
Abstract
Background:
Lung cancer is an important complication of combined pulmonary fibrosis and emphysema (CPFE). Whether the risk of lung cancer is higher in CPFE patients with usual interstitial pneumonia (UIP) than those with idiopathic pulmonary fibrosis (IPF) alone, remains controversial. We conducted this systematic review and meta-analysis to evaluate the prevalence of lung cancer in CPFE patients with UIP compared with IPF patients.
Methods:
We searched the PubMed, Embase, and Cochrane databases for studies that focused on the incidence of lung cancer in CPFE/UIP and IPF groups. We used a fixed-effects model to analyze the odds ratios (ORs) with 95% confidence intervals (CIs) according to data heterogeneity. The cumulative effects based on the publication year and sample size were assessed by cumulative meta-analysis.
Results:
A total of nine studies with 933 patients, including 374 CPFE patients with UIP, fulfilled the inclusion criteria. Overall, CPFE patients with UIP have a higher risk of lung cancer than those with IPF alone (OR = 2.69; 95% CI: 1.78–4.05). There were increased risks of lung cancer in CPFE/UIP patients with the presence of emphysema (OR = 2.93; 95% CI: 1.79–4.79) or emphysema in ⩾10% of the lung volume (OR = 2.22; 95% CI: 1.06–4.68).
Conclusions:
Our systematic review and meta-analysis indicated a significantly higher prevalence of lung cancer in CPFE patients with UIP than in patients with IPF alone.
The reviews of this paper are available via the supplemental material section.
Keywords
Introduction
Combined pulmonary fibrosis and emphysema (CPFE) is a clinical syndrome characterized by the presence of emphysema in the upper lung lobes, and pulmonary fibrosis in the lower lung lobes on chest high-resolution computerized tomography (HRCT). 1 In 2005, CPFE was first defined as a distinct, unrecognized syndrome by Cottin et al., 1 that does not resemble the physiological, radiological, and clinical features of a simple combination of emphysema and pulmonary fibrosis.2,3 Many pulmonary vascular diseases or parenchymal lung diseases have been associated with CPFE; for example, pulmonary hypertension 4 and acute lung injury. 5 It should be noted that, lung cancer, as a complication of idiopathic pulmonary fibrosis (IPF), 6 is also a complication of CPFE patients with poor prognoses. 7 Moreover, the risk of CPFE patients developing lung cancer was higher than those with IPF alone in a number of studies.7–10 The tendency for a CPFE patient to be a heavy smoker or to be older may contribute to this phenomenon, 11 as it has been shown that cigarette smoking and old age are risk factors of lung cancer. 12 However, other studies have found that there is no significant difference in the risk of lung cancer between CPFE patients and patients with IPF alone.13–17 Researchers have suggested that the similarity in pathogenesis in developing lung cancer could lead to the similarity in the incidence of lung cancer between the two distinct diseases, CPFE and IPF alone. 2 In addition, as the prognosis of CPFE patients with usual interstitial pneumonia (UIP) differs to those with other fibrotic patterns on HRCT,15,18 the heterogeneous CPFE diagnostic criteria, especially for different fibrosis patterns, may be another reason for the discrepancies in the reported prevalence of lung cancer between CPFE patients and patients with IPF alone. Therefore, whether CPFE patients are at an increased risk of lung cancer compared with patients with IPF alone remains controversial.
The focus of this systematic review and meta-analysis was to assess whether CPFE patients with UIP were more likely to contract lung cancer than those with IPF alone. As patients with IPF or UIP are involved in most studies focusing on CPFE, 19 the increased risk of developing lung cancer may provide evidence of the different mechanisms between CPFE/UIP and IPF alone for subsequent studies. Future studies that focus on the different mechanisms between CPFE/UIP and IPF diseases that result in lung cancer may be of great value to clinicians. This would allow them to rapidly discriminate between CPFE patients with UIP from those with IPF alone, as well as to conduct routine screening tests for lung cancer on CPFE patients with UIP.
Methods
Selection criteria
The inclusion criteria for this study were as follows: (1) study design: retrospective or cohort studies including CPFE patients with UIP and IPF patients; (2) provided the prevalence of lung cancer in CPFE patients with UIP and IPF patients; (3) confirmed lung cancer by pathological biopsy or surgery; (4) only studies written in English were included.
