
Abstract
Background:
The coronavirus disease 2019 (COVID-19) outbreak might have a psychological impact on frontline healthcare workers. However, the effectiveness of coping strategies was less reported.
Objectives:
We aimed to investigate the sources of stress and coping strategies among frontline healthcare workers fighting against COVID-19. We also performed a literature review regarding the effects of coping methods on psychological health in this population.
Methods:
We included frontline healthcare workers who completed an online survey using self-made psychological stress questionnaires in a cross-sectional study. We evaluated the association between potential factors and high-stressed status using a logistic regression model. We performed the principal component analysis with varimax rotation for factor analysis. We also performed a systematic review of published randomized controlled studies that reported the effects of coping methods on psychological health in COVID-19 healthcare workers.
Results:
We included 107 [32 (29–36) years] respondents in the final analysis, with a response rate of 80.5%. A total of 41 (38.3%) respondents were high-stressed. Compared with the low-stressed respondents, those with high-stress were less likely to be male (46.3% versus 72.7%, p = 0.006), nurses (36.6% versus 80.3%, p < 0.001), and more likely to have higher professional titles (p = 0.008). The sources of high-stress in frontline healthcare workers were categorized into ‘work factor’, ‘personal factor’, and ‘role factor’. A narrative synthesis of the randomized controlled studies revealed that most of the coping methods could improve the psychological stress in healthcare workers during the COVID-19 pandemic.
Conclusion:
Our findings suggest that some frontline healthcare workers experienced psychological stress during the early pandemic. Effective coping strategies are required to help relieve the stress in this population.
Introduction
Since the outbreak of coronavirus disease 2019 (COVID-19) in Wuhan, China, this new disease has infected more than 490 million people till 4 April 2022. 1 During the early pandemic period, more than 300 medical supporting teams with over 42,000 healthcare workers gathered in Wuhan to cope with the increasing crisis of COVID-19. Given the high infectivity of COVID-19 and the lack of effective treatment and preventive methods at that time, frontline healthcare workers in Wuhan were at high risk of being infected and developing psychological stress. The incidence of psychological crises associated with major disasters has been raised in previous studies. Among the 1621 severe acute respiratory syndrome (SARS) first-line medical staff in 2003, 68% experienced high-stress and 57% of them had psychological dysfunctions. 2 Risk factors for psychological stress in medical staff during the SARS outbreak might include the perception of the medical staff of their risk of infection, the impact of SARS on their work, feelings of depression, and working in high-risk medical units. 3 In the context of the present evolving COVID-19 pandemic, the psychological status among frontline healthcare workers requires particular attention. Moreover, COVID-19-related lockdowns might also have an impact on people’s living habits and behavioral risk factors. For example, preliminary data of the Lost in Italy project showed decreased smoking prevalence (from 23.3% to 21.9%) but increased prevalence of e-cigarette (from 8.1% to 9.1%) during the lockdown. 4 This project will contribute to establishing a comprehensive picture of societal, household, and individual-level changes due to the lockdown measures. 4 Moreover, there is a potential link between COVID-19 infection and negative clinical outcomes such as depression, and particularly suicidality, which is frequently underreported.5,6 An overview of the literature indicates that more than 2% of traffic accidents could be attributed to suicide behaviors. 7 The aforementioned studies raise a concern about COVID-19 infection–associated suicides and public health threats.
Although there are literature works aiming to investigate the factors for psychological stress in frontline healthcare workers,8–10 the effectiveness of coping strategies was less reported. A previous study showed that a digital learning package was appropriate and useful for the needs of healthcare workers in the United Kingdom. 11 Synthesizing the available information regarding the coping strategies might help to better support this population in dealing with the current pandemic. We hypothesized that well-designed intervention strategies might be helpful in coping with stress among frontline healthcare workers. We aimed to investigate the source of psychological stress in COVID-19 frontline healthcare workers and how they are coping in an online survey-based study. In addition, we conducted a narrative literature review of published randomized controlled trials (RCTs) that reported the effects of coping methods on psychological health in COVID-19 healthcare workers.
