IPF (aHR, 0.71; 95% CI, 0.59–0.87). The risk for developing VTE was increased in patients previously diagnosed with malignancy after their IPF diagnosis (aHR = 3.18, 95% CI = 2.47–4.11). The cumulative incidence of VTE in patients who had malignancy following an IPF diagnosis was higher than those without, which was also notably higher in patients with lung cancer (Figure 2).
Risk factors for developing venous thromboembolism in patients with idiopathic pulmonary fibrosis.
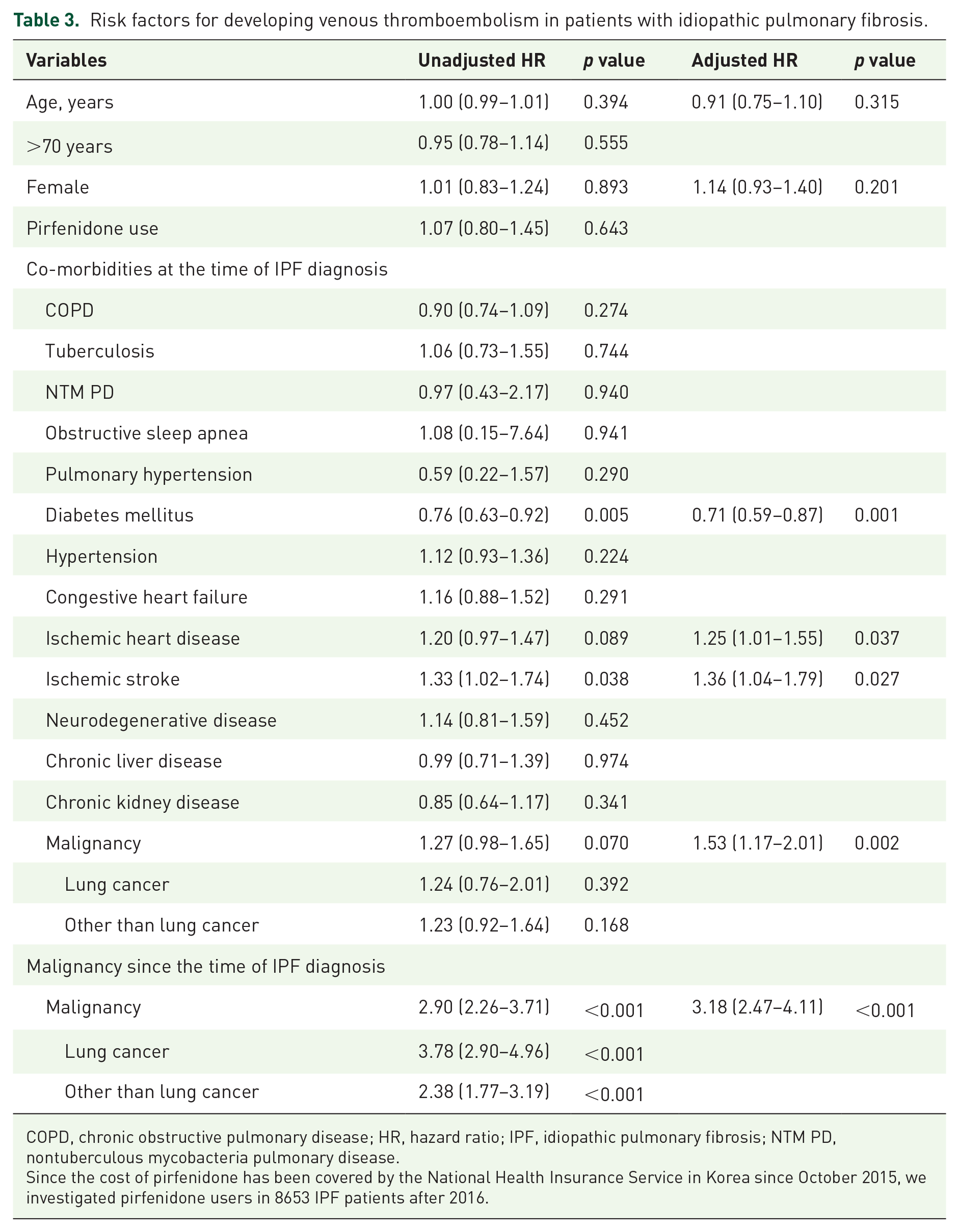
COPD, chronic obstructive pulmonary disease; HR, hazard ratio; IPF, idiopathic pulmonary fibrosis; NTM PD, nontuberculous mycobacteria pulmonary disease.