Based on the diagnostic criteria of CPFE, defined by Cottin et al., 1 patients who met the following criteria were diagnosed with CPFE: (1) the presence of emphysema lesions on chest HRCT, including centrilobular, paraseptal, or mixed emphysema, mainly in the upper lobes; (2) the presence of pulmonary fibrosis on chest HRCT, including reticulations, honeycombing, distortion of lung architecture, and/or bronchiectasis or traction bronchiectasis predominantly in the lower lobes. The diagnosis of IPF and UIP was performed according to the 2011 official ATS/ERS/JRS/ALAT guidelines for the diagnosis and management of IPF. 20 According to these guidelines, which describe the criteria for UIP patterns, the HRCT fibrotic patterns are divided into three subtypes. These are: a UIP pattern, possible UIP pattern, and inconsistencies with a UIP pattern. A UIP pattern and a possible UIP pattern on HRCT were considered as a defined UIP pattern for the diagnosis of IPF if no surgical lung biopsy was performed.
The exclusion criteria were as follows: (1) review articles, case reports, or observational studies without a control group; (2) studies that did not describe the incidence of lung cancer in CPFE patients with UIP or patients with IPF alone; (3) duplicated papers written by the same authors; (4) studies focusing on animals only.
Literature search
Our systematic review and meta-analysis were based on the PRISMA guidelines. 21 Two members of our group (QC and PL) searched the PubMed, Embase, and Cochrane databases for studies that were published from database inception to December 10, 2020, with a systemic literature search strategy that included supplementary data files. The literature search was performed and repeated several times by the two authors in different medical science information centers affiliated to Nanjing Medical University at different times independently. The two investigators viewed abstracts and full texts of the relevant papers in English. In addition, the reference lists of the related articles previously published were considered for an additional literature search.
Data extraction
The two members of our group (QC and PL) carried out data extraction independently. The data of the selected articles, including names of authors, publication year, country or area, design of study, sample size, population of patients with CPFE/UIP, and IPF alone developing lung cancer were reviewed and collected according to the selection criteria above. Only one study was included if the same raw data were published in different papers. We assessed the quality of all selected studies by following the Newcastle-Ottawa Quality Assessment Scale (NOS). 22
Statistical analysis
The Chi–squared test and I–squared test were used to measure the heterogeneity among studies. No significant heterogeneity was noted, according to our study, when p > 0.1 and I2 < 50%. If no significant heterogeneity was determined, the Mantel–Haenszel fixed-effects model was applied for the evaluation of odds ratios (OR) and 95% confidence intervals (CIs) in the meta-analysis; otherwise, a random-effect model was applied. 23 The cumulative effects, based on publication year and sample size, were estimated using cumulative meta-analysis. 24 We assessed publication bias by using funnel plots as a form of qualitative analysis. 25 The Begg rank correlation test (Begg’s Test) and Egger linear regression test (Egger’s Test) were used for the quantitative analysis of publication bias accordingly.26,27 p-values of ⩽0.05 across all tests were considered statistically significant in this study. Statistical analysis was conducted using the software STATA 12.0 (2000; STATA Corp., College Station, Texas, USA).
Results
Characteristics of the studies
A total of nine studies fulfilled the selection criteria and were included in this systematic review and meta-analysis. The characteristics of the nine studies that were included are summarized in Table 1 and Table 2. The PRISMA flow Diagram (Figure 1) shows the process of literature selection and identification. In total, 933 patients, including 374 CPFE patients with UIP and 559 patients with IPF but without emphysema were selected from the studies. The overall incidence of developing lung cancer was 13.7% (128/933), of which the CPFE/UIP group was 22.2% (83/374) and the IPF group was 8.1% (45/559). The publication years of the studies included in this systematic review and meta-analysis ranged from 2014 to 2019. The studies involved in our systematic review and meta-analysis were conducted in different countries; including China, Italy, Japan, Korea, Spain, and Turkey. No significant differences in age were reported in each selected study (Table 2). However, there were more male patients and smokers (with more pack-years) in the CPFE/UIP groups from five studies that we included. In addition, three studies specified the extent of emphysema when defining CPFE with a threshold of 10% lung volume. However, the presence of emphysema, without any specific thresholds, was required as part of the diagnostic criteria of CPFE in the six remaining studies.
The main characteristics of the studies included in this meta-analysis.

CPFE, combined pulmonary fibrosis and emphysema; IPF, idiopathic pulmonary fibrosis; NOS, Newcastle-Ottawa Quality Assessment Scale; UIP, usual interstitial pneumonia.
The demographic characteristics of the patients in the studies we included.
