
Abstract
Oral corticosteroids (OCS) have long been a mainstay of treatment for asthma exacerbations and chronic severe asthma. However, it is increasingly recognized that both long-term and short-term OCS use are directly associated with a wide range of serious adverse effects, and as such OCS-sparing treatment alternatives are now widely recommended for patients with severe asthma. While several international guidelines recommend these treatments, guidance on OCS tapering, and which patients are most likely to tolerate OCS reduction and/or discontinuation, is still lacking. Several biologics have demonstrated efficacy in patients with OCS-dependent asthma. One OCS-sparing treatment is the anti-interleukin-5 monoclonal antibody mepolizumab, which is approved for the treatment of severe eosinophilic asthma. In addition to improved exacerbation rates, asthma control, quality of life, and lung function among patients with severe eosinophilic asthma, mepolizumab also has an OCS-sparing effect, which has been demonstrated in randomized controlled trials and real-world studies. Both physicians and patients express concerns about the adverse effects of OCS, and additional data from the randomized, controlled SIRIUS trial (NCT01691508) highlight the high level of concern among patients regarding OCS-related burden. In this article, we discuss current guidance on OCS-sparing strategies for patients with severe asthma, provide a summary of the available evidence of the OCS-sparing effect of mepolizumab, and highlight patient and physician perspectives on the use of OCS and OCS-sparing treatments in severe asthma.
Keywords
Introduction
Asthma is a common, heterogeneous respiratory disease, usually characterized by chronic airway inflammation.1,2 The goal of asthma treatment is to minimize the manifestations of asthma by appropriate therapeutic intervention, which hinges on the intrinsic severity of disease activity, the degree of control achieved, and the ease of controlling disease manifestations.3,4 Difficult-to-treat asthma is defined as asthma that is uncontrolled despite prescription of medium- or high-dose inhaled corticosteroid (ICS) with a second controller [usually long-acting β2-agonist (LABA)] or with maintenance oral corticosteroids (OCS), or that requires high-dose treatment to maintain good symptom control and reduce the risk of exacerbations. 2 Severe asthma, which affects around 3–10% of the general asthma population, is a subset of difficult-to-treat asthma defined as asthma uncontrolled despite adherence to maximal, optimized high-dose ICS/LABA therapy and management of contributory factors, or that worsens when high-dose treatment is decreased.2,5 Compared with mild or moderate asthma, patients with severe asthma have more exacerbations and comorbidities, 6 which are associated with an elevated risk of morbidity and mortality.7,8 Historically, guidelines have recommended escalation to maintenance OCS treatment for severe asthma, if control is not achieved with standard of care. 9 Reports suggest 20–60% of patients with severe or uncontrolled asthma use long-term OCS therapy, with use more likely in those with the greatest number of exacerbations.10,11 Short-term OCS therapy use (i.e. for < 30 days) 12 is more variable, with reports of use in 23–93% of patients with severe or difficult-to-treat asthma, and patients with increasing disease severity were more likely to receive short-term OCS therapy. 10
Maintenance OCS use is associated with a wide range of well-recognized and serious short- and long-term adverse events (AEs), including weight gain, diabetes, osteoporosis, cataracts, hypertension, and adrenal suppression as well as increased risk of mortality.2,10,13–22 Psychological AEs, such as depression and anxiety, have also been reported by patients on OCS therapy. 23 Increasing OCS exposure has a statistically significant dose-dependent relationship with the risk of developing either acute or chronic OCS-related complications.14,20,24 This risk is also present with OCS exposures as low as ⩽1 mg/day,22,25,26 with each OCS prescription adding a cumulative burden on current and future health, regardless of dose and duration. 27 This is particularly pertinent for patients with severe asthma as OCS can also be used to treat comorbidities such as chronic rhinosinusitis with nasal polyps; 28 as such, multiple different specialists may be prescribing short-term OCS therapy. Indeed, even short-term OCS use is associated with sleep disturbance and an increased risk of infections, bone fractures, and thromboembolism, 12 and OCS bursts (OCS use for ⩽14 days) are associated with increased risk of gastrointestinal bleeding, sepsis, and heart failure within a month after treatment initiation. 