
Abstract
Background and objective:
The global prevalence and incidence of nontuberculous mycobacterial (NTM) infections are increasing; however, population-level data on healthcare use and medical costs for people with NTM infections are limited. Thus, we investigated the rates of healthcare use and medical costs of people with NTM infections in South Korea using the National Health Insurance Service-National Sample Cohort from 2002 to 2015.
Methods:
In this cohort study, people with and without NTM infection aged 20–89 years were matched 1 to 4 by sex, age, Charlson comorbidity index, and year of diagnosis. The overall and annual average healthcare use and medical costs were calculated. In addition, trends in healthcare use and medical costs for each of the 3 years before and after NTM diagnosis were investigated for people diagnosed with NTM infection.
Results:
A total of 798 individuals (336 men and 462 women) diagnosed with NTM infection and 3192 controls were included in the study. NTM-infected patients had significantly higher rates of healthcare use and medical costs than those in the control group (p < 0.05). NTM-infected patients showed 1.5 times the medical cost and 4.5 times the respiratory disease cost of the control group. People diagnosed with NTM infection incurred the highest medical costs in the 6 months before diagnosis.
Conclusion:
NTM infection increases the economic burden on Korean adults. Appropriate diagnostic tests and treatment plans for NTM infections are needed to reduce the burden of the disease caused by such infection.
Introduction
Nontuberculous mycobacteria (NTM) are a group of more than 200 species of environmental mycobacteria found in a wide range of sources in our daily lives (e.g. soil, dust, and water). 1 While exposure to NTM is generally harmless and can naturally be resolved through the human immune system, opportunistic infections from a small number of NTM can cause debilitating illnesses in humans, primarily involving the lungs. 2 One such disease is nontuberculous mycobacterial pulmonary disease (NTM-PD). NTM-PD is most common in patients with an already weakened immunity and pre-existing lung diseases, such as bronchiectasis, 3 chronic obstructive pulmonary disease (COPD), asthma, 4 and lung cancer. 5 Thus, patients with NTM infections often experience aggravation of respiratory symptoms that can require emergency care.
In many countries, the increasing prevalence6–8 of NTM-PD is an emerging public health concern. NTM-PD is of particular interest to public health professionals, as its diagnosis is difficult and requires lengthy and multiple processes that involve the evaluation of symptoms, the interpretation of radiographic findings, and microbiological confirmation through repeated laboratory tests.2,9 Furthermore, NTM-PD treatments typically involve species-specific multi-antibiotic therapies lasting more than 12 months,10,11 and these lengthy antibiotic therapies do not typically result in curing the disease, thus indicating the need for chronic disease management. For instance, the treatment success rate for patients with Mycobacterium avium complex is approximately 60%, 12 while success rates for the treatment of Mycobacterium abscessus stand around 30% or less. 13 Finally, the chronic nature of the disease progression and management is associated with high medical expenses and financial burden for patients with NTM-PD.14,15 Despite the emerging public health significance of NTM-PD and its implications for healthcare costs, only a limited number of studies examining the costs and financial burden of NTM-PD have been published.14–17
In South Korea, the age-adjusted prevalence of NTM infection between 2003 and 2017 increased nearly 30-fold to 1.2 per 100,000 and 33.3 per 100,000. 8 However, no study has assessed the trends in healthcare costs associated with the growing burden of NTM infections in Korea. The objective of the current study was to estimate the economic burden associated with NTM infection in Korea by focusing on healthcare use and medical costs.
Methods
Data source
This study used data from the National Health Insurance Service-National Sample Cohort (NHIS-NSC) 2.0 database of the NHIS, a compulsory single-payer national healthcare coverage system in South Korea. The NHIS-NSC is a large-scale population-based cohort comprising a representative sample of approximately 2% (1,000,000 people) of the general Korean population from 2002 to 2015. The database contains a de-identified research dataset that includes demographic information, disease diagnosis, therapeutic procedures, and drug prescriptions for participants. A more detailed description of NHIS-NSCs has been reported in another study. 18
Study population
To investigate the cost of NTM infection using the NHIS-NSC 2.0, we first used the NHIS-NSC 2.0 database to identify patients diagnosed with NTM infection between 2002 and 2015. Figure 1 shows the selection process of the study population. Individuals with two or more claims associated with NTM infection [International Classification of Diseases, 10th Revision (ICD-10) A31] between January 2002 and December 2015 were identified (n = 1243). Among these individuals, we excluded nine patients with a history of NTM infection in 2002 to ensure the inclusion of only patients with newly developed NTM infections. In addition, we limited the study subjects to adults, excluding those below the age of 20 years because there may be differences between adults and children in disease pattern, treatment, and medical cost system (n = 108). Also, since there was only one person above the age of 90 years, that person was excluded. Finally, people who died before the index date were excluded (n = 327).