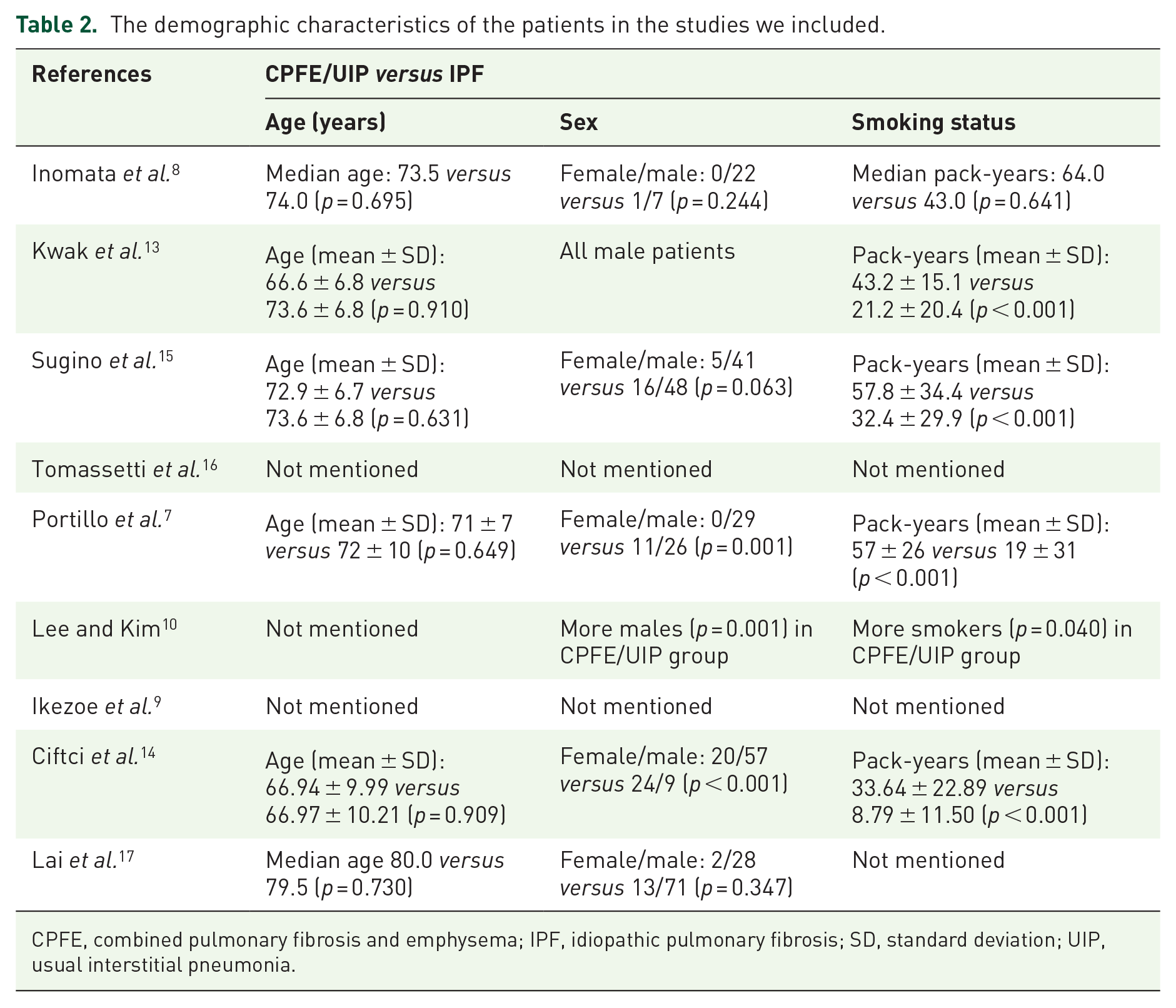
CPFE, combined pulmonary fibrosis and emphysema; IPF, idiopathic pulmonary fibrosis; SD, standard deviation; UIP, usual interstitial pneumonia.