29 Notably, the benefit of reducing long-term OCS may often be countered by an increased need for short-term OCS, 30 as any reduction in OCS use must be balanced with the risk of asthma exacerbations requiring rescue therapy. Overall, OCS use is a major contributor to the substantial risk among patients with severe asthma, worsening prognosis and potentially reducing life expectancy.23,31,32 As such, the development of strategies to decrease OCS exposure in patients with severe asthma has been a high priority for several decades, with replacement of OCS with alternative treatments, such as ICS, identified as a goal as early as 1973.2,25,33,34
Several biologic therapies developed for the treatment of severe asthma have been shown to have OCS-sparing effects.35–39 One such therapy is mepolizumab, a humanized monoclonal antibody approved in multiple regions worldwide for the treatment of severe eosinophilic asthma,40,41 an endophenotype of severe asthma characterized by eosinophilic inflammation and frequent exacerbations. 42 Mepolizumab is also approved for the treatment of eosinophilic granulomatosis with polyangiitis, hypereosinophilic syndrome, and chronic rhinosinusitis with nasal polyps.41,43 Mepolizumab binds to and inactivates interleukin 5 (IL-5), thereby blocking the proliferation, activation, and survival of eosinophils, and is associated with a range of clinical benefits in patients with severe eosinophilic asthma. 44 Notably, prednisolone treatment has also been associated with reduced expression of IL-5 mRNA in bronchial biopsies from patients with asthma. 45 As such, both OCS and mepolizumab have an anti-IL-5 effect.44,46 Here, we discuss current guidance on OCS-sparing strategies for patients with severe asthma, provide a summary of evidence of the OCS-sparing effect of mepolizumab, and highlight patient and physician perspectives on the use of OCS and OCS-sparing treatments in severe asthma.
Current clinical guidelines and patient views on the role of OCS and biologic therapies in severe asthma management
Current guidelines support the need to consider alternative treatment strategies to the use of OCS for patients with severe asthma, and anti-IL-5 therapies, anti-immunoglobulin E (IgE) therapy, and/or anti-IL-4/13 therapies are widely recommended (Table 1). From a patient’s perspective, the 2018 OCS Stewardship Statement underscores the urgent need to educate patients and healthcare providers about OCS-associated risks and protect patients from potential OCS overexposure, by suggesting OCS-sparing strategies. 21 Together with the consistent recommendations in asthma guidelines to reduce OCS use, the Stewardship Statement demonstrates the growing appreciation of the detrimental effects of both short- and long-term OCS use in patients with severe asthma. As such, strategies to minimize OCS use should be pursued as a high priority.
Guideline recommendations for OCS and biologic use for adults with severe asthma.

AEs, adverse events; ATS, American Thoracic Society; EAACI, European Academy of Allergy and Clinical Immunology; ERS, European Respiratory Society; FeNO, fractional exhaled nitric oxide; GINA, Global Initiative for Asthma; ICS, inhaled corticosteroid; IgE, immunoglobulin E; IL, interleukin; LABA, long-acting beta2-agonist; LAMA, long-acting muscarinic antagonist; NHLBI, National Heart, Lung, and Blood Institute; OCS, oral corticosteroid; ppb, parts per billion; SABA, short-acting beta2-agonist.
Panel were uncertain that the desirable consequences of the intervention outweighed the undesirable consequences based on low-quality evidence or the study populations not uniformly meeting ERS/ATS severe asthma criteria.
Determined by a blood eosinophil count ⩾ 300 cells/µl in the past 12 months, or ⩾ 150 cells/µl at treatment initiation.
Defined as inadequately controlled asthma, receiving ⩾ medium dose of ICS with/without another controller, including OCS, and ⩾ 1 blood eosinophil count ⩾ 400 cells/µl during a 2-4-week screening.
Uncontrolled by high-dose ICS + LABA with a baseline blood eosinophil count > 300 cells/µl (> 150 cells/µl for OCS-dependent patients).
Uncontrolled by medium-/high-dose ICS plus up to two additional controllers (including OCS), with T2 inflammation characterized by blood eosinophil count > 150 cells/µl and/or FeNO levels > 20 ppb.
With a total IgE level of 30–700 IU/ml (US) and 30–1500 IU/ml (EU) ± one perennial aeroallergen.
With FeNO ⩾ 24 ppb and blood eosinophil count ⩾ 260 cells/µl.
