
Abstract
Background:
Significant achievements in the treatment of chronic thromboembolic pulmonary hypertension (CTEPH) have provided effective therapeutic options for most patients. However, the true impact of the changed landscape of CTEPH therapies on patients’ management and outcomes is poorly known. We aimed to characterize the incidence, clinical characteristics, and outcomes of CTEPH patients in the modern era of CTEPH therapies.
Methods:
We analyzed the data of CTEPH adults enrolled in the prospective multicenter registry.
Results:
We enrolled 516 patients aged 63.8 ± 15.4 years. The incidence rate of CTEPH was 3.96 per million adults per year. The group was burdened with several comorbidities. New oral anticoagulants (n = 301; 58.3%) were preferred over vitamin K antagonists (n = 159; 30.8%). Pulmonary endarterectomy (PEA) was performed in 120 (23.3%) patients and balloon pulmonary angioplasty (BPA) in 258 (50%) patients. PEA was pretreated with targeted pharmacotherapy in 19 (15.8%) patients, and BPA in 124 (48.1%) patients. Persistent CTEPH was present in 46% of PEA patients and in 65% of patients after completion of BPA. Persistent CTEPH after PEA was treated with targeted pharmacotherapy in 72% and with BPA in 27.7% of patients. At a mean time period of 14.3 ± 5.8 months, 26 patients had died. The use of PEA or BPA was associated with better survival than the use of solely medical treatment.
Conclusions:
The modern population of CTEPH patients comprises mostly elderly people significantly burdened with comorbid conditions. This calls for treatment decisions that are tailored individually for every patient. The combination of two or three methods is currently a frequent approach in the treatment of CTEPH.
Clinical Trial Registration:
clinicaltrials.gov/ct2/show/NCT03959748
Introduction
Chronic thromboembolic pulmonary hypertension (CTEPH) is a rare and progressive disease caused by obstruction of the pulmonary arteries (PAs) by organized thrombi with accompanying precapillary arteriopathy.1–4 Prognosis in this disease has significantly improved 5 with the advent of pulmonary endarterectomy (PEA), which has provided hemodynamic normalization and improved clinical outcomes,2,6 especially in patients with central localization of pulmonary obstruction.
The group of CTEPH patients was well characterized in a large prospective international registry which enrolled patients between February 2007 and January 2009. 7 As the phenotype of CTEPH patients may be population dependent, 8 several national reports as summarized in Table 17,9–29 were of added value. Most of them, however, recruited patients before the marketing authorization of riociguat by the European Medicines Agency through the European Union (27/03/2014), and before the first experience with balloon pulmonary angioplasty (BPA) outside of Japan. 30 Significant achievements in the treatment of CTEPH in the last decade have provided effective therapeutic options for most CTEPH patients, even those with distal localization of the thrombi. This was mainly due to refinement of the technique of BPA by Japanese physicians.31,32 However, the true impact of the changed landscape of CTEPH therapies on patients’ management and outcomes is poorly known and thus far the results of only one prospective CTEPH registry enrolling patients in the BPA era have been published. 25 Therefore, in the present study based on the multicenter national registry (Polish Registry of Pulmonary Hypertension; BNP-PL) we assessed the prevalence, incidence, clinical characteristics and outcomes of patients with CTEPH recruited in the modern era of CTEPH therapies.
Summary of national and international CTEPH registries.

Mean ± standard deviation.
Increased during observation period.
Operated (PEA and/or BPA) versus non-operated.
Data available for only 310 patients.
Median and interquartile range.
Excluded patients ⩾85 years.
Also centers from Germany, Czech Republic and Slovakia.
BPA, balloon pulmonary angioplasty; CTEPH, chronic thromboembolic pulmonary hypertension; P, prospective analysis; PEA, pulmonary endarterectomy; PH, pulmonary hypertension; R, retrospective analysis.
