
Abstract
Background:
To achieve favorable hemodynamics, the number of balloon pulmonary angioplasty (BPA) sessions varied significantly among patients with inoperable chronic thromboembolic pulmonary hypertension (CTEPH). Increased BPA sessions burdened patients financially and psychologically. We aim to identify baseline characteristics that could predict early BPA response.
Methods:
Consecutive patients who were diagnosed with inoperable CTEPH and received BPA between May 2018 and October 2021 at Fuwai Hospital were retrospectively collected. Patients were categorized into ‘Early BPA responders’ or ‘Non-early BPA responders’ according to the hemodynamic outcome within the first three BPA sessions.
Results:
In total, 101 patients were included into analysis. At baseline, non-early BPA responders had lower female proportion, longer disease duration, and poorer laboratory test results compared with early responders, whereas hemodynamics were comparable. After the first three BPA sessions, hemodynamic improvement was more significant in early responders. Incidence of complication was comparable between the two groups. Multivariable logistic analysis identified that female sex (odds ratio [OR]: 7.155, 95% confidence interval [CI]: 1.323-38.692, p = 0.022), disease duration (OR: 0.851, 95% CI: 0.727-0.995, p = 0.043), baseline total bilirubin (OR: 0.934, 95% CI: 0.875-0.996, p = 0.038), and baseline NT-proBNP (OR: 0.473, 95% CI: 0.255-0.879, p = 0.018) were independently associated with early BPA response. Combination of these four parameters could predict 90% early BPA response.
Conclusions:
Patients with shorter disease duration, female sex, lower baseline NT-proBNP, and lower baseline total bilirubin are more likely to achieve early hemodynamic response to BPA. Moreover, early hemodynamic response was not accompanied with increased incidence of procedure-related complications.
Keywords
Introduction
Chronic thromboembolic pulmonary hypertension (CTEPH) is a progressive disease featured by organized thrombi obstruction in major pulmonary arteries, along with peripheral microvasculopathy in nonoccluded areas, which could lead to right heart decompensation and death. 1 Pulmonary endarterectomy (PEA) is regarded as the standard treatment of CTEPH, whereas about 40% of patients are not eligible for PEA due to distal lesions or comorbidities. 2 Balloon pulmonary angioplasty (BPA) is a promising treatment for patients with inoperable CTEPH or suffering from persistent PH after PEA, which could significantly improve hemodynamics, exercise capacity and survival. 3
BPA is a staged interventional procedure with each session addressing different lesions. On average, patients with inoperable CTEPH are expected to receive 3–4 sessions of BPA to achieve favorable hemodynamics. However, some patients still suffer from poor hemodynamics even after multiple BPA sessions. 4 Hug et al. 5 have reported that hemodynamic improvement is blunted after the third BPA session. More BPA sessions also burdened patients financially and psychologically. 6 It is of clinical and economic significance to identify baseline characteristics that may predict early BPA response. However, this is barely investigated.
The current study aims to identify potential predictors of early BPA response, especially noninvasive parameters derived from baseline demographics and regular laboratory tests.
Study design and methods
Study design and participants
Consecutive patients diagnosed with inoperable CTEPH according to guidelines, 7 and underwent BPA between May 2018 and October 2021 in Fuwai Hospital, Chinese Academy of Medical Sciences (Beijing, China) were included in the study. The Ethics Committee of Fuwai Hospital gave approval to the current study protocol (Approval NO: 2020-1275), and the current study was in compliance with the ISHLT Ethics statement. Informed consents were obtained from each patient. The diagnosis of CTEPH was based on the 2015 ESC/ERS guidelines, 7 and the eligibility for BPA was based on a multidisciplinary discussion involving pulmonary vascular specialist, PEA surgeons and interventional specialist. Inclusion criteria were as follows: (a) patients diagnosed with inoperable CTEPH and receiving BPA and (b) patients with follow-up hemodynamics. Patients with BPA sessions less than 3 times and did not reach early hemodynamic response were excluded, because these patients had an uncertain hemodynamic response and were likely to achieve a favorable hemodynamic response at the completion of the third BPA treatment. Demographics, exercise capacity, laboratory tests and echocardiography were evaluated prior to and post every BPA session. Hemodynamics of patients were measured by right heart catheterization (RHC) again approximately 3 months after the last BPA treatment.