The systematic review that informed the report did not include studies that examined the role of asthma biologics.
Step 5: Daily medium-high dose ICS-LABA + LAMA and as-needed SABA; step 6: Daily high-dose ICS-LABA + oral systemic corticosteroids + as-needed SABA.
Strategies for and goals of OCS tapering
While there is broad consensus on the need to minimize OCS use in patients with severe asthma, guidance on the strategies for, and goals of, OCS tapering in this population is lacking. In a recent Delphi world expert consensus, experts agreed that OCS tapering should be attempted in all patients with asthma who are receiving maintenance OCS therapy. 50 Furthermore, there was almost 80% agreement that OCS cessation should be implemented when there is no evidence of adrenal insufficiency. 50 The schedule and speed of OCS tapering should be determined by the needs of each individual patient, and based on factors such as duration of previous maintenance OCS, and history and future risk of AEs. 50 However, the minimum target dose for such tapering remains unclear. The European Academy of Allergy and Clinical Immunology (EAACI) guidelines and the Delphi consensus recommend a minimally important reduction of 50% in OCS dose and failure to achieve this may warrant switching strategies.48,50 We suggest that, while not every patient will be able to omit OCS use completely, any reduction in dose or frequency of use should be a treatment goal for patients with severe asthma, with the aim of reducing the daily dose to around physiological levels (i.e. prednisolone equivalent of ⩽5.0 mg/day). 51 Notably, biologics should play an important role in OCS tapering. 50
Evidence supporting the OCS-sparing effect of mepolizumab in patients with severe eosinophilic asthma
Mepolizumab has been approved for the treatment of severe eosinophilic asthma since 2015. 41 A wealth of data have now accumulated from randomized controlled trials, supported by a growing body of evidence from real-world studies, which together demonstrate the efficacy and safety of mepolizumab in patients with severe eosinophilic asthma, as well as its OCS-sparing effect (Table 2).
Design and outcomes of OCS-sparing mepolizumab clinical trials and real-world studies.
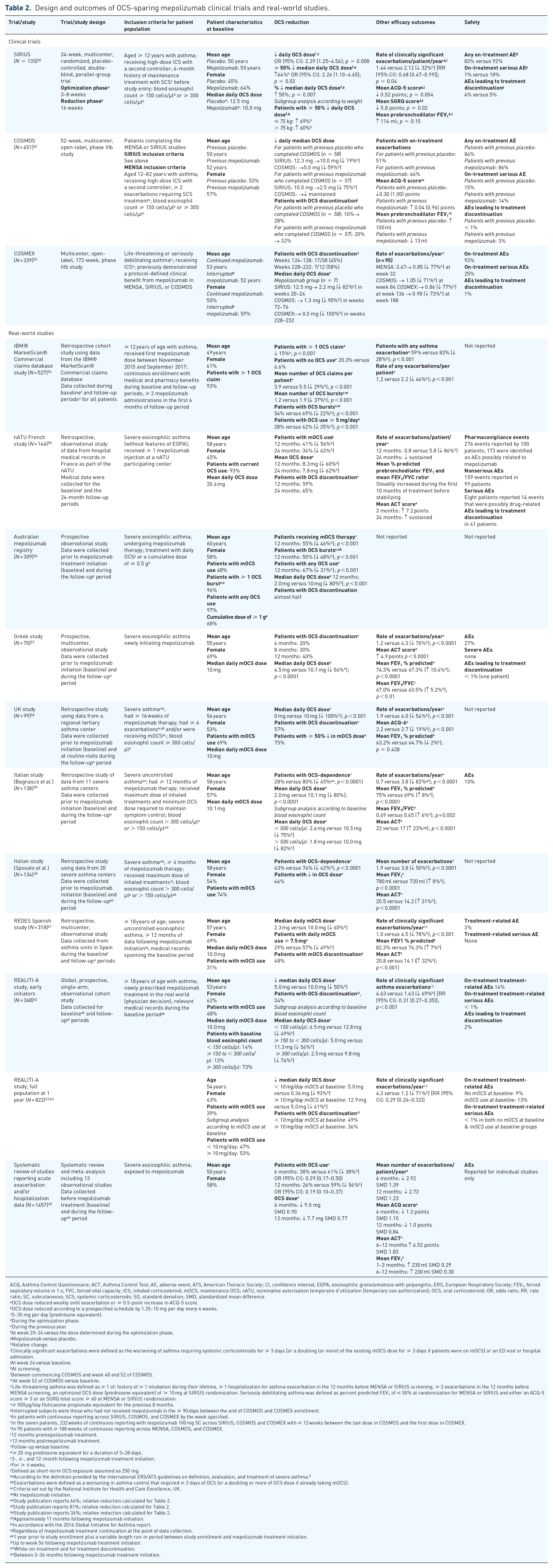
ACQ, Asthma Control Questionnaire; ACT, Asthma Control Test; AE, adverse event; ATS, American Thoracic Society; CI, confidence interval; EGPA, eosinophilic granulomatosis with polyangiitis; ERS, European Respiratory Society; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; ICS, inhaled corticosteroid; mOCS, maintenance OCS; nATU, nominative autorisation temporaire d’utilization [temporary use authorization]; OCS, oral corticosteroid; OR, odds ratio; RR, rate ratio; SC, subcutaneous; SCS, systemic corticosteroids; SD, standard deviation; SMD, standardized mean difference.