Methods
Registry design and CTEPH diagnosis
The design of the BNP-PL registry (https://clinicaltrials.gov/ct2/show/NCT03959748), enrollment criteria, and data collection were recently described in detail.33–35 The CTEPH adult arm of the registry enrolls adults with CTEPH from all 16 CTEPH reference centers in Poland accredited by the National Health Fund (NHF) for medical treatment of CTEPH. This ensures that all diagnosed patients in Poland are included in the registry. Among the enrolled centers, eight are actively involved in the BPA programme. Patients qualifying for PEA are referred to one of two cardiac surgery centers experienced in PEA. The protocol of the study was reviewed and accepted by the Bioethical Committee of Physicians and Dentists Chamber in Krakow (L.dz.OIL/KBL/27/2018). All patients signed an informed consent before enrollment in the study.
For the purposes of the present study, we analyzed the data of newly and previously diagnosed CTEPH adult (>18 years old) patients who were managed in the participating centers between 1 March 2018 and 31 August 2019. The diagnostic algorithm of CTEPH was based on current European Society of Cardiology (ESC) and European Respiratory Society (ERS) recommendations. 2 Newly diagnosed patients were those whose diagnoses had been established since 1 March 2018 (termed ‘incident cases’). At the time of enrollment they had not been treated for CTEPH. Patients who were diagnosed earlier have been classified as ‘prevalent cases’. All patients were categorized as operable or non-operable by one of two CTEPH teams. 36 The diagnosis of CTEPH was at the discretion of co-investigators who managed the enrolled patients in their centers. However, the diagnosis had to fulfill the criteria recommended by the ESC and ERS. The validity and credibility of the diagnostic algorithms were ensured by the experience of the investigators, CTEPH team evaluation, and an audit of the NHF programme.
Baseline and follow-up assessment
We analyzed patients’ characteristics at three timepoints: the time of diagnosis, enrollment, and follow-up. In incident cases the time of diagnosis was the same as the time of enrollment. The minimum set of data at diagnosis included: World Health Organization functional class (WHO-FC), CTEPH team opinion (operable versus non-operable), results of the imaging tests to diagnose CTEPH and data obtained at right heart catheterization such as mean pulmonary artery pressure (mPAP), right atrial pressure, cardiac index, pulmonary vascular resistance, PA wedge pressure, and PA oxygen saturation. 37 At enrollment we gathered the following data: WHO-FC, 6-minute walk distance (6MWD), N-terminal pro-brain natriuretic peptide (NT-proBNP) or brain natriuretic peptide (BNP), and right atrial area (RAA) as assessed by echocardiography, medical, surgical, or interventional treatments, and comorbidities. All follow-up visits were scheduled according to the NHF programme criteria, which require the assessment of treatment efficacy at 3 to 6-month intervals. Patients were followed from the time of enrollment until 31 August 2019.
Statistical analysis
The period prevalence of CTEPH was calculated as the number of patients diagnosed with CTEPH in every center who were alive on 1 March 2018, and all new patients diagnosed between 1 March 2018 and 31 August 2019 (numerator) per the total number of Polish adults (denominator, n = 31,512,906; 16,471,228 adult women and 15,041,678 adult men) based on the most recent data (31 December 2017) obtained from Statistics Poland (Central Statistical Office, https://stat.gov.pl/en). The incidence was calculated as the number of new CTEPH cases per year (numerator) per the number of Polish adults (denominator). For the comparison of continuous variables between the two groups, we used the Student’s t test, and for categorical variables the chi 2 test with Yates’s correction as needed. A Kaplan–Meier survival curve was used to delineate patient survival starting at the time of enrollment. The significance level was set at an alpha level of 0.05. Statistical analysis was performed with the use of Dell Inc. (2016), Dell Statistica (data analysis software system), (version 13; Dell, Texas, USA) software.dell.com.
Results
Study group and diagnostics
We enrolled in the present study 516 patients with CTEPH aged 63.8 ± 15.4 years, including 329 (63.8%) prevalent and 187 (36.2%) incident cases. At enrollment a significant number of patients (n = 286; 55.4%) were ⩾65 years old. Most patients were at WHO-FC II and III (n = 235; 45.5% and n = 225; 43.6%, respectively) followed by patients at WHO-FC I and IV (n = 39; 7.6% and n = 17; 3.3%, respectively). The mean 6MWD was 334 ± 166.4 m, the mean NT-proBNP level was 1482 ± 3130 pg/ml, and the mean RAA was 28.1 ± 17 cm2. At enrollment the study patients were treated with riociguat (n = 247; 47.9%), sildenafil (n = 93; 18%), treprostinil (n = 12; 2.3%), macitentan (n = 3; 0.6%) and bosentan (n = 1; 0.2%).