RHC and BPA procedural details
RHC and BPA procedural details were in accordance with our previous description and detailed in supplementary material. 3 Before each BPA session, RHC was performed to obtain the hemodynamics parameters. Subsequently, BPA was performed with selective pulmonary angiography and lung ventilation/perfusion scintigraphy as reference. Hemodynamics were measured again after each BPA session.
Definition of early BPA responders and non-early BPA responders
In accordance with the study by Taniguchi et al., 8 patients were categorized into ‘Early BPA responders’ or ‘Non-early BPA responders’ according to the hemodynamic outcome within the first three BPA sessions. ‘Early BPA responders’ were patients who achieved a mean pulmonary arterial pressure (mPAP) ⩽ 30 mmHg and/or a reduction of pulmonary vascular resistance (PVR) ⩾ 30% within three BPA sessions. Otherwise, the patients were categorized as ‘Non-early BPA responders’.
Statistical analysis
Distribution of variables was examined by Kolmogorov-Smirnova test. Accordingly, normally distributed continuous parameters were examined by independent-sample t test and presented as the mean ± standard deviation; abnormally distributed continuous parameters were examined by Mann–Whitney U test and presented as the median (interquartile range). Categorical variables are given as counts (percentages) and the Chi-square test with or without continuity correction or Fisher exact test was used to compare differences between groups. Two-way repeated measures of variance were applied to evaluate hemodynamic changes after each BPA session with Bonferroni post hoc tests for multiple comparisons. Univariable and multivariable logistic regressions (backward elimination method) were used to identify parameters independently correlated with early response to BPA. A receiver operator characteristic curve analysis was applied to evaluate predictive ability of variables. A two-tailed p value less than 0.05 was considered of statistical significance. SPSS 26.0 (IBM SPSS Corp.; Armonk, NY, USA) and Prism GraphPad 9 (GraphPad Software, LA Jolla, CA, USA) were used for statistical analyses.
Results
Baseline demographics of included patients
A total of 184 patients with inoperable CTEPH underwent BPA from May 2018 to October 2021 (Figure 1). Among them, 83 patients were excluded due to lack of follow-up hemodynamics (n = 54) or BPA sessions < 3 with uncertain hemodynamic response (n = 29). Finally, a total of 101 patients were included into analysis with 279 BPA sessions performed. The mean age of included patients was 58.94 ± 11.36 years old and 57 (56.44%) were females. The median time interval between baseline and follow-up hemodynamic measurement was 9 months (interquartile range: 5–14 months). Within 3 BPA sessions, 89 patients achieved favorable hemodynamic response to BPA, whereas 12 patients did not.

The patient enrollment flow chart.
Early BPA responders vs non-early BPA responders
At baseline, non-early BPA responders had lower female proportion, longer disease duration, and poorer laboratory test results compared with early responders, whereas hemodynamics and exercise capacity were comparable between the two groups (Table 1). The prevalence of comorbidities was also comparable between the two groups except higher prevalence of atrial fibrillation in non-early BPA responders, which might account for larger left atrial anteroposterior diameter in non-early BPA responders. Baseline serum levels of N-terminal pro-brain natriuretic peptide (NT-proBNP), total bilirubin, direct bilirubin and creatinine were significantly higher in non-early responders. Of note, hemodynamics such as mPAP and PVR were comparable between the two groups at baseline. The number and type of baseline lesions were also comparable between the two groups except higher proportion of total occlusion in non-early responders (6.91% vs 15.66%, p = 0.050).
Clinical features of early BPA responders and non-early responders at baseline.

Alb, albumin; ALT, glutamic pyruvic transaminase; AST, aspartate amino transferase; BPA, balloon pulmonary angioplasty; BMI, body mass index; CREA, creatinine; DBil, direct bilirubin; dPAP, diastolic pulmonary arterial pressure; EF, ejection fraction; GGT, gamma glutamyl transpeptidase; LA, left atrium dimension; mPAP, mean pulmonary arterial pressure; mRAP, mean right atrial pressure; NT-proBNP, N-terminal pro-brain natriuretic peptide; PAWP, pulmonary arterial wedge pressure; PVR, pulmonary vascular resistance; RVED/LVED, right ventricular end-diastolic diameter/ left ventricular end-diastolic diameter; 6MWD, 6-min walk distance; sPAP, systolic pulmonary arterial pressure; SVO2, mixed venous oxygen saturation; TRV, tricuspid regurgitation velocity; TBil, total bilirubin; TP, total protein; WHO FC, World Health Organization functional class. Significant p values (p < 0.05) are bolded.
per patient.
sum of all lesions in each group
Data are presented as mean ± standard deviation, median (interquartile range) or number (percentage).