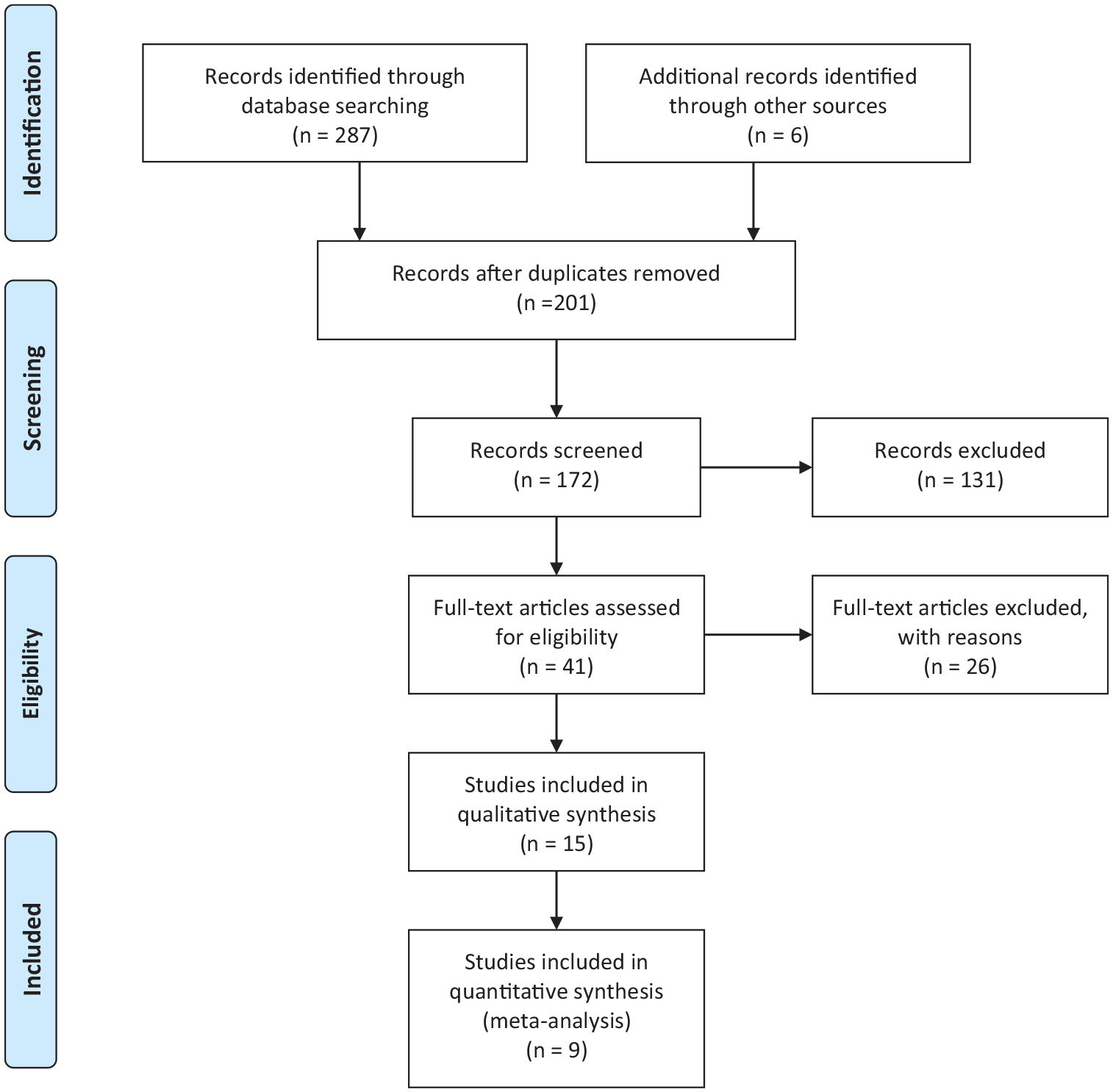
PRISMA 2009 flow diagram.
An increased risk of lung cancer was described by four studies, whereas no significant difference was found by five studies. A total of six studies described the results of pulmonary function testing (PFT) in patents with CPFE/UIP and IPF alone. A general description of the PFT parameters reported in more than three studies is provided in Table 3, including forced vital capacity (FVC; % predicted), forced expiratory volume in one second (FEV1; % predicted), FEV1/FVC ratio, diffusing capacity for carbon monoxide (DLCO; % predicted), and DLCO/alveolar volume (VA) ratio (% predicted). We found that the CPFE patients with UIP had significantly lower FEV1/FVC ratios and DLCO (% predicted) compared with patients with IPF alone in five studies (Table 3).
Pulmonary function testing parameters of the patients from reviewed studies.

Variables are presented as mean ± SD or median (interquartile range).
CPFE, combined pulmonary fibrosis and emphysema; DLCO, diffusing capacity for carbon monoxide; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; IPF, idiopathic pulmonary fibrosis; SD, standard deviation; UIP, usual interstitial pneumonia; VA, alveolar volume.