At diagnosis (Table 2) most patients were at WHO-FC III; however, incident cases were less functionally impaired than prevalent cases. The period prevalence of CTEPH was 16.4 per million adults, including 15.5 per million women and 17.3 per million men. The incidence rate was estimated at 3.96 new CTEPH patients per million per year.
Characterization of the study group at the time of diagnosis of chronic thromboembolic pulmonary hypertension.
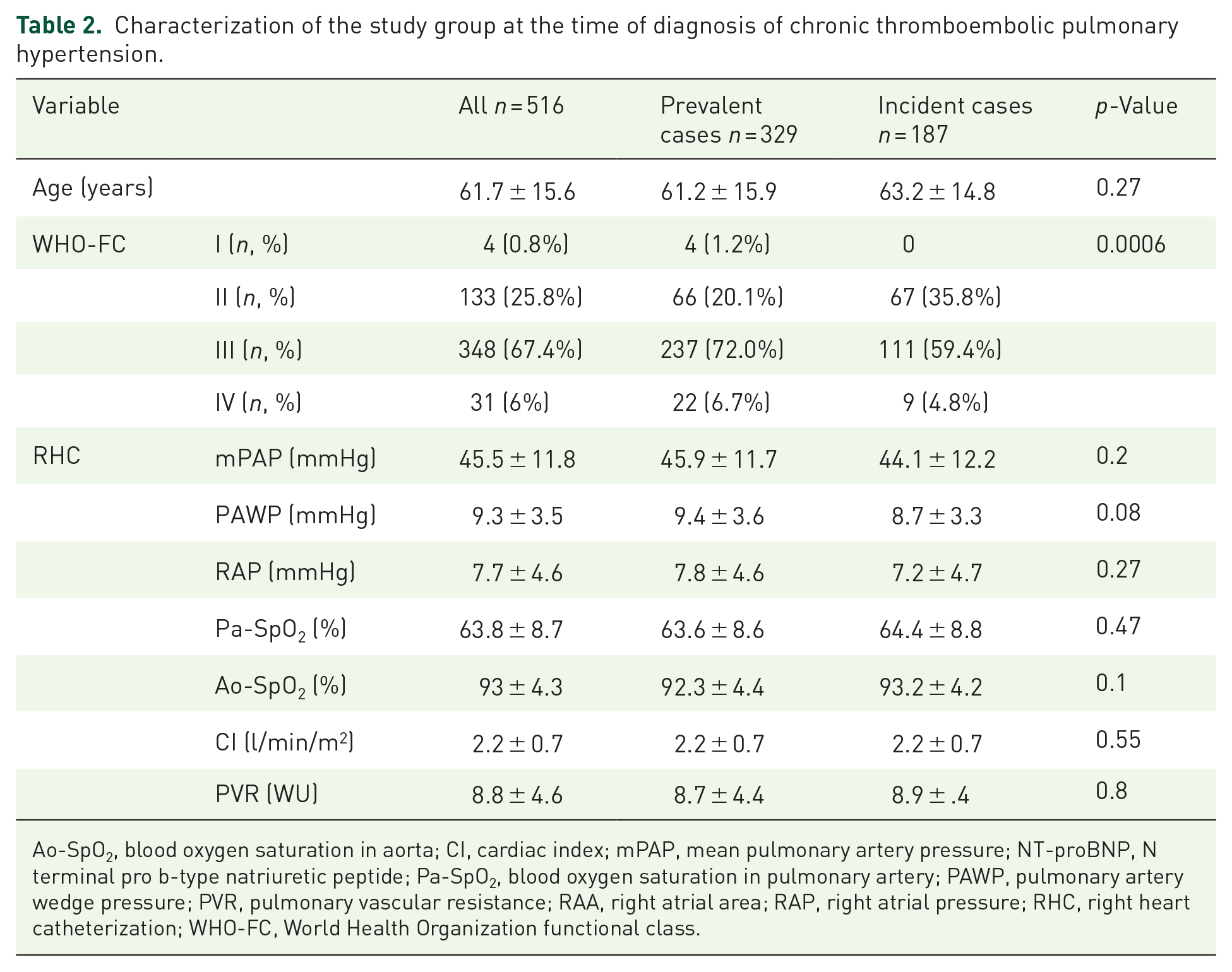
Ao-SpO2, blood oxygen saturation in aorta; CI, cardiac index; mPAP, mean pulmonary artery pressure; NT-proBNP, N terminal pro b-type natriuretic peptide; Pa-SpO2, blood oxygen saturation in pulmonary artery; PAWP, pulmonary artery wedge pressure; PVR, pulmonary vascular resistance; RAA, right atrial area; RAP, right atrial pressure; RHC, right heart catheterization; WHO-FC, World Health Organization functional class.