Within the first three BPA sessions, both early and non-early responders had comparable number of total dilated pulmonary segments, similar number of dilated lower pulmonary vessels and comparable time interval between baseline and follow-up despite more BPA sessions in non-early responders (Table 2). Despite comparable dilated pulmonary segments, clinical profiles varied significantly after the first 3 BPA sessions. Compared with non-early responders, early BPA responders had significantly lower NT-proBNP levels, more favorable hemodynamics, better cardiac function (Table 2). Distinctively, a significantly steeper reduction in mPAP and PVR was observed in early responders (Figure 2). When analyzing hemodynamics at the procedural level, early responders had significant reduction in mPAP and PVR after each BPA session, whereas in non-early responders, bare hemodynamic improvement was observed when comparing hemodynamics procedurally with preceding BPA sessions. However, when cumulatively observed, hemodynamics of non-early responders were also significantly improved after the third BPA session compared with baseline.
Clinical features of early BPA responders and non-early responders at follow-up.

Alb, albumin; ALT, glutamic pyruvic transaminase; AST, aspartate amino transferase; BPA, balloon pulmonary angioplasty; CREA, creatinine; DBil, direct bilirubin; dPAP, diastolic pulmonary arterial pressure; EF, ejection fraction; GGT, gamma glutamyl transpeptidase; LA, left atrium dimension; mPAP, mean pulmonary arterial pressure; mRAP, mean right atrial pressure; NT-proBNP, N-terminal pro-brain natriuretic peptide; PAWP, pulmonary arterial wedge pressure; PVR, pulmonary vascular resistance; RVED/ LVED, right ventricular end-diastolic diameter/ left ventricular end-diastolic diameter; 6MWD, 6-min walk distance; sPAP, systolic pulmonary arterial pressure; SVO2, mixed venous oxygen saturation; TRV, tricuspid regurgitation velocity; TBil, total bilirubin; TP, total protein; WHO FC, World Health Organization functional class. Significant p values (p < 0.05) are bolded.