Subgroup analysis and cumulative meta-analysis
The Mantel–Haenszel fixed-effects model was applied to evaluate OR and 95% CIs due to the low heterogeneity among the studies (p = 0.975, I2 = 0) in this meta-analysis. From the forest plot of the overall meta-analysis, a significant increased risk of lung cancer was observed for the CPFE patients with UIP in comparison to those with IPF alone (Figure 2; OR = 2.69; 95% CI: 1.78–4.05; p < 0.001).

Overall meta-analysis of lung cancer risk in patients with CPFE/UIP and IPF alone.
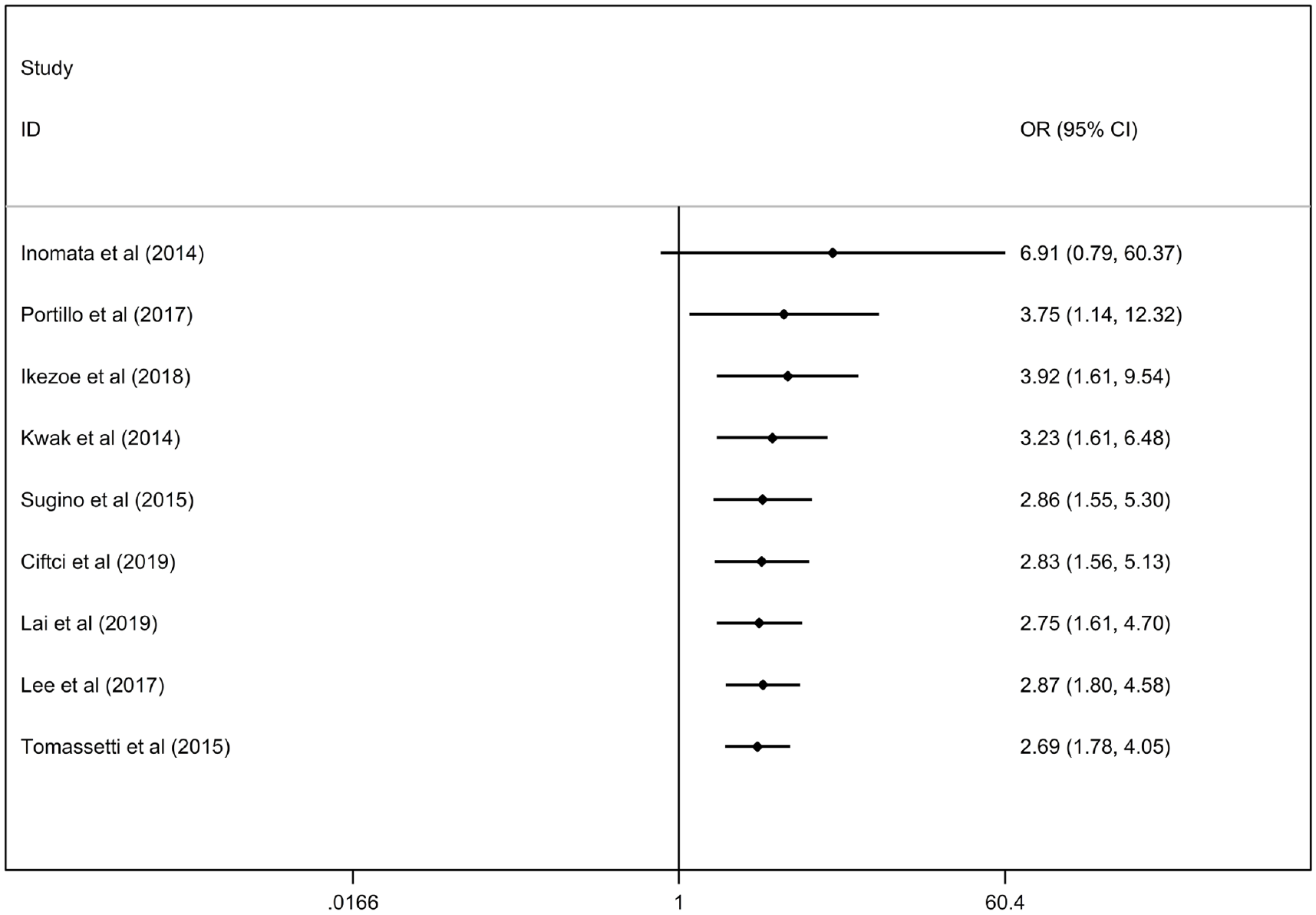
Despite the low heterogeneity (I2 = 0), subgroup analysis was used to compare the extent of emphysema in CPFE patients with UIP; in selected studies, the severity of emphysema was defined by different thresholds (presence of emphysema or ⩾10% lung volume). A significantly higher prevalence of lung cancer was observed in CPFE/UIP patients with the presence of emphysema (OR = 2.93; 95% CI: 1.79–4.79; p < 0.001) or ⩾10% lung volume of emphysema (OR = 2.22; 95% CI: 1.06–4.68; p = 0.035) based on the outcomes of subgroup analysis (Figure 3). Subgroup analysis was performed according to countries, and an increased risk existed in both Asian (OR = 2.94; 95% CI: 1.78–4.86; p < 0.001) and European countries (OR = 2.26; 95% CI: 1.11–4.59; p = 0.024) where the nine included studies conducted (Figure 4). Moreover, a statistically significant increase in the prevalence of lung cancer in CPFE patients with UIP was found since 2014. In addition, a 95% CI in the cumulative meta-analysis remained increasingly stable over the publication duration of the studies (Figure 5). Furthermore, the addition of studies with larger sample sizes from the cumulative meta-analysis did not result in substantive changes in the risk of lung cancer (Figure 6).