Since the cost of pirfenidone has been covered by the National Health Insurance Service in Korea since October 2015, we investigated pirfenidone users in 8653 IPF patients after 2016.

The cumulative incidence of VTE were presented in this figure. Patients, who had malignancy following an IPF diagnosis, was higher probability than those without, which was also notably higher in patients with lung cancer. (a) any type of malignancy, (b) lung cancer, and (c) all malignancies except lung cancer.
Treatment modalities for VTE and disease burden
The majority of IPF patients with VTE were treated with anticoagulants including LMWH (49.8%) or DOAC (55.4%) (Table 4). Contrastingly, only a few patients received treatments with thrombolysis (2.0%) or thrombectomy (0.8%). During the study period, the prescription rate of DOAC for VTE treatment in patients with IPF increased, whereas that of warfarin or LMWH decreased (Figure 3).
Treatment for venous thromboembolism in patients with idiopathic pulmonary fibrosis.

DOAC, direct oral anticoagulant; IPF, idiopathic pulmonary fibrosis; LMWH, low-molecular-weight heparin.
Data are presented as numbers (%). Because the cost of pirfenidone has been covered by the National Health Insurance Service in Korea since October 2015, we investigated pirfenidone users in 8653 IPF patients after 2016.

(a) This figure presented the change of using anticoagulants for venous thromboembolism in patients with idiopathic pulmonary fibrosis. (b) The prescription rate of direct oral anticoagulants was increased. Conversely, the rate of low-molecular-weight heparin and warfarin use was decreased.
In patients with VTE, the median (IQR) hospitalization numbers per person, ER visits, and ICU admissions were 5 (3–9), 2 (1–4), and 1 (0–1), respectively, which were significantly higher than patients without VTE (Table 5). Among 446 patients diagnosed with VTE, 74 patients (16.6%) were hospitalized due to VTE during the study periods. VTE also was the cause of ER visits in 55 patients (12.3%) and ICU admissions in 26 patients (5.8%). Moreover, the total medical costs and IPF-related medical costs were also higher in patients with VTE than those without.
Medical resource utilization in patients with idiopathic pulmonary fibrosis according to the diagnosis of venous thromboembolism.
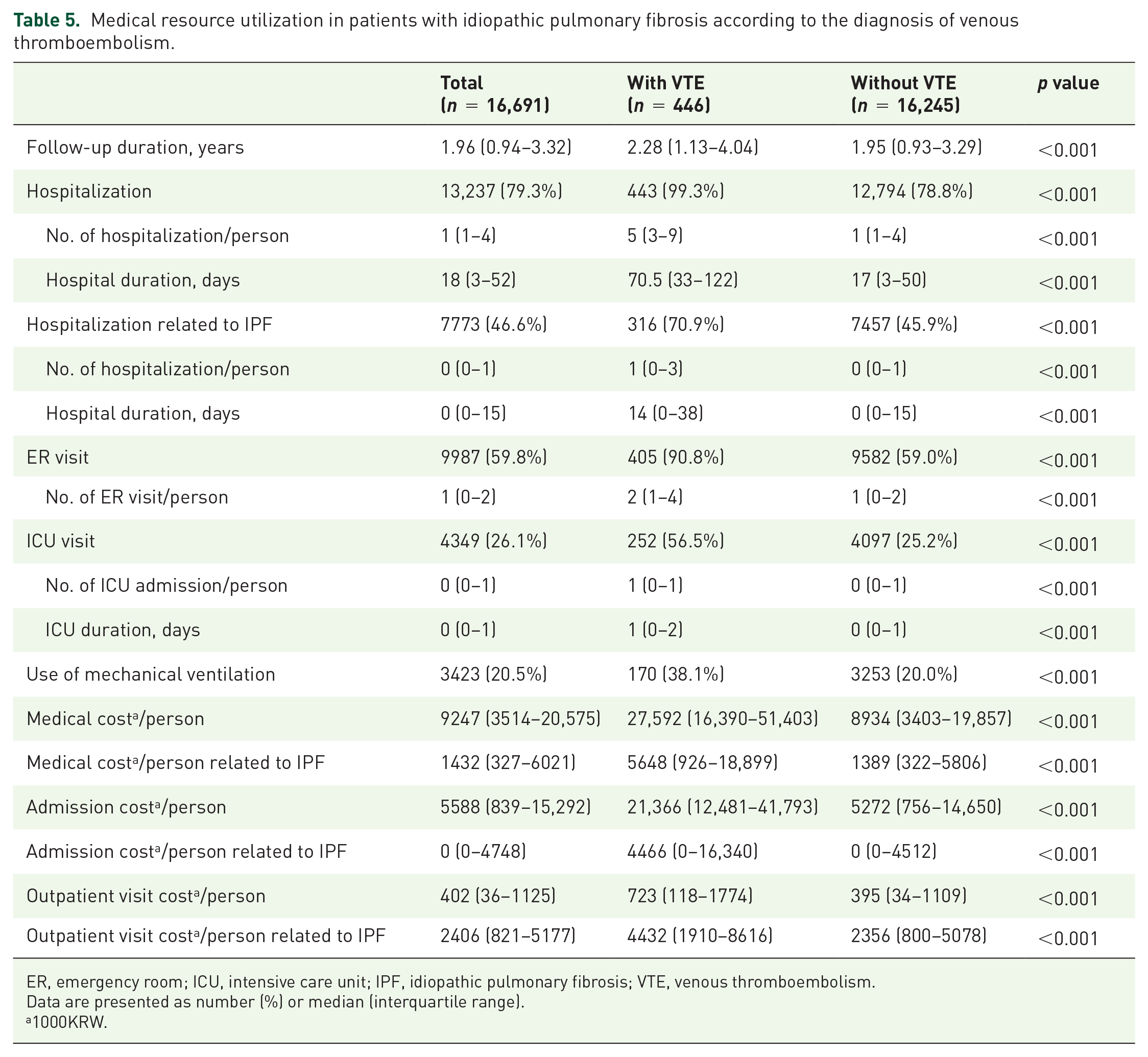
ER, emergency room; ICU, intensive care unit; IPF, idiopathic pulmonary fibrosis; VTE, venous thromboembolism.