OCS dose reduced weekly until exacerbation or ⩾ 0.5-point increase in ACQ-5 score.
OCS dose reduced according to a prespecified schedule by 1.25–10 mg per day every 4 weeks.
5–35 mg per day (prednisone equivalent).
During the optimization phase.
During the previous year.
At week 20–24 versus the dose determined during the optimization phase.
Mepolizumab versus placebo.
Relative change.
Clinically significant exacerbations were defined as the worsening of asthma requiring systemic corticosteroids for ⩾ 3 days [or a doubling (or more) of the existing mOCS dose for ⩾ 3 days if patients were on mOCS] or an ED visit or hospital admission.
At week 24 versus baseline.
At screening.
Between commencing COSMOS and week 48 and 52 of COSMOS.
At week 52 of COSMOS versus baseline.
Life-threatening asthma was defined as ⩾ 1 of: history of ⩾ 1 intubation during their lifetime, ⩾ 1 hospitalization for asthma exacerbation in the 12 months before MENSA or SIRIUS screening, ⩾ 3 exacerbations in the 12 months before MENSA screening, an optimized OCS dose (prednisone equivalent) of ⩾ 10 mg at SIRIUS randomization. Seriously debilitating asthma was defined as percent predicted FEV1 of ⩽ 50% at randomization for MENSA or SIRIUS and either an ACQ-5 score ⩾ 3 or an SGRQ total score ⩾ 60 at MENSA or SIRIUS randomization.
⩾ 500 µg/day fluticasone propionate equivalent for the previous 8 months.
Interrupted subjects were those who had not received mepolizumab in the ⩾ 90 days between the end of COSMOS and COSMEX enrollment.
In patients with continuous reporting across SIRIUS, COSMOS, and COSMEX by the week specified.
In the seven patients, 232 weeks of continuous reporting with mepolizumab 100 mg SC across SIRIUS, COSMOS and COSMEX with ⩽ 12 weeks between the last dose in COSMOS and the first dose in COSMEX.
In 95 patients with ⩾ 188 weeks of continuous reporting across MENSA, COSMOS, and COSMEX.
12 months premepolizumab treatment.
12 months postmepolizumab treatment.
Follow-up versus baseline.
⩾ 20 mg prednisone equivalent for a duration of 3‒28 days.
3-, 6-, and 12-month following mepolizumab treatment initiation.
For ⩾ 6 weeks.
Defined as short-term OCS exposure assumed as 250 mg.
According to the definition provided by the International ERS/ATS guidelines on definition, evaluation, and treatment of severe asthma. 5
Exacerbations were defined as a worsening in asthma control that required ⩾ 3 days of OCS (or a doubling or more of OCS dose if already taking mOCS).
Criteria set out by the National Institute for Health and Care Excellence, UK.
At mepolizumab initiation.
Study publication reports 66%; relative reduction calculated for Table 2.
Study publication reports 81%; relative reduction calculated for Table 2.
Study publication reports 34%; relative reduction calculated for Table 2.
Approximately 11 months following mepolizumab initiation.
In accordance with the 2016 Global Initiative for Asthma report.
Regardless of mepolizumab treatment continuation at the point of data collection.