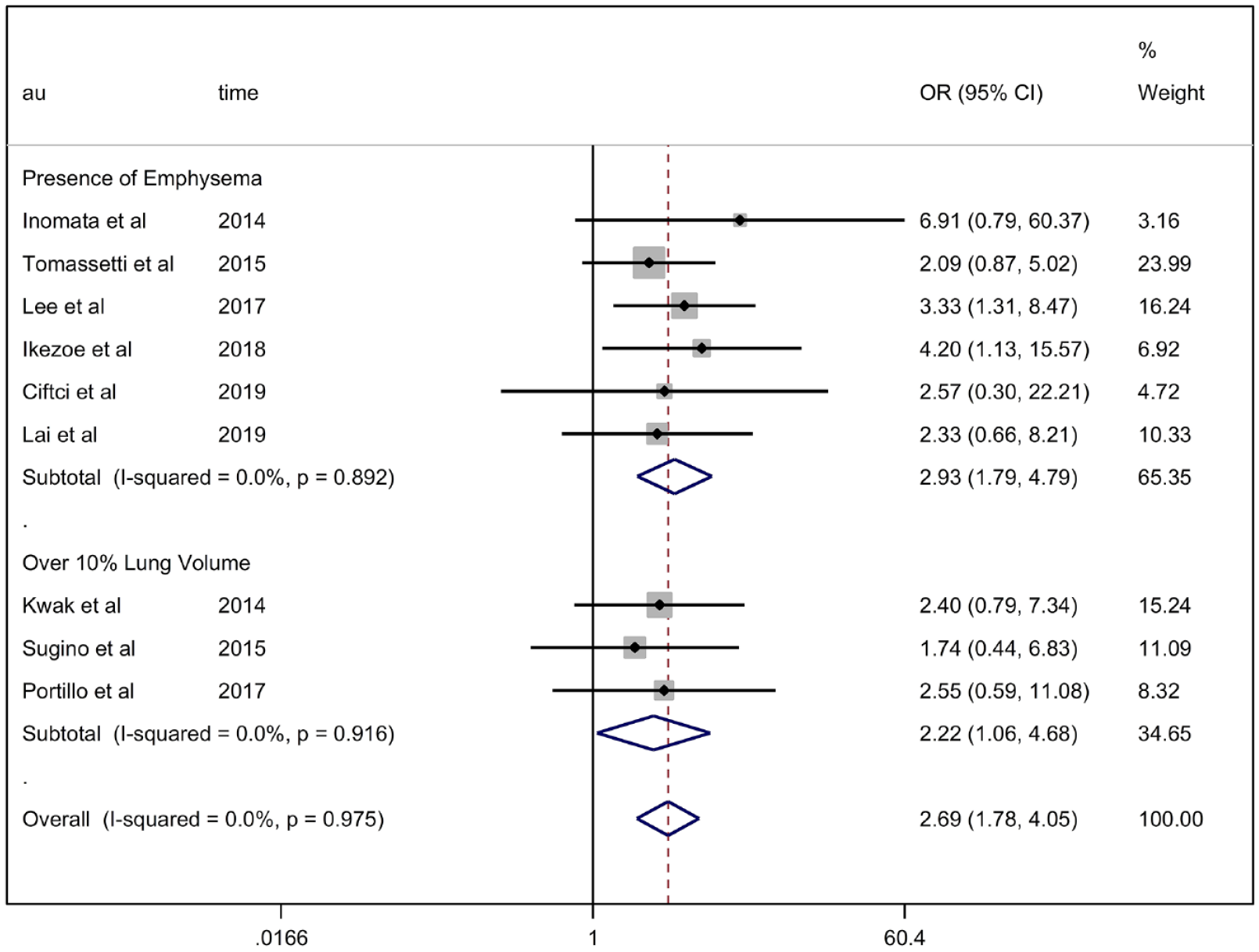
Subgroup meta-analysis of the selected studies based on different thresholds of emphysema extent used for CPFE definition.