CTEPH was confirmed by classic PA arteriography in most patients (n = 496; 96.1%). In the other 20 (3.9%) patients the diagnosis was based on computed tomography pulmonary artery angiography (CTPA).
During the diagnostic work-up, ventilation–perfusion lung scintigraphy (V/Q scan) was performed in 155 (30%) patients and perfusion scintigraphy in 57 (11%) patients. In most patients (n = 133; 25.8%) the single photon edition computed tomography (SPECT-CT) technique was used. In the remaining 22 (4.3%) patients, planar lung scintigraphy was applied. V/Q scan showed at least one unmatched segmental perfusion defect in 118 (76.1%) patients and at least one unmatched subsegmental perfusion defect in an additional 37 (23.9%) out of the 155 patients who had been tested with this technique.
Using PA arteriography as the reference method to detect CTEPH, we found that the criterion of one or more mismatched segmental perfusion defect in V/Q scan had a sensitivity to diagnose CTEPH of 81.1% (95% confidence interval (CI): 72.5–87.9%), the criterion of any mismatched perfusion defects had a sensitivity of 100% (95% CI: 96.7–100%), and CTPA had a sensitivity of 76.6% (95% CI: 67.6−84.1%). Central lesions were present in 157 (30.4%) patients, peripheral lesions were present in 206 (39.9%) patients, and mixed (central and peripheral) lesions were present in 144 (27.9%) patients.
At the time of diagnosis 362 (70.2%) patients were classified as inoperable and 154 (29.8%) were considered operable. Inoperability resulted from distal localization of the thromboembolic lesions (n = 225; 62.2%), poor clinical status, low benefit-to-risk ratio or comorbidities (n = 88; 24.3%), or a lack of consent (n = 49; 13.5%).
Therapy
At enrollment to the study PEA or BPA were completed in 216 patients. In 100 patients BPA treatment was ongoing, and the remaining 200 patients had had no previous intervention. At follow-up PEA was performed in an additional 13 patients and BPA in an additional 19 patients. Overall, PEA was performed in 120 (23.3%) patients and BPA in 258 (50%) patients (Figure 1). Analysis of the treatment status at study enrollment showed that the near normalization of mPAP (<25 mmHg) was present in 44.3% of patients after PEA and 35.3% of patients after BPA (Table 3). Additional BPA after PEA resulted in hemodynamic near-normalization in 35% of patients (Table 3).
Treatment status of study patients at enrollment.

BPA, balloon pulmonary angioplasty; CTEPH, chronic thromboembolic pulmonary hypertension; mPAP, mean pulmonary artery pressure; PEA, pulmonary endarterectomy.

Assessment of operability by the chronic thromboembolic pulmonary hypertension (CTEPH) teams and final treatment of the study group.
Before PEA 19 (15.8%) patients were pretreated with targeted pharmacotherapy, while BPA was pretreated in 124 (48.1%) patients. Table 3 shows that almost half of the patients treated with BPA still continued targeted pharmacotherapy despite mPAP near-normalization, which is in contrast to the group of patients after PEA. Targeted pharmacotherapy included monotherapy in most patients (n = 343; 97.4%), and a combination therapy in a small group of nine (2.6%) patients who participated in the open-label phases of clinical trials. The therapies included: riociguat (n = 253; 71.9%), sildenafil (n = 83; 23.6%), subcutaneous treprostinil (n = 5; 1.4%), macitentan (n = 2; 0.6%) and combinations of sildenafil and treprostinil (n = 1; 0.3%), sildenafil and macitentan (n = 1; 0.3%), sildenafil and bosentan (n = 1; 0.3%), and riociguat and treprostinil (n = 6; 1.7%).