Flow diagram of the study population.
The selected patients with NTM infections were matched by sex, age, and Charlson comorbidity index (CCI) in the year of the index date with four controls who had no claims related to NTM infection between 2002 and 2015, using propensity score (PS) matching. PS matching reduced potential confounding factors and balanced the baseline covariates of the two groups. 19 PSs were derived from the predicted probability of patients with NTM infection versus those without NTM infection using a logistic regression model adjusted for confounding by age, sex, CCI scores, and index year. To reduce misclassification of exposure time (thereby misrepresenting cumulative medical care costs in the control group), time zero to track medical care costs in the control group was aligned to the index dates of the matching people with NTM infection. 20 A total of 798 patients with NTM infection and 3192 matched controls were included in this matched cohort study. To investigate trends in healthcare use and medical costs before and after the diagnosis of NTM infection, a subgroup of patients diagnosed with NTM infection between 2011 and 2012 (n = 189) and matched controls (n = 756) were selected.
Outcomes and other variables
We compared the healthcare use (frequency of outpatient department visits and inpatient hospitalizations) and medical costs (outpatient and inpatient costs) of people with NTM infection to those without NTM infection. We also investigated the healthcare use and medical costs related to respiratory diseases (RDs), the most common comorbidity in people with NTM infection.21,22 RD was defined as having two or more ICD-10 claims for asthma (J45–J46), bronchiectasis (J47), and COPD (J42–J44). Other comorbidities of interest, hypertension (I10–I15), diabetes (E10–E14), gastroesophageal reflux disease (GERD; K21), and cancer (all C-codes) were considered as covariates. First, we calculated the total healthcare use and medical costs over the entire follow-up period. Second, we calculated the average annual healthcare use and medical costs by considering the follow-up period. In addition, we calculated healthcare use and medical costs every 6 months for each of the 3 years before and after the index date. Medical costs included all costs related to diagnostic tests, procedures, and treatments covered by the NHIS. 23
Participants were classified into seven age groups (20–29, 30–39, 40–49, 50–59, 60–69, 70–79, and 80–89 years) to compare the risk of mortality by age group of 10 years old. The NHIS database initially classified participants into 11 classes based on income (with class 0 indicating the lowest income group and class 10 indicating the highest income group). Because the income classification was too detailed, we re-categorized these classes into three groups with reference to previous studies (low income, classes 0–2; medium income, classes 3–7; high income, classes 8–10). The regions of residence were categorized into urban (Seoul, Busan, Daegu, Incheon, Gwangju, Daejeon, and Ulsan) and rural (Gyeonggi, Gangwon, Chungcheongbuk, Chungcheongnam, Jeollabuk, Jeollanam, Gyeongsangbuk, Gyeongsangnam, and Jeju) taking into account regional characteristics. CCI scores were divided into four groups (0, 1, 2, 3, or higher) considering the CCI score distribution of the subject.
Statistical analysis
Categorical variables were reported as frequencies and percentages. For descriptive analyses, the mean (M), standard deviation (SD), 95% confidence interval (CI), median, and interquartile range (IQR) were reported for all continuous variables. To compare patients with NTM infection and matched controls, appropriate univariate tests (i.e. a chi-square test of independence for categorical variables and Wilcoxon–Mann–Whitney test for continuous variables) were used. All costs in the study are expressed as recorded between 2002 and 2015 and have been converted to US dollars (USD), with a conversion rate of 1260.6 won per USD, based on the exchange rate as of June 3, 2022. All analyses were performed using the SAS Enterprise Guide 7.1 (SAS Institute Inc., Cary, NC, USA). Statistical significance was defined as a two-sided p value of < 0.05.