Data are presented as mean ± standard deviation, median (interquartile range) or number (percentage).
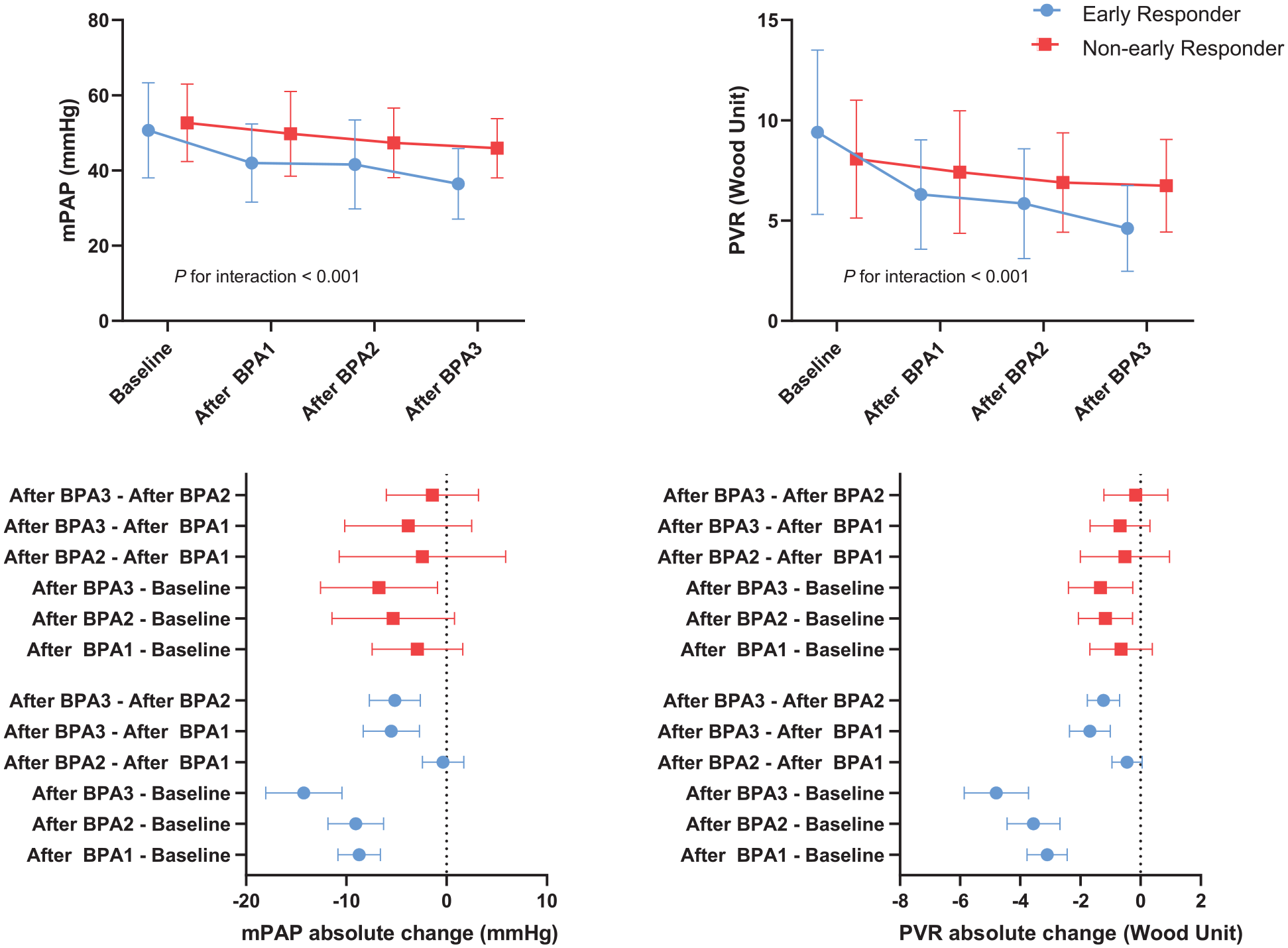
The time course of mPAP and PVR during BPA sessions, stratified by early BPA responders and non-early BPA responders.
Complications in early BPA responders and non-early BPA responders
Complications of BPA were analyzed at the procedural level (Table 3). BPA-related complications occurred in 36 procedures (12.90% of all 279 procedures), which was mostly attributed to hemoptysis or hemosputum (7.89% of all 279 procedures) and mild vascular injury (2.87% of all 279 procedures). The occurrence of complications was comparable in both groups.
Procedure level analysis of complications in early BPA responders and non-early responders.

BPA, balloon pulmonary angioplasty.
Data are presented as number (percentage).
Predictors of early response to BPA
Univariable logistic regression analysis identified that age, female sex, disease duration, baseline NT-proBNP, number of total occlusion lesions, gamma glutamyl transpeptidase, total bilirubin, direct bilirubin and creatinine were correlated with BPA early response (Table 4), whereas baseline hemodynamics, the number of baseline lesions, the number of dilated lower lung field, BPA eligibility, the number of total dilated pulmonary segments could not predict early response. After adjusting for confounders, female sex (odds ratio [OR]: 7.155, 95% confidence interval [CI]: 1.323-38.692, p = 0.022), disease duration (OR: 0.851, 95% CI: 0.727-0.995, p = 0.043), baseline total bilirubin (OR: 0.934, 95% CI: 0.875-0.996, p = 0.038) and baseline NT-proBNP (OR: 0.473, 95% CI: 0.255-0.879, p = 0.018) could predict early response to BPA independently (Table 5), whereas the number of total occlusion lesions lost statistical significance (Table S2). Moreover, using these four parameters could predict 89.9% early BPA response (AUC: 0.899, 95% CI: 0.829-0.969; Formula: Early response = 2.691-0.069*Tbil-0.748*NT-proBNP + 1.968*Female-0.162*Disease duration) (Figure 3).
Univariable logistic regression analysis for early response to BPA.