1 year prior to study enrollment plus a variable length run-in period between study enrollment and mepolizumab treatment initiation.
Up to week 56 following mepolizumab treatment initiation.
While-on-treatment and for treatment discontinuation.
Between 3–36 months following mepolizumab treatment initiation.
Clinical trial data
SIRIUS (NCT01691508) was the first randomized trial to use a biologic (mepolizumab) to target OCS reduction by reducing eosinophil counts in severe eosinophilic asthma. 35 To determine the true minimum OCS dose required for disease control, patients’ OCS dose was reduced during an optimization phase before randomization. Following randomization to either mepolizumab 100 mg subcutaneous or placebo, OCS doses were tapered based on a prespecified algorithm if asthma control was maintained and there were no symptoms of adrenal insufficiency. The trial showed significantly greater reductions in maintenance OCS dose in patients receiving mepolizumab versus those receiving placebo, independent of patient weight (Table 2), with median daily OCS dose falling by 69% (10.0–3.1 mg) at week 24 in the 66 patients in the mepolizumab group who reached week 20–24 of the study (Figure 1). Furthermore, patients treated with mepolizumab had fewer exacerbations and significant improvements in asthma control and quality of life versus those on placebo, even with the clinically relevant reduction in OCS dose (Table 2). Notably, the median percentage reduction in daily OCS dose in the SIRIUS placebo arm was 0%. This reduction was in contrast to VENTURE (dupilumab; 50%) and ZONDA (benralizumab; 25%) suggesting a placebo effect in those trials, which needs to be accounted for when considering the reduction in the active treatment arm of these studies.37,38 These data demonstrate the effectiveness of the SIRIUS optimization phase in reducing OCS to the lowest effective dose. SIRIUS demonstrated that significant and clinically relevant OCS reductions were possible with mepolizumab not only without a loss of asthma control but with concomitant clinical improvements. Overall, 54% of patients on mepolizumab had a clinically meaningful reduction in their OCS dose (⩾ 50%48,50) and 14% were able to discontinue OCS therapy in this short-term trial with only a 16-week period of dose reduction; 35 however, longer and larger trials were needed to determine the plausibility and long-term effects of complete OCS withdrawal.
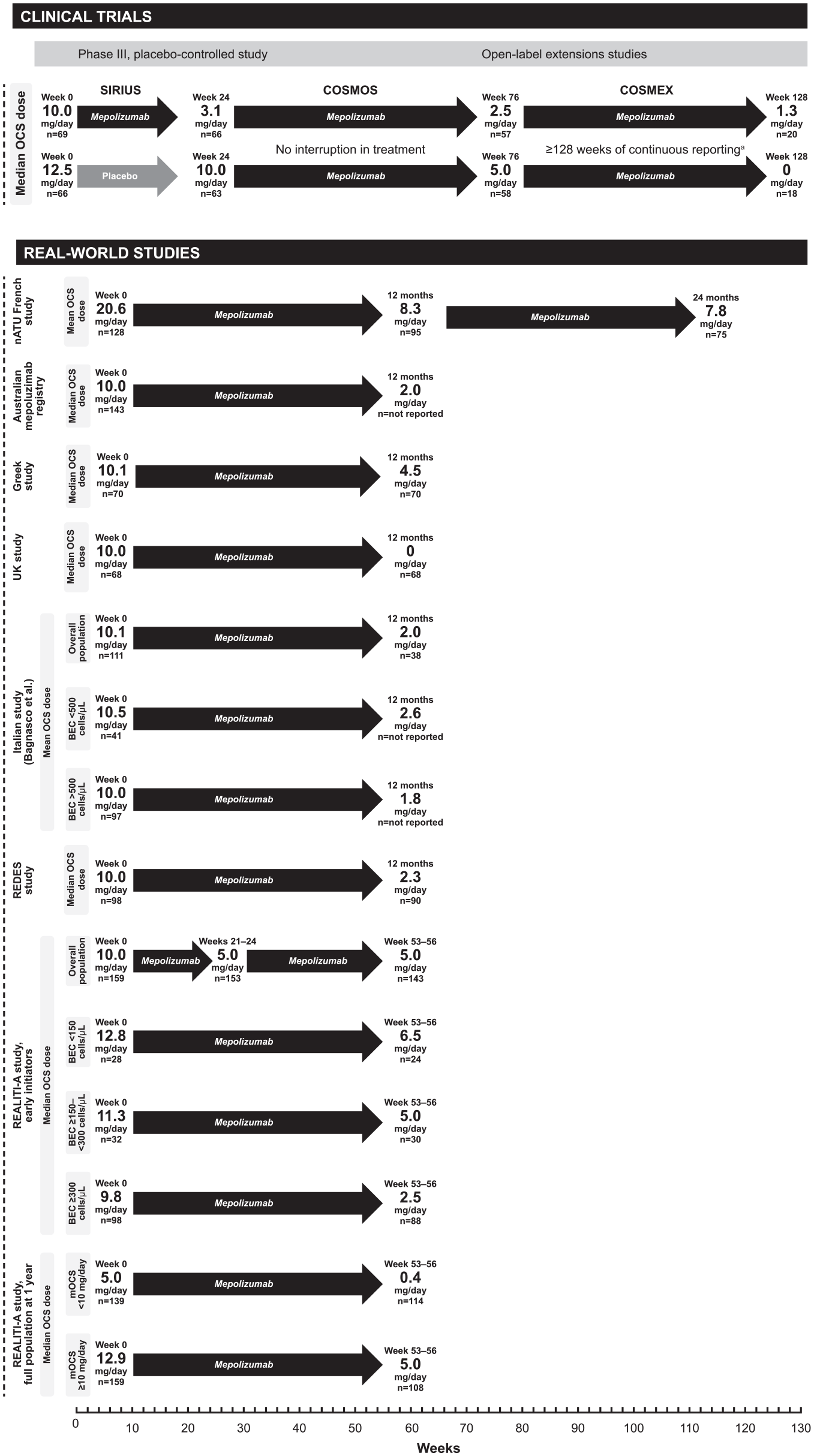
OCS dose reductions in clinical trials and real-world studies.