Methods
Survey-based study
Study overviews and subjects
This is a survey-based cross-sectional study. The electronic form of a self-made questionnaire delivered in Chinese was sent to the eligible participants through an online WeChat platform between 1 April and 14 April 2020. Each questionnaire has been anonymously protected. The study was approved by the local Ethics Committee. Written informed consent was obtained when the respondents completed and submitted their questionnaires. Doctors and nurses from Fujian medical team who had direct contact with COVID-19 patients in designated hospitals in Wuhan during the early pandemic were recruited for assessment. Team managers and heads were contacted to obtain lists of the staff members. A total of 133 frontline doctors and nurses who worked in Wuhan between 13 February and 30 March 2020 were identified.
Develop a questionnaire
From 1 March 2020, five medical students and two senior neurologists were involved in the design of this survey-based study. The preliminary questionnaire was initially developed by referring to the relevant literature and by consulting experts on health-related stress, 12 and was reviewed through qualitative work, focusing on the source of COVID-19 related stress, including working, human, and role factors. Quantitative analysis and discussion were performed on the scale changes, paring down, increase and improve the part of items about the source of stress. Feedback from pilot testing showed that respondents could readily understand what we were referring to. The final edition of the questionnaire includes five parts. The first part includes the demographics, including age, occupation, working years, marital status, and so on. The second part includes 16 items regarding the source of stress, reflecting the severity of psychological stress before and after the outbreak. The medical staff’s response to the severity of the stressors was assessed using a 3-point scale, ranging from ‘none’ to ‘severe’ (0 = none, 1 = moderate, 2 = severe). The third part includes 13 stress coping strategies, with the frequency ranging from ‘none’ (0) to ‘many times’ (3) on four Likert-type scales. The fourth part includes 11 questions about whether the medical staff have enough motivation for fighting against COVID-19 in Wuhan. The fifth section contains 11 questions about the change of the attitudes toward the positive and negative aspects of the outbreak, ranging from ‘strongly agree’ (1) to ‘common agree’ (3) to ‘disagree’ (4) to ‘uncertain’. Mean scores were obtained in questions based on the Likert-type scale. We defined ‘1 to 2’ as ‘agree’, ‘3 to 4’as ‘disagree’, and ‘5’ as ‘uncertain’ degree on the Likert-type scale. All fields were marked as mandatory, so a participant could not move forward unless all questions have been answered. Therefore, all participants completed the entire questionnaire without missing data.
Statistical analysis
Continuous variables were summarized as mean and standard variations or median with interquartile range (IQR), and categorical variables as frequencies with percentage, where appropriate. We compared the difference in continuous variables using the Mann–Whitney test and the difference in categorical variables using the Chi-square test or Fisher’s exact test as appropriate. Logistic regression analysis was used to identify the variables associated with high-stressed status. We performed the principal component analysis with varimax rotation for factor analysis. All statistical analyses were done using the statistical software package (SPSS 25,0, IBM).
Narrative synthesis of RCTs
Literature search and screening
We performed a systematic review of published RCTs using PubMed and the Cochrane Central Database from 2020 through to 28 March 2022, based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 11 Specifically, we aimed to identify original research that reported the effect of coping methods on psychological stress, mental health, or sleep quality. We used the following terms (‘Coronavirus’ OR ‘COVID-19’ OR ‘SARS-CoV-2’ OR ‘2019-nCoV’) AND (‘stress’ OR ‘psychological’ OR ‘psycho*’ OR ‘post-traumatic stress symptoms’ OR ‘depression’ OR ‘anxiety’ OR ‘burnout’) AND ( ‘healthcare workers’ OR ‘staff’ OR ‘doctor*’ OR ‘nurse*’ OR ‘physician’ OR ‘health personnel’). We also manually screened out the relevant potential article in the references selected to obtain a comprehensive list of studies. Literatures were eligible if they met the following criteria: (1) Original published RCTs involving healthcare workers regardless of language, race, and area. The intervention arm was coping strategies, and the controlled arm was placebo or comparator. We excluded observational studies (cohort studies, cross-sectional studies, case–control studies, case series, etc.), pooled analyses, reviews, meta-analysis, editorials, comments, conference papers, and those with insufficient or inaccurate data information provided.