Results
Baseline characteristics
The baseline characteristics of the study population are shown in Table 1. In total, 798 patients with NTM infection (Mage = 56.0 years) and 3192 controls (Mage = 55.7 years) were included. The mean follow-up period was 3.6 years. Among the patients with NTM infection, 336 (42.1%) were men and 462 (57.9%) were women. In both the patient and control groups, the 60–69 years age group accounted for the largest proportion of participants, followed by the 70–79 years age group. The difference in income levels between people with and without NTM infection was statistically significant, but income information for 693 people in the control group was missing.
Baseline characteristics of the study population after propensity score matching.

CCI, Charlson Comorbidity Index; COPD, chronic obstructive pulmonary disease; GERD, gastroesophageal reflux disease; NTM, nontuberculous mycobacteria infection. Data are presented as mean ± standard deviation or mean and percent (%).
An independent t test for continuous variables and the chi-square test for categorical variables were used.
Income was divided into 11 classes (class 1, lowest income; class 11, highest income), which were reclassified into three groups (low, classes 1–3; medium, classes 4–8; high, classes 9–11). In people without NTM, income information was missing for 693 cases (n = 2499).
Region of residence was categorized into urban (Seoul, Busan, Daegu, Incheon, Gwangju, Daejeon, and Ulsan) and rural (Gyeonggi, Gangwon, Chungcheongbuk, Chungcheongnam, Jeollabuk, Jeollanam, Gyeongsangbuk, Gyeongsangnam, and Jeju).
Since the participants were matched by sex, age, and CCI score, there was no significant difference in terms of these characteristics between people with and without NTM infection. However, when looking at the prevalence of comorbidities individually, the rates of asthma (47.1% versus 13.2%), bronchiectasis (28.8% versus 2.0%), COPD (38.6% versus 18.2%), GERD (64.7% versus 52.8%), and cancer (20.4% versus 14.3%) were significantly higher in people with NTM than in those without NTM infection (p < 0.0001 for all). In contrast, hypertension (40.1% versus 49.4%) and diabetes mellitus (27.8% versus 33.8%) were significantly lower in patients with NTM infection than in those without NTM infection (p < 0.01 for all).
Healthcare use and medical costs in the entire follow-up period
People with NTM infection had significantly higher rates of healthcare use and medical costs than those without NTM infection (p < 0.05) (Table 2). The number of inpatient visits (2.44 versus 2.18) and outpatient visits (97.98 versus 87.46) was greater for people with NTM infection than in those without NTM infection (p < 0.0001 for all). The number of inpatient visits (1.00 versus 0.32) and outpatient visits (13.50 versus 4.29) due to RD was also greater in those diagnosed with NTM than in the control group (p < 0.0001 for all). The total number of inpatient and outpatient visits in the patient group was 1.1 times that of the control group, and the number of inpatient and outpatient visits due to RD was 3 times that of the control group.