Data are presented as number (%) or median (interquartile range).
1000KRW.
Discussion
To our knowledge, there are limited studies regarding VTE in patients with IPF. In the current study, 2.7% of patients with IPF were diagnosed with VTE and received anticoagulant agents. Among various characteristics, former diagnoses of IHD, ischemic stroke, and malignancy were significant risk factors for VTE. Malignancies diagnosed following the IPF diagnosis presented higher HR than any other comorbidities, especially lung cancer. The occurrence of VTE in patients with IPF was associated with increased medical costs and medical resource usage.
In this study, we reported that the prevalence of VTE in patients with IPF was 2.7%. This result correlates with that of previous studies.4,5 Compared with the general population, the prevalence of VTE is increased approximately more than twofold higher in patients with IPF.12,13 In our study, the incidence rate per 1000 person-years of VTE was 7.08 and was not significantly different among all age groups except for the twenties age group. Alternatively, the annual incidence of VTE was reported between 23.9 and 42.2 per 100,000 population in the general population and 101.9 and 151.2 per 100,000 population in the old population (age ⩾60) of South Korea. 14 Considering that the incidence of VTE in the general population increased in the old age group, it was possible that IPF might be a stronger effect on the occurrence of VTE than aging factor. Patients with pulmonary fibrosis exhibited a higher incidence of VTE compared with those suffering from COPD, lung cancer, and in the general population, presenting risk rates of 44%, 54%, and 34%, respectively. 4 Numerous previous studies have reported an increased risk of VTE in patients with IPF. Indeed, Sode et al. 15 identified a 1.8-fold increase in the hazard ratio (HR) for VTE in patients with idiopathic interstitial pneumonia in national Danish registries compared with the respective control group. A meta-analysis similarly presented a 2.11-fold HR (95% CI = 1.28–3.48) for VTE in patients with IPF. 12 Although accurate mechanisms regarding the increased risk of VTE were unclear, IPF was regarded as a hypercoagulable state due to the activated clotting cascade in IPF pathogenesis.16,17 Therefore, it is necessary to monitor the occurrence of VTE in patients with IPF.