Alb, albumin; ALT, glutamic pyruvic transaminase; AST, aspartate amino transferase; BPA, balloon pulmonary angioplasty; BMI, body mass index; CREA, creatinine; DBil, direct bilirubin; dPAP, diastolic pulmonary arterial pressure; EF, ejection fraction; GGT, gamma glutamyl transpeptidase; mPAP, mean pulmonary arterial pressure; NT-proBNP, N-terminal pro-brain natriuretic peptide; PVR, pulmonary vascular resistance; RVED/ LVED, right ventricular end-diastolic diameter/ left ventricular end-diastolic diameter; 6MWD, 6-min walk distance; SVO2, mixed venous oxygen saturation; TRV, tricuspid regurgitation velocity; TBil, total bilirubin; TP, total protein; WHO FC, World Health Organization functional class. Significant p values (p < 0.05) are bolded. Lower lung field refers to A6-A10.
Baseline variable were included in analysis.
for each increase of 1000 ng/L in NT-proBNP.
per patient.
Multivariable logistic regression analysis for early response to BPA.
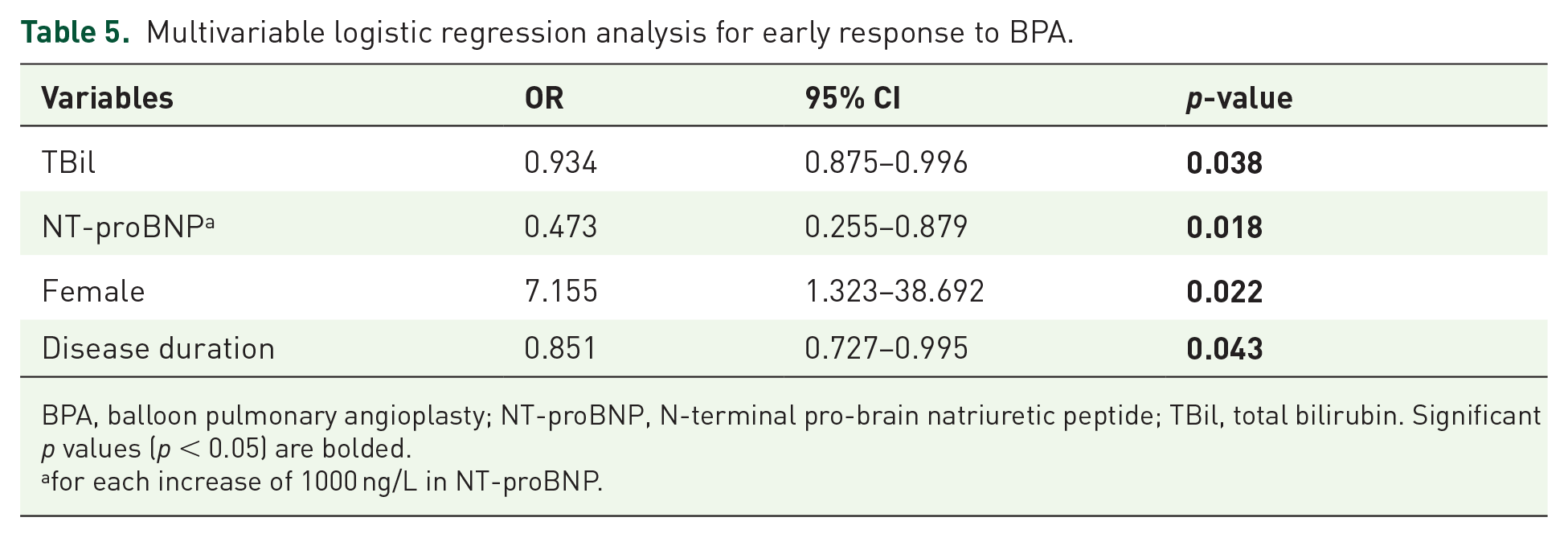
BPA, balloon pulmonary angioplasty; NT-proBNP, N-terminal pro-brain natriuretic peptide; TBil, total bilirubin. Significant p values (p < 0.05) are bolded.
for each increase of 1000 ng/L in NT-proBNP.

Receiver operator characteristic curve of parameters in predicting early hemodynamic response to BPA.
Discussion
In the present study, we found that shorter disease duration, female gender, lower baseline NT-proBNP, and baseline total bilirubin could independently predict early hemodynamic response to BPA, whereas baseline hemodynamics and the number of dilated lower lung field did not. Moreover, the combination of these four parameters had 90% probability to correctly predict whether a patient could achieve a favorable hemodynamic response within three BPA sessions.