Associated medical conditions and additional therapies
Most patients had a history of acute pulmonary embolism (APE) and were of a blood group other than O (Table 4). They also frequently presented with conditions characteristic of left heart disease. The operable patients, as compared to the non-operable patients, were younger, more frequently of a blood group other than O and had a history of deep vein thrombosis and APE. In turn, non-operable patients more frequently had thyroid disorders including hypothyroidism and hyperthyroidism. Most patients were using anticoagulation at enrollment, usually in the form of non-vitamin K antagonist oral anticoagulants (NOACs) (Table 5). The other frequently used therapies reflected the burden of comorbidities.
Associated medical conditions and additional therapies in patients with chronic thromboembolic pulmonary hypertension at enrollment to the study.

COPD, chronic obstructive pulmonary disease; PE, pulmonary embolism.
Pharmacotherapy in the study patients at enrollment to the registry.

Follow-up
Patients were followed for a mean of 14.3 ± 5.8 months. During that time 26 (5%) patients died due to progression of right heart failure (10 cases; 38.5%), cancer (three cases; 11.5%), infections (three cases; 11.5%), sudden cardiac death (two cases; 7.7%), respiratory failure (two cases; 7.7%), bleeding (one case; 3.8%), renal failure (one case; 3.8%) and unknown causes (four cases; 15.4%). Patients treated only with pharmacotherapy had more severe disease at enrollment and worse survival than patients treated with PEA or BPA (Table 6 and Figure 2). We did not find any difference in survival (p = 0.88) between patients treated with PEA and patients treated with BPA. Table 6 presents characteristics of patients in relation to the mode of treatment. As compared to invasive methods (PEA or BPA), medical treatment was chosen more frequently in more compromised patients defined by higher WHO-FC and NT-proBNP levels and shorter 6MWD, while BPA was preferred over PEA in older patients and in those with less centrally located lesions. Table 7 shows that patients who died at follow-up had higher NT-proBNP blood levels, greater RAA, and shorter 6MWD at enrollment than those who survived.
Comparison of study patients in relation to treatment modalities.

Patients in whom only pharmacological therapy was used.
Patients in whom PEA was used as a first-line invasive treatment.
Patients in whom BPA was used as a first-line invasive treatment.
In post hoc analysis significant differences were found between: (a) PEA group and medical treatment group (p < 0.0001) and between PEA group and BPA group (p < 0.0001); (b) all groups (p < 0.0001); (c) PEA group and medical treatment group (p < 0.0001) and between PEA group and BPA group (p < 0.0001); (d) medical treatment group and PEA group (p = 0.002) and medical treatment group and BPA (p = 0.0001) group; (e) medical treatment group and PEA group (p = 0.001) and medical treatment group and BPA (p = 0.0005) group; (f) medical treatment group and PEA group (p = 0.048); (g) medical treatment and PEA group (p = 0.001), and medical treatment and BPA (p = 0.03) group.
6MWD, 6-minute walk distance; BPA, balloon pulmonary angioplasty; NT-proBNP, N terminal pro B-type natriuretic peptide; PEA, pulmonary endarterectomy; RAA, right atrial area; WHO-FC, World Health Organization functional class.
Comparison of patients with chronic thromboembolic pulmonary hypertension with respect to survival at the end of follow-up.

6MWD, 6-minute walk distance; Ao-SpO2, blood oxygen saturation in aorta; CI, cardiac index; mPAP, mean pulmonary artery pressure; NT-proBNP, N terminal pro B-type natriuretic peptide; Pa-SpO2, blood oxygen saturation in pulmonary artery; PAWP, pulmonary artery wedge pressure; PVR, pulmonary vascular resistance; RAA, right atrial area; RAP, right atrial pressure; RHC, right heart catheterization; WHO-FC, World Health Organization functional class.