Traditionally, there are several risk factors related to developing VTE, including immobilization, malignancy, and trauma.3,18 IPF is also alleged to increase the incidence of VTE;4,5 however, there are only a limited number of studies currently investigating this. In contrast to the general population, old age was not significantly associated with an increased incidence of VTE.18,19 Interestingly, IHD and ischemic stroke were associated with increased aHR for VTE in our study. We hypothesize that this was because two different diseases share many common risk factors.20,21 DM was a well-known risk factor for IHD and ischemic stroke. Yet, the studies investigating the relationship between VTE and DM are rife with controversies.22–24 In our study, DM was the only factor related to a lower risk of VTE in patients with IPF, while the explanation as to why requires further investigation. In a previous nationwide, retrospective, cohort study performed in South Korea, patients with DM undertook an increased use of low-dose aspirins. 25 Thus, increased use of low-dose aspirin in patients with DM might lead to a lower incidence of VTE. To clarify this point, further large-scale investigations are required.
In the current study, malignancy was the crucial risk factor for VTE in patients with IPF after multivariate analysis, regardless of the time of malignancy diagnosis and cancer type. Malignancy is a well-known risk factor for VTE with or without IPF, because malignancy is related to the thrombophilic condition, including hypercoagulable state and accompanying other risk factors.2,26 Since only patients with IPF were included in this study, it is uncertain whether the increased rate of VTE mainly resulted from IPF itself or combined malignancy. However, it was possible that patients with IPF accompanied with malignancy presented a higher risk for VTE than patients with IPF without malignancy. Accompanying lung cancer was the highest risk factor for VTE in our study, which is consistent with several studies in a variety of populations.27–29 IPF is a well-known risk factor for lung cancer.13,30 In addition, other types of cancer are also more common in patients with IPF than in the general population. 7 Therefore, these patients might need to be carefully investigated for VTE.
Although observation periods were longer in patients with VTE, accompanied VTE in patients with IPF was related to more utilization of medical resources in this study. Medical costs associated with VTE were notably increased.31,32 However, adequate treatment of VTE led to a reduction in medical costs. 31 Up until 2016, low-molecular-weight heparin was the predominantly used VTE treatment. However, since then, DOACs have become increasingly popular; a pattern also reported by several other studies.33,34 There was no difference in the pattern of anticoagulants usage according to sex, age, and usage of pirfenidone. Several studies have reported that the use of warfarin could be harmful to patients with IPF.35,36 Therefore, further studies would be required to analyze the optimal treatment strategy and treatment response according to anticoagulants for VTE in patients with IPF.
There were several limitations in this study. First, we defined IPF and VTE based on the ICD-10 code at the time of diagnosis. Although the correlation between actual diagnosis and operational definition using ICD-10 codes is well known, one concern is that the operational definition led to either an overestimation or underestimation of a specific disease. In particular, about 100 patients under the age of 40 were identified as having IPF in the current study. It was possible that some of the patients were misdiagnosed or misclassified as IPF. To overcome this point, attempts were subsequently made to adjust the accuracy of diagnosis by using combined RID code for IPF and prescription of anticoagulants for VTE. Second, the association between accompanied VTE and mortality was not analyzed, because the information about the deaths could not be gathered. Third, the association between severity and exacerbation history of IPF and developing VTE could not be investigated in this study. Patients with severe IPF and a history of exacerbation have an increased chance of developing VTE due to hospitalization. Finally, the causal relationships could not be presented due to the design of the study. We could not investigate the role of IPF itself as VTE-provoking factors, since VTE and IPF share several risk factors. In addition, we did not investigate the effect of drugs, including aspirin and anti-cancer treatment, which might be related to the development of VTE. To overcome this limitation, further prospective studies are required.
In conclusion, we identified a prevalence of 2.7% and that IHD and ischemic stroke might be risk factors for VTE in patients with IPF. In particular, malignancies could be regarded as significant risk factors, irrespective of the time at which it was diagnosed or the cancer type. Therefore, clinicians might be required to closely monitor for VTE in patients with IPF.