Healthcare use and medical costs of people with and without NTM.
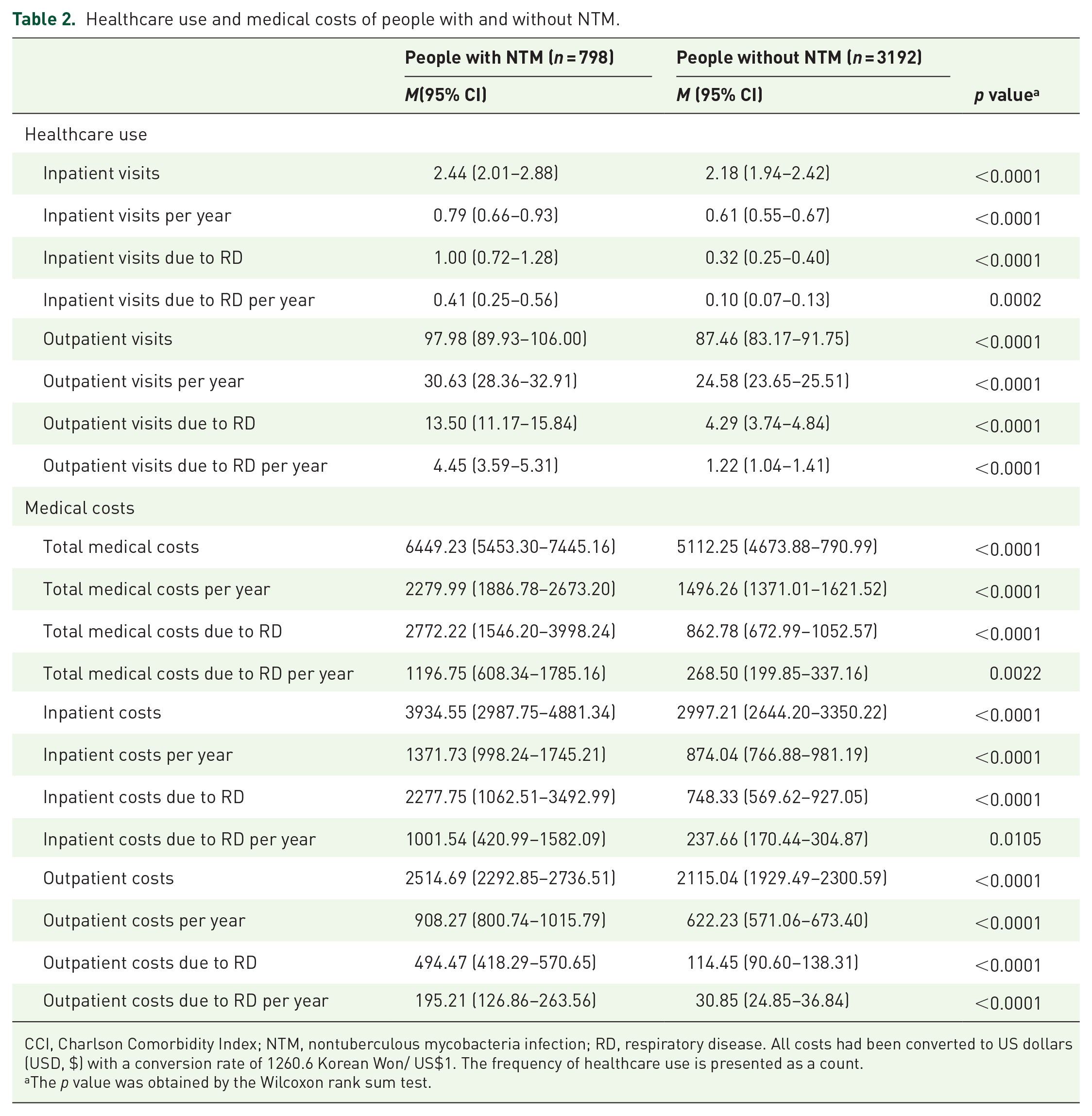
CCI, Charlson Comorbidity Index; NTM, nontuberculous mycobacteria infection; RD, respiratory disease. All costs had been converted to US dollars (USD, $) with a conversion rate of 1260.6 Korean Won/ US$1. The frequency of healthcare use is presented as a count.
The p value was obtained by the Wilcoxon rank sum test.
The total medical costs during the entire follow-up period for people with and without NTM infection were US$6449.23 and US$5112.25, respectively. When the inpatient and outpatient costs were divided, the inpatient costs were significantly higher than the outpatient costs in people diagnosed with and without NTM infection. The costs for the people with NTM infection were significantly greater than those for the control group for both inpatient (US$3934.55 versus US$2997.21) and outpatient costs (US$2514.69 versus US$2115.04) (p < 0.0001 for all). Both inpatient (US$2777.75 versus US$748.33) and outpatient costs (US$494.47 versus US$114.45) due to RD were also significantly greater for NTM patients than those in the control group (p < 0.0001 for all). The cost of RD for people with NTM infection was approximately 3.2 times that of the control group (Table 2 and Figure 2).

Medical costs of people with and without NTM infection.
In people with NTM infection, the inpatient cost was 1.6 times that of the outpatient cost, and 58% of the inpatient cost was hospitalization due to RD. The inpatient cost of the control group was 1.4 times the outpatient cost, and the inpatient cost due to RD accounted for 25% of the total inpatient cost.
When we calculated the average cost per year considering the follow-up period of the individuals, the average medical costs per year were 1.5 times higher for people with NTM infection than those without NTM infection (US$2279.99 versus US$1496.26, p < 0.0001) (Figure 3). The average medical cost due to RD per year was 4.5 times higher for people with NTM infection than those without NTM infection (US$1196.75 versus US$268.50, p = 0.0022). For both people with and without NTM infection, the inpatient costs per year were significantly higher than the outpatient costs per year (p < 0.0001). The inpatient cost per year for people with NTM infection accounted for 60% of the total medical cost per year (US$1371.73), and the inpatient cost of the control group accounted for 58% of the total medical cost per year (US$874.04). The annual costs due to RD accounted for approximately 52% of the total medical cost per year (US$1196.75) in people with NTM infection and 18% of the total medical cost per year (US$268.50) in people without NTM infection.