Data extraction and methodological quality of included RCTs
Two authors blindly assessed study inclusion and quality, and extracted data on study characteristics (i.e. authors, date of publication, setting, sample size, and study design), participants’ characteristics (i.e. mean/median age and sex), inclusion and exclusion criteria, follow-up time points, and outcome measures using standardized data collection sheets. Data extractions were checked for accuracy by two authors. The frequency counts and measures of association for outcomes when reported were extracted. Disagreements and missing data were settled by team discussion. Two authors independently evaluated the quality of the included RCTs using the Cochrane Collaboration risk of bias tool. 13
Data available statement
The request to get access to data in this article should be addressed to the corresponding author.
Results
Demographics of the participants
Between 1 April and 14 April 2020, a total 133 questionnaires were sent out to the frontline healthcare workers of Fujian medical team supporting COVID-19 patients in Wuhan. We chose this period because these frontline healthcare workers were resting in a hotel after completing their tasks in Wuhan and returning to Fujian. Therefore, they would have adequate time and energy to respond to the survey. A total of 107 questionnaires (80.5%) were returned. Of these 107 respondents, 105 (98.1%) self-reported their physical health conditions as ‘good’, with only two (1.9%) ‘fair’. Ninety-eight (91.6%) respondents had directly contacted the COVID-19 patients in the isolation ward. The median score of stress of all respondents was 10 (IQR [7–12]). We therefore dichotomized respondents into low-stress (⩽10) and high-stress (>10). The demographic characteristics of participants with and without high-stress are shown in Table 1. A total of 41 (38.3%) respondents were assessed as high-stress. Compared with the low-stressed respondents, those with high-stress were less likely to be male (46.3% versus 72.7%, p = 0.006) and nurses (36.6% versus 80.3%, p < 0.001) and more likely to have higher professional titles (p = 0.008).
Demographic characteristics of participants with and without high-stress.

COVID, coronavirus disease 2019; IQR, interquartile range.
Evaluation of risk factors for high-stress status:
Supplemental Table 1 summarizes the association between the 16 factors and high-stress status using a univariable logistic regression model. All 16 factors were associated with high-stressed status (p < 0.001, respectively).
Comparison of the mean score of second-order factors of sources of stress
Factor analysis with orthogonal varimax rotation was carried out on the 16 items to determine the validity of the scale structure, with a Kaiser–Meyer–Olkin (KMO) = 0.914 m. The χ2 value was 1345.385 (degrees of freedom = 120) and significant (p < 0.001). The correlation matrix showed that the variables shared commonality and were appropriate for factor analysis. By means of factor analysis, three factors with eigenvalues greater than 1 were elicited (Supplemental Table 2). Factor analysis revealed three categorical factors: ‘work factor’, ‘personal factor’, and ‘role factor’. We found significant differences in all categorical stress factors between the participants with high- and low-stress (p < 0.001, respectively). The assessment of pressure sources in participants with low-stress was mild, compared with moderate in those with high-stress.