Significance of early response
Generally, BPA is performed multiple times with each session addressing different lesions to reduce the risk of complication. To achieve prognostic beneficial hemodynamics, number of BPA sessions varied significantly among different patients, ranging from 3 to 10. 9 One more BPA session indicates at least 4 months delay in achieving favorable hemodynamics, 5 which could be further prolonged for patients who live far from experienced PH center under the COVID-19 pandemic. Delayed return to prognostic beneficial hemodynamics could contribute to poorer survival. 10 Besides impaired prognosis, each additional BPA session was estimated to increase annual hospital costs by 10,000 Euro and medication costs by 20,000 Euro. 6 Moreover, patients with blunted hemodynamic improvement after BPA are more likely to receive PH targeted medication, which might further exaggerate the financial cost to 25,000 Euro per quality-adjusted life year. 6 Due to limitation in daily activity and high financial cost, patients with CTEPH also suffered from profound emotional burdens and poor quality of life. 11 Increased BPA sessions and prolonged medical treatment could further increase patients’ anxiety. Therefore, earlier achievement of favorable hemodynamics is of prognostic and socioeconomic significance.
Hug et al. 5 have demonstrated that hemodynamic improvement blunted after the third BPA session, which was also observed in non-early responders in the current study. While early responders achieved significant hemodynamic improvement after each BPA session, hemodynamic improvement was not obvious in non-early responders when analyzed procedurally and only became evident when analyzed cumulatively.
Predictors of early response
Compared with early BPA responders, non-early responders had significantly longer disease duration, which could contribute to more advanced pulmonary vascular remodeling and microvasculopathy. 12 Consistent with current study, previous studies have found that BPA could not address microvasculopathy. Patients with impaired subpleural perfusion, 8 reduced diffusing capacity for carbon monoxide8,13 and longer duration between disease onset and BPA 12 , which reflects advanced microvasculopathy, had poor hemodynamic responses even after sufficient BPA sessions (5 BPA sessions on average).
Females are more likely to achieve early BPA response compared with male counterparts. Similarly, previous studies have found that female patients with CTEPH had better survival than males, irrespective of receiving PEA or not, despite higher prevalence of PH in female. 14 The underlying mechanism could be attributable to protective effect of estrogen and detrimental impact of testosterone on cardiac and pulmonary vessels. 15 Studies found that testosterone correlated with right ventricular hypertrophy and fibrosis, contributing to impaired right ventricular-pulmonary artery coupling and more advanced pulmonary artery remodeling. 15
When mPAP mildly elevated, right ventricular could enhance contractility to maintain cardiac output. With disease progression, mPAP further increases and right ventricular decouples from pulmonary artery, leading to right heart failure and hepatic congestion, which could be reflected by elevated NT-proBNP and total bilirubin, respectively. 16 NT-proBNP mirrors cardiac wall stress and ventricular remodeling, which is associated with cardiac impairment and prognosis of patients with PH. 7 As the most widely used biomarker of PH, NT-proBNP is incorporated into risk stratification of patients with PH in 2015 ESC/ERS guidelines. 7 Surie et al. 17 found that patients with lower BNP level at baseline had reduced risk of residual PH after PEA and better postoperative survival. The role of NT-proBNP in BPA had been investigated by Kriechbaum et al., 18 who found that the reduction of NT-proBNP is proportional to hemodynamic improvement after BPA, indicating that consecutively monitoring NT-proBNP level under staged BPA treatment could facilitate evaluating BPA efficacy and assessing disease severity. Furthermore, our current study suggested that higher NT-proBNP at baseline was associated with blunted hemodynamic response after BPA and each 1000 ng/L increase in NT-proBNP doubled the risk of delayed hemodynamic response to BPA, which could facilitate clinicians’ planning of BPA sessions and conservation with BPA candidates. Besides elevation of NT-proBNP, advanced right heart failure also impairs inferior venal cava backflow, leading to hepatic congestion and elevation of total bilirubin level. Total bilirubin also serves as an indicator of right heart failure and could predict BPA early response.