Average medical costs per 1 year for people with and without NTM infection.
Healthcare use and cost for the previous 3 years and the following 3 years from the index date
Figure 4 shows the medical costs of people diagnosed with NTM infection in 2011 and 2012 compared to those without NTM infection for 3 years before and 3 years after the date of diagnosis.

(a) Total medical costs and (b) medical costs due to RD for each 3 years before and after the index date for people with and without NTM infection.
There was no significant difference in the total healthcare use and cost for those diagnosed with and without NTM infection between 12 and 36 months before the index date (Additional File 1: Table 1). However, healthcare use and costs due to RD among those diagnosed with NTM infection were higher than those of the control group from 30 to 36 months before NTM infection was diagnosed. During the 12 months prior to being diagnosed with NTM infection, the level of healthcare use and medical costs of participants was significantly higher than in those without NTM infection. In particular, the total medical cost for those diagnosed with NTM infection in the 6 months prior to being diagnosed with NTM infection was about 2.1 times that of those without NTM infection, and the cost of RD was approximately 7.8 times that of those without such infection.
Even after the index date, those diagnosed with NTM infection had significantly higher total medical costs than those without NTM infection (Additional File 1: Table 2). In particular, the cost of RD was consistently higher for those diagnosed with NTM infections than for those without.
Discussion
This study compared healthcare use and medical costs for individuals with and without a diagnosis of NTM infection. This study found that people who were diagnosed with NTM infection had higher medical costs starting from the year before they were diagnosed with NTM infection than those who did not. The average medical costs per year for those with NTM infection were 1.5 times that of those without NTM infection, and the average medical costs of RD per year were 4.5 times that of those without NTM infection.
Other countries have published studies comparing healthcare use and costs of people with and without NTM infections.14,15,17 A matched cohort study of 91 people who received a prolonged regimen (>1-month duration) of antimicrobial therapy in Ontario, Canada, from September 2003 to October 2008 found that people with NTM infection and NTM-related RD had higher medical costs than those without. 15 Furthermore, in a study conducted in Germany using a sample of 7,073,357 anonymized persons covered by German public statutory health insurances, 125 patients with newly diagnosed NTM-PD in 2010 and 2011 were matched with 1250 control patients by age, sex, and CCI. In that study, the mean direct expenditure of patients with NTM-PD was nearly four times higher than that of the matched normal control group. 14 In addition, the inpatient costs were approximately three times higher in the NTM-PD group than in the control group, accounting for 63% of the total medical costs.
Another matched cohort study (1039 people with NTM-PD and 2078 people without NTM-PD) in the United States investigated healthcare use and standardized healthcare expenditures for 12 months prior to NTM-PD diagnosis (year 1) and 2 years thereafter (year 2). 17 The average healthcare cost in year 1 was US$72,475 [95% CI (US$58,510–US$86,440)] for patients with NTM-PD and US$28,405 [95% CI (US$8859–US$47,950)] for the matched controls, with a difference of US$44,070 [95% CI (US$27,132–US$61,008); p < 0.001]. The mean cost in year 2 was US$48,114 [95% CI (US$31,722–US$64,507)] for patients with NTM-PD and US$28,990 [95% CI (US$9429–US$48,552)] for the matched control group, with a difference of US$19,124 [95% CI (US$7865–US$30,383); p < 0.001].
Our findings, similar to those in other countries,14,15,24 showed that people with NTM infection had significantly higher rates of healthcare use and medical costs than those without. This increase in average medical costs per year was likely influenced by the increase in medical costs due to RD. For those without NTM infection, RD accounted for approximately 18% of the average medical costs per year, whereas for those with NTM infection, RD accounted for 52% of the average medical costs per year. In addition, inpatient costs per year accounted for approximately 60% of the average medical costs per year for people diagnosed with NTM infection, and 73% of these inpatient costs were due to RD.