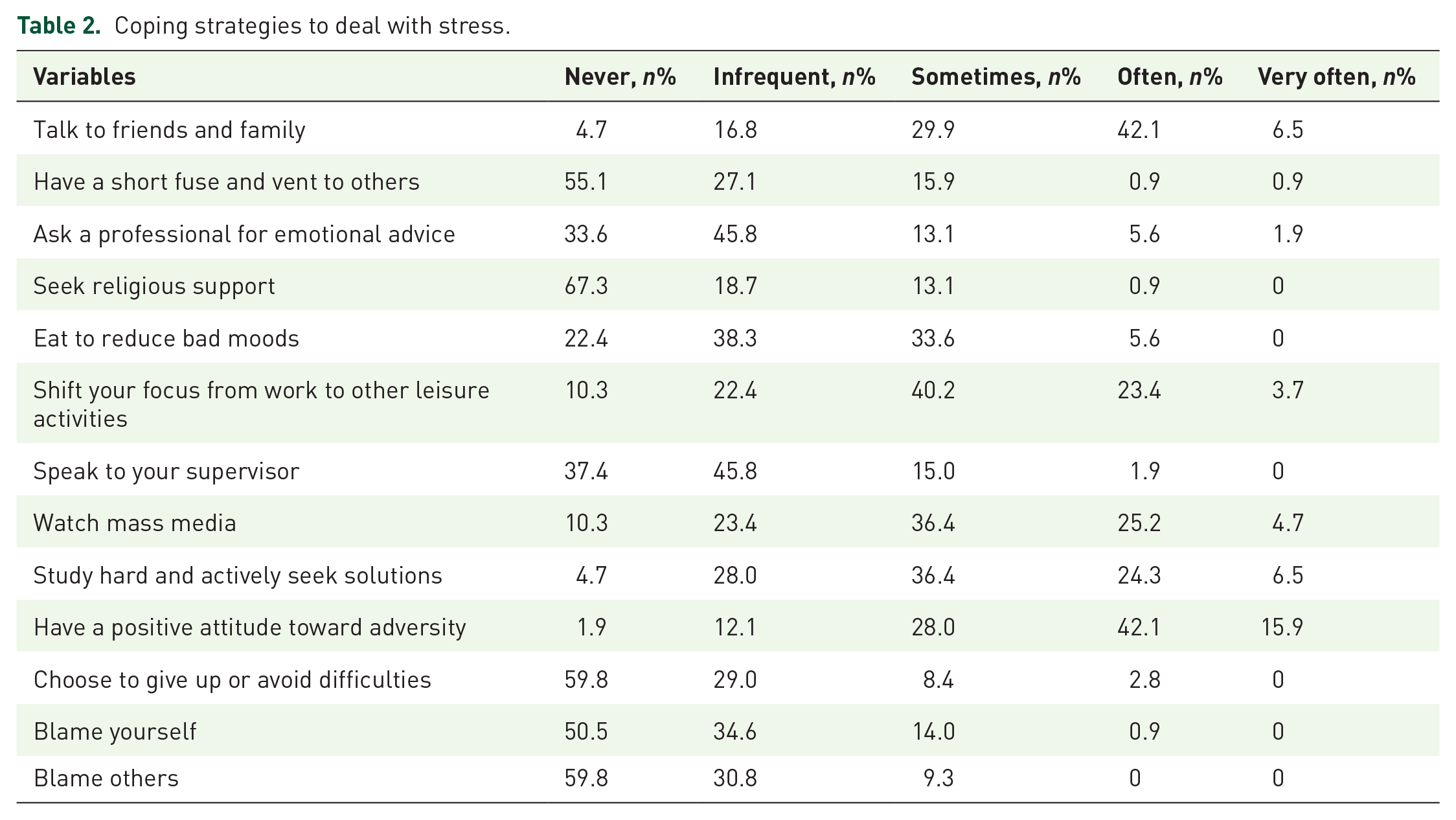
Strategies to deal with stress
The coping strategies are classified into four grades: infrequent, sometimes, often, and very often. Table 2 shows different coping strategies used by the respondents. Talking with friends or family members and having a positive attitude toward adversity were the most frequently used methods, followed by watching mass media, studying hard, and actively seeking solutions. In contrast, the most infrequently used strategies were having a short fuse and venting to others, seeking religious support, choosing to give up or avoid difficulties, and blaming oneself or others.
Coping strategies to deal with stress.