Kaplan–Meier survival curves for patients with chronic thromboembolic pulmonary hypertension treated with pulmonary endarterectomy (PEA) or balloon pulmonary angioplasty (BPA) (invasive treatment) and with only pharmacotherapy including targeted treatment.
Discussion
In the present study we have shown the most recent data on characteristics, diagnostic work-up, therapeutic decisions and outcomes of CTEPH patients in the era of advanced surgical, interventional, and pharmacological therapies. This population at its mean age over 60 years was diagnosed as being in poor functional status and burdened with several comorbidities. Most patients were classified as inoperable based on the CTEPH team decisions. Despite the fact that PEA remains a treatment of choice in CTEPH targeted pharmacotherapies and BPA have been used more frequently than PEA. Importantly, a hybrid use of two or three of the available treatment methods is typical, and pharmacotherapy has frequently been retained even after successful interventional treatment. Unexpectedly, we noted a preference for NOACs over vitamin K antagonists in this group.
CTEPH is considered a rare disease, but its prevalence and incidence are poorly known. Most data come from follow-up studies in patients presenting with APE. 2 However, a significant number of patients with CTEPH do not have a history of APE, which suggests that the true incidence of CTEPH is likely to be underestimated. 7 More robust data may come from observational studies that include all patients with a CTEPH diagnosis made in a general population of a given territory. In this way, 10 involving all pulmonary hypertension centers in the UK the incidence of CTEPH was estimated at 1.75 cases per million per year in 2006. Reports from other countries show similar (Spain 0.9 cases per million per year, Portugal 1.1 cases per million per year, Sweden two cases per million per year) or higher (Latvia 5.1 cases per million per year, Germany 5.7 cases per million per year) incidence of CTEPH, which locates our results in the middle. In a recent study using data from epidemiologic studies, registries and national databases, it has been estimated that diagnosed CTEPH patients account for only 7–29% of all CTEPH patients, which means that most CTEPH patients are still undiagnosed in our country and others. 38
In our study most patients had their final diagnosis of CTEPH made based on classic pulmonary angiography, which is a diagnostic gold standard, and rarely were they based on CTPA and lung V/Q scan only. The use of V/Q scan was relatively low, which results from the low availability of this diagnostic tool in Poland. However, the use of PA angiography was higher than in some previous reports 7 and was dictated by preferences of CTEPH teams, especially PEA and BPA specialists. In a subgroup of patients we could have found that the criterion of any perfusion lung defect in V/Q scan identified all patients who had CTEPH, but neither a lack of any segmental perfusion defect in V/Q scan nor a lack of angio-computed tomography signs of CTEPH were able to exclude the disease reliably. This observation is in line with previous reports39,40 and supports the recommendations of the nuclear medicine societies and reports of the Sixth World Symposium on Pulmonary Hypertension 2 to use binary interpretation of the lung V/Q scan.
In our study most patients were determined as inoperable due to distal localization of the thromboembolic lesions, poor clinical status, comorbidities, or lack of consent. This was in contrast to other national and international CTEPH registries in which operable patients accounted for 60% to 70% of the assessed groups (Table 1). Those studies, however, recruited patients before the wide availability of approved medical therapies and BPA, which may have influenced the decisions of the CTEPH teams. This was recently illustrated by a group at the French National Reference Center, 41 where the proportion of patients with CTEPH who had been operated on decreased after the advent of BPA (in 2014), from 82% in 2012–2013 to 51% in 2015–2016. Importantly, the total number of surgically treated patients with CTEPH remained unchanged because referrals increased during this time. Another analysis of the UK CTEPH center shows that the number of patients determined primarily as technically operable is significantly higher than the number of patients who are operated on (60% of patients qualifying for PEA). 42 In a recent German registry of CTEPH which enrolled newly diagnosed patients in 2016, only 50% were treated with PEA. 25 The Spanish Registry of Pulmonary Arterial Hypertension (REHAP), which started in 2007, shows that the chance of being operated on for CTEPH depended on the expertise of the qualifying center. 18 In designated CTEPH expert centers 47.9% of patients were operated on, while in other centers it was only 4.6% of patients. In Poland, where determination of CTEPH patients is centralized (conducted by two CTEPH teams) and regulated by a reimbursement policy of the NHF, 70% of patients were determined as inoperable. An important proportion of the patients in this group had poor clinical status and comorbidities which in the opinion of the CTEPH teams excluded them from operation. In fact our CTEPH patients had more comorbidities than those reported in the international registry 7 (e.g. obesity 31.6% versus 17.6%; coronary artery disease 18.6% versus 11.8%; diabetes 17% versus 5.2%) despite being of a similar age at study enrollment. When differences in the proportions of operable and inoperable patients in different studies are analyzed, it should be noted that there is no current method for standardizing operability or surgical risk for CTEPH, which to a large extent is a subjective decision of surgeons based on their experience.