A time-trend analysis of medical costs showed that medical cost was the highest 6 months before the index date in people with NTM infection. No previous data were found to analyze the cost before and after NTM infection, but considering that most of the medical costs for patients with active tuberculosis,25,26 another bacterial disease, are incurred during diagnosis and initial treatment, high medical costs for 6 months before and after diagnosis of NTM infection in our study may be due to the cost of diagnostic tests and initial treatment. In a previous study, total costs, including direct medical costs (e.g. physician services, diagnostic tests, and hospitalization expenses), direct non-medical costs (e.g. transport and food during healthcare visits), and indirect costs (e.g. wage and income lost) before and after tuberculosis diagnosis, were calculated through a systematic literature review. 26 Of the total costs for tuberculosis patients, direct medical costs were 17.2% before diagnosis and 7.8% after diagnosis.
Medical costs due to RD in people diagnosed with NTM infection were already high before they were diagnosed with NTM infection, and even after diagnosis, they were relatively higher than in those who were not diagnosed with NTM infection. Given that chronic lung diseases (e.g. COPD, bronchiectasis, and asthma) are known risk factors for NTM infection, cause respiratory symptoms, and require medical treatment even before NTM diagnosis, medical costs due to RD were relatively higher in people with NTM infection than in those without.
A previous study in Korea investigated the medical costs and healthcare utilization among people with NTM infection according to accompanying GERD. 27 In that study, among people with NTM infection, those with GERD had higher rates of medical use than those with only NTM, and medical costs for the former group were approximately twice as high. Considering the frequent chronic comorbidities in people with NTM infection,21,28 comorbid conditions other than RDs may be an additional cost burden for people with NTM infection.
Our study has several strengths. First, this study used the NHIS-NSC 2.0 database of South Korea, which is representative of the national population and contains healthcare utilization information from all settings in the country. Second, our study is one of the few to examine trends in healthcare use and costs among people with NTM using national-level data. Since there are limited data on medical use or costs related to NTM infection, we believe that our findings will be helpful to healthcare providers, health policymakers, and related researchers in the future.
Our study also has limitations to be discussed. First, the diagnosis of NTM infection and comorbidities in this study was based on insurance claims, which rely on the ICD-10 codes. The use of administrative claims data may have resulted in issues, such as coding accuracy (e.g. overcoding, undercoding, or miscoding), diagnostic inertia, and lack of disease specificity. Thus, we defined disease based on at least two claims associated with NTM infection (ICD-10, A31), similar to most previous studies analyzing claims data.8,17,24,29,30 Second, the study population was homogeneously Korean, which may limit the generalizability of the findings to other ethnic populations. Third, inflation and changes in the won–dollar exchange rate between 2003 and 2015 were not considered in this study. However, as cost studies related to NTM infection are very scarce, our study still provides the initial data necessary for conducting cost studies related to NTM infection in the future. Fourth, medical costs may differ depending on the characteristics of patients with NTM infections, the region in which they live, and the type of medical institution they visit, which was not considered in this study. A study design and stratification analysis that specifically considers NTM patients’ residential areas, the level of medical institution used, and patient characteristics are needed in future studies. Fifth, we could not assess potential indirect healthcare costs for reasons, such as loss of productivity. Therefore, the total healthcare expenditures may be higher than those currently reported. In addition, NTM infection has the potential to affect long-term health or result in the death of patients due to complications or comorbidities. A prospective cohort study of the effects of NTM infection on mortality and long-term disease burden is needed in the future.
In conclusion, patients diagnosed with NTM infection had significantly higher rates of healthcare use and medical costs than those without. In particular, the medical costs approximately 6 months before and after the diagnosis were high in people with NTM infection. In conclusion, NTM infection has been shown to increase the economic burden on people, and appropriate diagnostic tests and treatment plans for NTM infection and control are needed to reduce the disease burden on those diagnosed with NTM infection.
Supplemental Material
sj-docx-1-tar-10.1177_17534666221148660 – Supplemental material for Healthcare use and medical cost before and after diagnosis of nontuberculous mycobacterial infection in Korea: the National Health Insurance Service-National Sample Cohort Study
Supplemental material, sj-docx-1-tar-10.1177_17534666221148660 for Healthcare use and medical cost before and after diagnosis of nontuberculous mycobacterial infection in Korea: the National Health Insurance Service-National Sample Cohort Study by Seung Won Lee, Shihwan Chang, Youngmok Park, Sol Kim, Hojoon Sohn and Young Ae Kang in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.