Changes in attitudes after the outbreak of COVID-19
The changes in life attitudes and personal values are shown in Supplemental Table 3. More than 90% of the respondents agreed to enhance their health awareness of the environment, believed to be more intimate with their colleagues, and were inclined to spend more time helping others avoid their own infections and were more sympathetic to the patients. Moreover, 102 (95.3%) respondents more valued gathering with family. Interestingly, the proportion of participants who agreed with the feeling that death is possible and unexpected, and fearing the disease and death were similar (data available on 106 participants).
Review results
A total of seven published RCTs14–20 met our inclusion criteria (Figure 1). Supplemental Table 4 summarizes the key characteristics of the included RCTs. The inclusion and exclusion of the included RCTs are shown in Supplemental Table 5. The sample size of eligible participants in all included studies ranged from 28 to 482. Four studies included nurses, one study included both nurses and therapists, and three included healthcare providers. The coping methods vary, including online interventional programs,14,16,17,19,20 video-based programs, 18 and pharmacological treatment. 15 Among all coping strategies, online programs were most frequently used, including an online ambulatory intervention (expressive writing, adaptive emotion regulation activity, and positive emotion-generation activities), an online mindfulness-based stress reduction program, an e-aid cognitive behavioral therapy, and a PsyCovidApp targeting emotional skills, healthy lifestyle behavior, burnout, and social support. The outcomes include symptoms or levels of anxiety, depression, stress, burnout, post-traumatic stress, and sleep quality. Table 3 and Supplementary Table 6 show that all the coping strategies significantly improved psychological stress or sleep quality. One study showed that cannabidiol (150 mg twice daily) reduced burnout and emotional exhaustion. 15 However, caution needs to be addressed to balance the benefits of cannabidiol therapy with potential undesired or adverse effects. The included RCTs’ quality was generally high (Figure 2). All included RCTs were single-centered, and the follow-up duration was relatively short (ranging from 7 to 90 days). Due to the high heterogeneous nature of intervention strategies and outcomes, we did not conduct a quantitative meta-analysis.

Flowchart of literature selection.
Purpose and main finding of included randomized controlled trials.

COVID, coronavirus disease 2019; ECBT-I, e-aid Cognitive Behavior Therapy; EFT, Emotional Freedom Techniques; MBSR, mindfulness-based stress reduction.

Reporting bias of RCTs assessed by Cochrane Collaboration’s tool.
Discussion
The present analysis has several important findings. First, our survey-based cross-sectional study showed that a considerable proportion of healthcare workers presented with psychological stress. Moreover, coping methods (i.e. talking with friends or family members) that were used in our participants had a positive attitude toward adversity. In addition, our review of available RCTs’ evidence showed that most of the coping methods could improve the psychological stress in healthcare workers during the COVID-19 pandemic. Our findings raise concerns about the psychological stress of healthcare workers involved in the COVID-19 crisis, suggesting timely psychological support and interventions for this population.
In our cohort, 41 (38.3%) frontline doctors and nurses experienced high-stress during their working in an isolation ward. A previous study showed that 26% of nurses reported mental health problems after they had worked in isolation wards for 7–10 days. 21 A national-level survey showed that 570 (27.3%) COVID-19 healthcare workers reported severe psychological distress. 22 Variations were observed probably depending on sample, regions, duration in isolation wards, and different assessment tools. Recently, Taylor et al. 12 developed 36-item COVID Stress Scales to measure fear of infection, fear of the socio-economic consequences of the pandemic, compulsive checking and reassurance-seeking regarding possible pandemic-related threats, and traumatic stress symptoms. The COVID Stress Scales were validated in large, population-representative samples in North America. Our scale shares similarities to some extent with the COVID Stress Scales established by Taylor et al. 12 Moreover, the validity of our scale structure showed that the variables were appropriate for factor analysis. Therefore, it might also provide evidence of a COVID-19-related stress syndrome. Our scale needs to be validated in future larger sample-size studies.