Most patients enrolled in the registry were treated with one targeted drug, usually riociguat, which was the only treatment accepted for reimbursement by the NHF and which was supported by data from clinical trials.43,44 An important and new finding of our study is that targeted pharmacotherapies in some patients were used despite a good result of BPA. This might have resulted from the fact that BPA has usually been supported by pharmacotherapy and that the clinical significance of its withdrawal or maintenance has not been documented. Almost all CTEPH patients were anticoagulated at enrollment, usually with NOACs. Although the safety and efficacy of NOACs in CTEPH patients is unknown and their use has not been supported by pulmonary hypertension guidelines, the number of patients using NOACs presenting to CTEPH centers is rising,45,46 which results from the potential for a lower side-effect profile, and the greater convenience of dosing of NOACs over vitamin K antagonists. A multicenter retrospective analysis of patients with CTEPH after PEA showed that post-PEA functional and hemodynamic outcomes and bleeding risk were unaffected by the type of anticoagulation, but recurrent venous thromboembolism rates were significantly higher in those receiving NOACs. 45 Still, prospective studies are needed to understand the clinical usefulness of NOACs in CTEPH.
The most frequent comorbidities of CTEPH patients were hypertension, coronary artery disease (CAD), diabetes, thyroid disorders, and atrial fibrillation. The prevalence of cardiovascular disease (CVD) risk factors and CAD is high in our group, exceeding that reported in the international CTEPH registry, which had recruited patients 10 years earlier. This may result from the fact that Polish adults are generally burdened with a higher incidence of CVD risk factors and a higher risk of CVD mortality than their counterparts in western European countries.47,48 Thyroid disorders, especially hypothyroidism and treatment with levothyroxine, have previously been linked to CTEPH,49,50 and our results complement the previous findings. Our new observation is that hyperthyroidism was over two times more prevalent in non-operable patients as compared to operable patients. This association has never been analyzed and requires further research, but data from preclinical studies link elevated T3 to vascular remodeling, which plays an important role in patients with distal disease. 51 Most of our CTEPH patients had at least one APE in their history, but fewer than half had experienced deep vein thrombosis, which is in line with previous European reports. 7 Similarly to these reports, a history of deep vein thrombosis and APE, especially recurrent pulmonary embolism, were associated with the operable phenotype of CTEPH. Implantation of a vena cava filter was generally low. Its insertion was more commonly applied in operable patients, as it was previously a routine perioperative procedure in some centers.
We found that 64.7% of patients after completed BPA treatment and 55.7% of patients after PEA still had CTEPH (persistent or recurrent). These PEA results were similar in a recent study of the Papworth Hospital where 51% of patients still had mPAP ⩾25 mmHg at the time of follow-up right heart catheterization 3–6 months after PEA. 52 Based on our results, we do not conclude about the superiority of BPA or PEA, as in our study these two groups were not adjusted for such comparisons, but we underscore the need for careful observation of CTEPH patients after BPA and PEA. In addition, the relatively high rates of persistent CTEPH may support the role of adjunctive medical therapy in patients treated with PEA or BPA. However, PEA or BPA are associated with better survival than pharmacotherapy alone.
At diagnosis, the prevalent cases had more severe disease than incident cases. This could suggest a trend towards earlier diagnosis of CTEPH in recent years.
Strengths and limitations
Our study has several strengths. First of all, we present the results of the largest multicenter CTEPH registry recruiting patients in the modern era of CTEPH treatment, including pharmacological, surgical, and percutaneous methods. Second, by including all centers which diagnose and treat CTEPH patients we were able to estimate the incidence and prevalence of this disease. Third, we assessed the diagnostic value of lung V/Q scan and CTPA in real-world clinical practice.