Subgroup meta-analysis based on different regions of the included studies.

Cumulative meta-analysis of the included studies based on publication year. The OR (95%CI) values on the figures means the overall OR (95%CI) calculated by the studies on the same row and all the rows above.
Cumulative meta-analysis of the included studies based on sample size. The OR (95%CI) values on the figures means the overall OR (95%CI) calculated by the studies on the same row and all the rows above.
Evaluation of publication bias
We found that there was no publication bias from the funnel plot (Figure 7). In addition, Begg’s Test and Egger’s Test were applied, and the results demonstrated that there was no significant publication bias [Egger’s Test: p = 0.372; 95% CI: −0.90 to 2.11 (Figure 8); Begg’s Test: z = 1.15 <1.96, p = 0.251, continuity corrected (Figure 9)].

Evaluation of publication bias by Funnel plot.
Evaluation of publication bias by Begg’s Test.

Evaluation of publication bias by Egger’s Test.
Discussion
Our systematic review and meta-analysis indicated that a statistically significant higher prevalence of lung cancer existed in CPFE patients with UIP, compared with those with IPF alone. To the best of our knowledge, this is the first meta-analysis to examine the risks of lung cancer in CPFE patients with UIP, although two meta-analysis studies described the clinical features or prognosis of CPFE in lung cancer patients in comparison with the result to patients without CPFE.28,29 In the current review, the risks of lung cancer for CPFE patients with UIP were 2.69 times higher than for patients with IPF alone (OR = 2.69; 95% CI: 1.78–4.05; p < 0.001), where no significant changes occurred in the cumulative analysis.
After reviewing the CPFE studies and other CPFE-related studies during data extraction, we noted that different selection criteria were utilized for CPFE patients, including varied types of intestinal lung diseases or thresholds of emphysema. It should be noted that a systematic review published in 2020 found that approximately half of CPFE-related studies (34 studies, 47%) required a diagnosis of IPF for CPFE patients. 19 Therefore, we only included CPFE patients with pulmonary fibrosis of UIP subtype in our meta-analysis and performed a subgroup analysis for different emphysema thresholds. Subgroup analysis demonstrated that an increased risk of lung cancer still existed in CPFE patients with different emphysema thresholds (presence of emphysema or ⩾10% lung volume).
Hypotheses were formulated to explain the higher risks of lung cancer for CPFE patients. Firstly, CPFE, as one of the smoking-related lung diseases, rather than pulmonary fibrosis alone, was more likely to occur in heavy smokers and males,30,31 who were susceptible to lung cancer, especially squamous cell carcinoma. 12 In addition, squamous cell carcinoma was reported to be the most frequent histological subtype of lung cancer in CPFE patients. 28 In our systematic review and meta-analysis, five studies also found that CPFE patients with UIP tended to be heavy smokers compared with IPF-alone patients. Besides cigarette smoking, it has been shown that radiographic emphysema, per se, is independently-associated with lung cancer development.32,33 Therefore, compared with patients with IPF alone, it seems reasonable to attribute the higher frequency of lung cancer in CPFE patients to the combined effects of emphysema and fibrosis in carcinogenesis. However, it remains unknown whether the increased risk of lung cancer in CPFE patients results from more than the sum of its parts (emphysema and pulmonary fibrosis) or just a simple sum of its parts. Additional precise statistic models are required to calculate and compare the influences on lung cancer development in CPFE patients. Bioinformatic analysis and whole-genome microarray sequencing revealed that there were significant differences in gene expression between the fibrotic and emphysematous lesions in CPFE patients with lung cancer, 34 which might explain the genetic mechanisms behind CPFE patients developing lung cancer. Additional studies, focusing on the molecular mechanisms of lung cancer in CPFE patients, are urgently required in this area. However, as previously noted, a lack of official CPFE identification and classification guidelines are major obstacles in furthering biological and clinical studies. 19 Of course, we cannot ignore the fact that the prevalence of CPFE in patients with emphysema or pulmonary fibrosis was not very low (range, 18.8% to 50.9%), 35 and CPFE patients with UIP were at an increased risk of lung cancer as demonstrated in our meta-analysis. Overall, considering the prevalence and serious complications associated with a poor prognosis of CPFE, it is necessary to make a concerted effort to formulate official CPFE guidelines in the future.