Such long-term data were obtained from the COSMOS (NCT01842607) 52-week, open-label extension (OLE) trial, 52 which enrolled patients with severe eosinophilic asthma who had previously received mepolizumab or placebo in the MENSA 66 or SIRIUS 35 trials (Table 2). In contrast to the protocol-defined OCS reduction schedule in SIRIUS, OCS tapering in COSMOS was at the discretion of the physician. The median daily OCS dose achieved with mepolizumab during SIRIUS was further reduced among patients who completed the open-label period of COSMOS (Figure 1). In addition, by weeks 48 to 52 of COSMOS, a further 18% of patients previously on placebo and 12% of patients previously on mepolizumab were no longer receiving OCS treatment versus the beginning of the COSMOS trial (Table 2). These results further supported a clinically meaningful mepolizumab-induced OCS dose reduction in SIRIUS, indicated a durable and stable effect over time, and highlighted that OCS discontinuation is not possible in all patients. Importantly, as OCS reduction was based on physician judgment and as the trial was open label, the dose reductions seen may better reflect what could be achieved in clinical practice versus those seen during SIRIUS.
Further evidence on the long-term OCS-sparing effects of mepolizumab was obtained from the 172-week OLE COSMEX (NCT02135692) trial. COSMEX enrolled patients from COSMOS who had been assessed as having protocol-defined life-threatening or seriously debilitating asthma before entry into their first mepolizumab trial (Table 2) and patients remained in COSMEX until they could begin commercially available mepolizumab in their participating country. 53 As such, the duration of follow-up varied. While the main aim of this trial was to assess the long-term safety and efficacy of mepolizumab in patients with the most severe eosinophilic asthma, daily OCS use was assessed as a secondary endpoint. Among 38 patients (placebo, n = 18; mepolizumab, n = 20 in the initial SIRIUS study) with ⩾ 128 weeks of continuous reporting across SIRIUS, COSMOS, and COSMEX and ⩽ 12 weeks between their last COSMOS dose and first COSMEX dose, there was a sustained reduction in daily OCS dose (Table 2 and Figure 1). In addition, 17/38 (45%) patients were able to discontinue OCS use during COSMEX. These data support the use of mepolizumab as a long-term, effective OCS-sparing treatment choice and suggest that there is potential for a slow progressive tapering of OCS therapy with long-term mepolizumab, even in those with the most severe asthma.