The main limitation of our study is the risk of selection bias when we present the outcome results, as prevalent patients who died before 1 March 2018 could not be enrolled into our study. To reduce this risk we started the observation at enrollment to the study instead of at CTEPH diagnosis. The methodological limitations inherent to registry-based studies have recently been acknowledged. 53 We also acknowledge that due to a low number of end points, our survival analysis was not adjusted for confounding factors; for example, age, severity of CTEPH, and comorbid conditions which besides the treatment method could have impacted the status of the patients at follow-up.
Conclusions
The modern population of CTEPH patients comprises mostly elderly people significantly burdened with comorbid conditions. The combination of two or three therapeutic methods is currently a typical approach in the management of CTEPH. This calls for treatment decisions that are individually tailored to every patient.
Footnotes
Author contributions
GK is the guarantor of the paper and takes responsibility for the integrity of the work as a whole, from inception to publication. Conception and design: GK. Acquisition of data: all authors. Analysis and interpretation of data: GK, MW, WM, MK, PPr, WJ, EL. Drafting the manuscript: GK, WM, MW. Critical revision for intellectual content and final approval of the version to be published: all authors.
Conflict of interest statement
Grzegorz Kopeć reports grants and personal fees from Actelion Pharma, personal fees from Janssen-Cilag Polska, personal fees from AOP Orphan, personal fees from MSD. Olga Dzikowska-Diduch has nothing to declare. Ewa Mroczek has nothing to declare. Tatiana Mularek-Kubzdela reports fees for lectures from MSD, Bayer, Jansen, AOP Orphan, Beringher, Pfizer, grants from MSD, Bayer, Jansen, AOP Orphan, Beringher. Łukasz Chrzanowski reports fees for lectures from MSD, non-financial support from MSD. Ilona Skoczylas has nothing to declare. Michał Tomaszewski has nothing to declare. Małgorzata Peregud-Pogorzelska has nothing to declare. Danuta Karasek has nothing to declare. Ewa Lewicka reports fees for lectures from Bayer, MSD, AOP Orphan, Janssen-Cilag, Pfizer and Boehringer-Ingelheim. Wojciech Jacheć has nothing to declare. Zbigniew Gąsior has nothing to declare. Piotr Błaszczak has nothing to declare. Katarzyna Ptaszyńska-Kopczyńska has nothing to declare. Katarzyna Mizia-Stec has nothing to declare. Andrzej Biederman has nothing to declare. Dariusz Zieliński has nothing to declare. Roman Przybylski has nothing to declare. Piotr Kędzierski has nothing to declare. Marcin Waligóra has nothing to declare. Marek Roik has nothing to declare. Marek Grabka has nothing to declare. Joanna Orłowska has nothing to declare. Aleksander Araszkiewicz has nothing to declare. Marta Banaszkiewicz has nothing to declare. Sylwia Sławek-Szmyt has nothing to declare. Szymon Darocha reports grants and personal fees from Janssen-Cilag, MSD, Bayer, and AOP Orphan. Wojciech Magoń has nothing to declare. Alicja Dąbrowska-Kugacka reports fees for lectures from MSD, Actelion, AOP Orphan and Bayer. Jakub Stępniewski has nothing to declare. Kamil Jonas has nothing to declare. Karol Kamiński has nothing to declare. Jarosław D. Kasprzak reports fees for lectures from Janssen/Actelion, AOP Orphan. Piotr Podolec reports personal fees from Actelion, personal fees from Jansen, personal fees from AOP ORPHAN, personal fees from Bayer. Piotr Pruszczyk reports fees for lectures from Merck. Adam Torbicki reports grants and personal fees from Actelion Pharma, personal fees from Janssen-Cilag Polska, personal fees from AOP Orphan, personal fees from MSD, grants and personal fees from Bayer Healthcare and the Chairperson of the Foundation on Pulmonary Hypertension. The foundation receives donations including those from industry. The chairmanship is an honorary function and is unrelated to financial or other benefits. The funders had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results. Marcin Kurzyna reports fees for lectures from MSD, AOP Orphan and Janssen-Cilag.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Polish Cardiac Society.