The psychological response of frontline healthcare workers to an epidemic of infectious diseases might be complicated. In line with previous studies,23–25 fear of being infected was a robust risk factor for a high-stress in our cohort. The death of medical workers due to inadequate personal protective measures in the early outbreak in Wuhan might cast a psychological shadow in frontline medical workers. Updated research on possible transmission approaches, such as aerosol transmission, might intensify the perception of personal danger of doctors and nurses working in an isolation ward. Previous studies showed that adequate protective facilities were helpful in alleviating the psychological disorders in a SARS crisis.26,27 Conversely, some researchers argued that wearing personal protective equipment for a long time may increase psychological stress.28,29 One study showed that wearing N95 facial mask for an 8-h shift had no obvious harmful effects on healthcare workers’ physiological health, compared with those who wore surgical facial mask. 30 However, the limited sample size did not have adequate statistical power to detect between-group differences in outcomes. More comprehensive studies that include a larger sample size of healthcare workers are needed to address this issue.
As a considerable proportion of healthcare workers may have anxiety, depression, and stress symptoms in relation to COVID-19, it is urgent to establish effective coping strategies that can address the need of this population. Previous studies found e-communication was associated with a reduced risk of isolation and psychological stress. 31 Healthcare workers are more likely to receive social support from family and workmates than from professional help. 32 Utilization of electronic media like digital learning packages, applications, and social media can be a popular approach to reducing psychological disorders in young and mid-aged healthcare workers. Our data showed that talking with friends or family members was the most frequently used method to alleviate respondents’ psychological stress. Convenient Internet access makes it easy for respondents to communicate with friends or family via mobile phone calls or video chats. Our review of available RCTs showed that among different coping methods for psychological stress, online programs were most widely used to improve the psychological stress or sleep quality in healthcare workers. Notably, the heterogeneity of intervention methods and outcomes did not allow us to conduct a meta-analysis. Future studies using quantitative analyses merit further study under pandemic conditions.
Limitations
We acknowledge limitations. First, our survey-based study is limited by the small sample size and reliance on self-report data. Second, participants in the current study were healthcare workers in Wuhan during the early pandemic; our findings might not be generalizable to all medical staff. However, the high response rate of the study sample might have been representative for frontline healthcare worker population during the COVID-19 pandemic. Third, the psychological stress was assessed using a self-reporting questionnaire, and our findings need to be validated in future large sample-size studies. However, all respondents self-reported their stress factors shortly after their working experience in Wuhan, which might minimize the recall bias. Fourth, our study and most of the previous studies on COVID-19 and mental health were cross-sectional, which may not accurately provide incremental changes in the mental health of healthcare workers. The follow-up duration of include RCTs was relatively short; future longitudinal designed studies are needed to assess changes in psychosocial responses over time. Finally, our literature review is limited because we could not perform the quantitative meta-analysis due to the heterogeneous coping method and outcomes of included RCTs.
Conclusion
Our findings showed that some frontline healthcare workers experienced high-stress during the early COVID-19 outbreak. Moreover, appropriate coping methods could improve the high-stress situation of frontline healthcare workers. Therefore, our study may provide valuable insight for policy-makers to pay attention to the COVID-19-related stress among frontline healthcare workers. We propose introducing easily accessible online-based programs as specific intervention strategies to provide timely psychological support for this specific population during the pandemic.
Supplemental Material
sj-docx-1-tar-10.1177_17534666221130215 – Supplemental material for Psychological stress and coping strategies among frontline healthcare workers supporting patients with coronavirus disease 2019: a retrospective study and literature review
Supplemental material, sj-docx-1-tar-10.1177_17534666221130215 for Psychological stress and coping strategies among frontline healthcare workers supporting patients with coronavirus disease 2019: a retrospective study and literature review by Xingyu Ding, Zihong Jian, Yiming Xu, Zibei Lin, Ziyang Chen, Yixian Zhang, Huayao Huang, Ronghua Chen, Pincang Xia, Wei Zhang and Houwei Du in Therapeutic Advances in Respiratory Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.