There are some limitations in this systematic review and meta-analysis. Firstly, the sample size of each study we included was not very large. Secondly, no acknowledged diagnostic criteria of CPFE have been established until now, although all CPFE patients in the selected studies were diagnosed according to the initial definitions proposed by Cottin et al. 1 The unstandardized criteria of CPFE, including different emphysema thresholds, may contribute to undue diagnosis or less sensitivity for CPFE. In addition, we only included CPFE patients with UIP, and did not focus on the risks of lung cancer in CPFE patents with other subtypes of pulmonary fibrosis. Lastly, it is possible that the inclusion of papers written only in English may result in a statistic bias.
Conclusions
In conclusion, our systematic review and meta-analysis indicated a significantly higher prevalence of lung cancer in CPFE patients with UIP than those with IPF alone for the first time. Additional multi-center or prospective research should be conducted in the future.
Supplemental Material
sj-pdf-1-tar-10.1177_17534666211017050 – Supplemental material for An increased risk of lung cancer in combined pulmonary fibrosis and emphysema patients with usual interstitial pneumonia compared with patients with idiopathic pulmonary fibrosis alone: a systematic review and meta-analysis
Supplemental material, sj-pdf-1-tar-10.1177_17534666211017050 for An increased risk of lung cancer in combined pulmonary fibrosis and emphysema patients with usual interstitial pneumonia compared with patients with idiopathic pulmonary fibrosis alone: a systematic review and meta-analysis by Qianqian Chen, Ping Liu, Hong Zhou, Hui Kong and Weiping Xie in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-2-tar-10.1177_17534666211017050 – Supplemental material for An increased risk of lung cancer in combined pulmonary fibrosis and emphysema patients with usual interstitial pneumonia compared with patients with idiopathic pulmonary fibrosis alone: a systematic review and meta-analysis
Supplemental material, sj-pdf-2-tar-10.1177_17534666211017050 for An increased risk of lung cancer in combined pulmonary fibrosis and emphysema patients with usual interstitial pneumonia compared with patients with idiopathic pulmonary fibrosis alone: a systematic review and meta-analysis by Qianqian Chen, Ping Liu, Hong Zhou, Hui Kong and Weiping Xie in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-3-tar-10.1177_17534666211017050 – Supplemental material for An increased risk of lung cancer in combined pulmonary fibrosis and emphysema patients with usual interstitial pneumonia compared with patients with idiopathic pulmonary fibrosis alone: a systematic review and meta-analysis
Supplemental material, sj-pdf-3-tar-10.1177_17534666211017050 for An increased risk of lung cancer in combined pulmonary fibrosis and emphysema patients with usual interstitial pneumonia compared with patients with idiopathic pulmonary fibrosis alone: a systematic review and meta-analysis by Qianqian Chen, Ping Liu, Hong Zhou, Hui Kong and Weiping Xie in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-4-tar-10.1177_17534666211017050 – Supplemental material for An increased risk of lung cancer in combined pulmonary fibrosis and emphysema patients with usual interstitial pneumonia compared with patients with idiopathic pulmonary fibrosis alone: a systematic review and meta-analysis
Supplemental material, sj-pdf-4-tar-10.1177_17534666211017050 for An increased risk of lung cancer in combined pulmonary fibrosis and emphysema patients with usual interstitial pneumonia compared with patients with idiopathic pulmonary fibrosis alone: a systematic review and meta-analysis by Qianqian Chen, Ping Liu, Hong Zhou, Hui Kong and Weiping Xie in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
Author contributions
WX and HK contributed to this work equally. WX and HK were responsible for conceptualization, funding acquisition, project administration, supervision, writing-review, and editing. QC was involved in the investigation and writing of the original draft. QC and PL were involved in data curation, formal analysis, writing-review, and editing. HZ contributed to the methodology and writing of the original draft. PL and HZ were responsible for the software application.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Foundation of China (NSFC) [grant number 81870054] and Key Project of National Science & Technology for Infectious Diseases of China [grant number 2018ZX10722301-002].
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.