Real-world data
Initial real-world evidence on the OCS-sparing effect of mepolizumab came from a retrospective cohort study conducted between 2015 and 2017 [GSK ID: 209642 (HO-19-19597)], 54 which assessed outcomes in the 12 months following versus the 12 months before mepolizumab initiation (Table 2). The OCS-sparing effect of mepolizumab was demonstrated by a reduced proportion of patients with ⩾ 1 OCS claim, a lower mean number of OCS bursts, and a lower proportion of patients with chronic OCS use (Table 2). Furthermore, the proportion of patients discontinuing OCS increased by 14% between pretreatment and follow-up (p < 0.001) (Table 2).
Reductions in OCS use were also shown in a retrospective, observational study conducted in 2015–2016 in France [nATU; GSK ID: 207943 (HO-17-18317)]. 55 Data from patients with severe eosinophilic asthma were collected for 24 months following mepolizumab initiation. Notably, while 93% of patients were using OCS at baseline, there was a 62% reduction in the proportion of patients using OCS following 24 months of mepolizumab treatment (Table 2). Patients who still required OCS during follow-up needed lower doses at month 24 versus baseline (mean: 7.8 mg/day versus 20.6 mg/day) 55 and these lower OCS doses were consistent with those reported for corticosteroid replacement for adrenal insufficiency. 67 As seen in the clinical trials, reductions in OCS use were accompanied by improvements in exacerbation rate, lung function, and asthma control (Table 2).
Several other regional real-world studies, conducted across Australia, Greece, United Kingdom, Italy, and Spain also showed the OCS-sparing effect of mepolizumab in patients with severe eosinophilic asthma (Table 2).56–61 In addition, the Australian study identified baseline predictors of OCS discontinuation after 6 months of mepolizumab treatment. These were lower body mass index (BMI) [odds ratio (95% confidence interval): 0.93 (0.87–0.98); p = 0.009], late-onset asthma [1.03 (1.01–1.05); p = 0.010], and a lower Asthma Control Test score [1.11 (1.01–1.22); p = 0.028]. 56
REALITI-A is the largest 24-month, prospective, international, observational study (GSK ID: 204710), which collected data from routine healthcare visits from patients with asthma enrolled between December 2016 and October 2019. 62 The data from the early trial initiators (N = 368) showed a 50% reduction in the median daily maintenance OCS dose following mepolizumab treatment at 1 year (Figure 1); similar reductions were also seen across baseline blood eosinophil subgroups (Figure 1 and Table 2). Using data from the full study population at 1 year (N = 822), a subgroup analysis by baseline maintenance OCS dose thresholds showed that, following mepolizumab treatment, a 93% reduction in median daily OCS dose was observed in patients with a baseline maintenance OCS dose < 10 mg/day, with 49% of these patients discontinuing OCS use (Figure 1 and Table 2).
Together these studies demonstrated that the OCS-sparing effects of mepolizumab seen in clinical trials were extended to a real-world clinical setting. Indeed, a recent systematic literature review of 13 real-world studies showed that patients were much less likely to require OCS following 6 or 12 months of mepolizumab treatment; OCS doses were significantly decreased after 6 (9.0 mg reduction) and 12 months (7.7 mg reduction) of treatment (Table 2). 65 Further information on the use of biomarkers to predict the likelihood of OCS reduction in individual patients is needed; additional work should focus on facilitating tailored and optimized OCS tapering among patients with severe asthma.
Lessons from OCS-sparing trials and real-world data
Phase III, controlled studies assessing formal OCS reduction with mepolizumab are limited to SIRIUS; however, a much greater wealth of data spanning a longer time period are available from extension and real-world studies. The real-world data have been collated in clinically relevant settings in which OCS reductions are likely to have been tailored to individual patients rather than being conducted based on formal algorithms. Together with the data from SIRIUS, the real-world studies to date have demonstrated sustained OCS-sparing effects with mepolizumab that span a range of patients with differing clinical characteristics and disease severities, providing important information for clinicians managing patients with severe disease. The studies also demonstrate that complete OCS discontinuation is not possible in all patients, but clinically meaningful reductions can often be achieved. While it is recognized that adrenal insufficiency can contribute to the need for maintenance of OCS therapy among patients with severe asthma, 50 further information on the characteristics of those without adrenal insufficiency who are most likely to be able to discontinue OCS would be clinically useful. The Australian mepolizumab registry study 56 associated lower BMI and optimized asthma control with a greater likelihood of discontinuing OCS use in clinical practice, although these characteristics may also indicate less severe disease where OCS treatment is less widely utilized. However, the characteristics of patients most likely to tolerate OCS discontinuation require further investigation. Importantly, as mepolizumab was the first approved anti-eosinophilic biologic with proven OCS-sparing capabilities, it is likely that in real-world practice, patients with the most severe disease and the longest duration of OCS therapy would have been initiated on mepolizumab. This should be considered when interpreting these real-world outcomes.