Contrary to our initial hypothesis that treating lower lung field contributes to early BPA response, we found that the location of treated lung field could not predict BPA early response. Similarly, Hug et al. 5 found that treating basal lung field did not contribute to greater hemodynamic improvement than addressing apical lesions. Tsuji et al. 12 reported that location of addressed pulmonary vessels was not associated with hemodynamic outcome after BPA. Supine position when measuring hemodynamics might account for the comparable hemodynamics when treating different lung fields given that bases have more pulmonary perfusion only in a standing position rather than a supine position. Although the number of total occlusion lesions was associated with early response in univariable logistic regression, statistical significance was lost after adjusting for disease duration and NT-proBNP, which could be attributed to the causal relationship between total occlusion and disease duration. Long-term disease duration could contribute to vessel occlusion.
In the current study, the total complication rate was 12.9%, mainly attributed to hemoptysis and mild pulmonary vascular injury, which was comparable to the results of a current meta-analysis, namely 11.8% of all included BPA sessions. 9 We previously assumed that early BPA responders might have higher incidence of BPA associated complications than non-early responders. However, the incidence of complications was comparable between early responders and non-early responders, indicating that achieving favorable hemodynamics earlier did not contribute to more complications.
Impact of medication on BPA
In the current study, 62.38% patients received PAH specific medical therapy at baseline, and non-early responders were more likely to receive PAH targeted medicine compared with early responders, whereas the difference did not reach statistical significance. The higher proportion of PAH targeted medication in non-early responders might be attributable to poorer clinical status at baseline compared with early responders. Therefore, these patients were more likely to receive PAH targeted medication prior to BPA to achieve a more stable and optimal state. To preclude the potential bias introduced by PAH-targeted drug administration at baseline, we further adjusted for baseline PAH targeted medication in multivariable logistic regression, and found that baseline PAH targeted medication was not associated with early response after BPA. Similar results were also observed in the previous studies, where baseline PAH targeted therapy was comparable between ‘BPA responders’ and ‘BPA non-responders’ 8 or ‘patients with residual PH’ and ‘without residual PH after BPA’. 12 Currently, riociguat is the only PAH targeted medication approved for CTEPH by US Food and Drug Administration, which could only reduce mPAP by 4.5 mmHg based on the phase II study of riociguat for patients with CTEPH. 19 Other PAH targeted agents, including endothelin receptor antagonists, phosphodiesterase-5 inhibitors and prostacyclin analogues, despite being widely off-label prescribed, were not approved for the treatment of CTEPH, and could only reduce mPAP or PVR to a small extent.20–22 Of note, an international prospective registry study found that the survival rates were comparable between those who received and did not receive PAH-targeted therapy. 23 Therefore, the impact of PAH-targeted medication on hemodynamics of CTEPH might be limited.
Limitation
The current study had inherent limitations of retrospective design. In all, 83 patients were excluded due to lack of follow-up hemodynamics or insufficient BPA sessions. In addition, the study was based on a single center. However, Fuwai hospital is one of the largest and the most experienced expert CTEPH centers in China, where patients come from all over the country. Therefore, the patients in the current study are representative. The sample size of current study is relatively small, which warrants future studies with larger sample size. In the current study, 63 (62.38%) patients received PAH specific medical therapy at baseline and non-early responders were more likely to receive PAH targeted medicine compared with early responders (83.3% vs 59.6%, p = 0.110). To preclude the potential bias introduced by PAH targeted medication at baseline, we further adjusted for baseline PAH targeted drugs in multivariable logistic regression, and found that total bilirubin, NT-proBNP, female sex and disease duration were still independently associated with non-early response after BPA in multivariable logistic regression (Supplemental Table S3).
Conclusion
Patients with shorter disease duration, female sex, lower baseline NT-proBNP and baseline total bilirubin are more likely to achieve early hemodynamic response to BPA. Moreover, early hemodynamic response was not accompanied with increased incidence of procedure-related complications.
Supplemental Material
sj-docx-1-tar-10.1177_17534666221138001 – Supplemental material for Predictors of early response to balloon pulmonary angioplasty in patients with inoperable chronic thromboembolic pulmonary hypertension
Supplemental material, sj-docx-1-tar-10.1177_17534666221138001 for Predictors of early response to balloon pulmonary angioplasty in patients with inoperable chronic thromboembolic pulmonary hypertension by Xin Li, Yi Zhang, Qi Jin, Qin Luo, Qing Zhao, Tao Yang, Qixian Zeng, Lu Yan, Anqi Duan, Zhihua Huang, Meixi Hu, Changming Xiong, Zhihui Zhao and Zhihong Liu in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.