OCS-sparing treatments at the patient and physician level
To date, there has been little focus on the direct impact of OCS reductions on a patient level. Furthermore, the concerns of healthcare professionals relating to OCS use, such as maintaining asthma control and reducing AE burden, are also important considerations. Additional data from SIRIUS provide insights into the burden of worry associated with OCS use among patients and the burden of OCS-related AEs in this population.
OCS use from the patient’s perspective
The real-world benefit of OCS reduction on patient’s perception on quality of life has been demonstrated in patients who have discontinued OCS use following biologic treatment; these improvements in quality of life were paralleled by progressive mood improvements over time. 68 During SIRIUS, patients completed a Steroid Perception Questionnaire (Supplementary materials), which assessed the levels of concern (‘worry’) regarding daily OCS use. Responses showed that a high proportion of patients were ‘very worried’ or ‘extremely worried’ about OCS side effects, including cataracts, bone fracture, and weight gain, both prior to and following 24 weeks of treatment (Table 3), emphasizing the importance of minimizing OCS use at a patient level. In addition, at baseline, 112/134 (84%) patients reported that they were worried about the side effects of long-term OCS use and 85/134 (63%) patients had talked with their physician regarding their concerns surrounding OCS use. These findings align with recent literature reviews that highlighted a wide range of OCS-related side effects, even with brief exposure to OCS, and these side effects worried patients.22,69 Furthermore, patients had low levels of satisfaction with the information provided by healthcare professionals regarding OCS-related side effects. Overall, these factors contributed to high levels of poor OCS treatment adherence. 69
High level of worry responses a in the Steroid Perception Questionnaire at baseline and week 24 (ITT population).

ITT, intent-to-treat; SC, subcutaneous.
Responses were ‘very worried’ or ‘extremely worried’.
Sixty-four patients had data available at week 24.
OCS use from the physician’s perspective
Of great clinical interest are the trial outcomes assessing patients who were able to reduce their OCS usage by ⩾ 50% or discontinue completely versus those who continued OCS alongside their study treatment. These data will provide information for physicians regarding the likelihood of patients tolerating OCS reduction or discontinuation.
In the SIRIUS trial, evaluation of asthma control in patients who were not able to decrease OCS was difficult to assess, as reducing OCS dose was dependent on maintaining asthma control. Nonetheless, between weeks 0 and 4, during which time OCS use was stable, an improvement in asthma control was achieved with mepolizumab versus placebo (least squares mean change in ACQ-5 score: −0.47 versus 0.02; treatment difference: −0.49; p < 0.001) and this improvement was maintained for the duration of the study. Further analysis of clinical trial outcomes according to OCS reduction will be useful and may provide valuable clinical information regarding the effect of OCS tapering on disease control.
On-treatment AEs potentially related to OCS use were reported in 27/135 (20%) patients during SIRIUS (Table 4). Information on the timing of these AEs in relation to OCS dose reduction and whether they led to discontinuation was not available; collation of these details would be useful in any future work. One of the most common steroid-related medical conditions experienced by patients at enrollment into the SIRIUS study included weight gain. Despite this, patients experienced minimal mean change in weight in the mepolizumab (0.2 kg) or placebo (−0.6 kg) groups from baseline to week 24. These data highlight the concern surrounding OCS use among patients with severe asthma and add to the existing reports of AE burden associated with OCS use.2,10,13–21 Together, this evidence supports the goal of reducing, or discontinuing where possible, OCS treatment in this population and further emphasizes the need for OCS-sparing treatment alternatives such as mepolizumab.
Summary of on-treatment AEs potentially associated with OCS toxicity in the SIRIUS trial (ITT population).
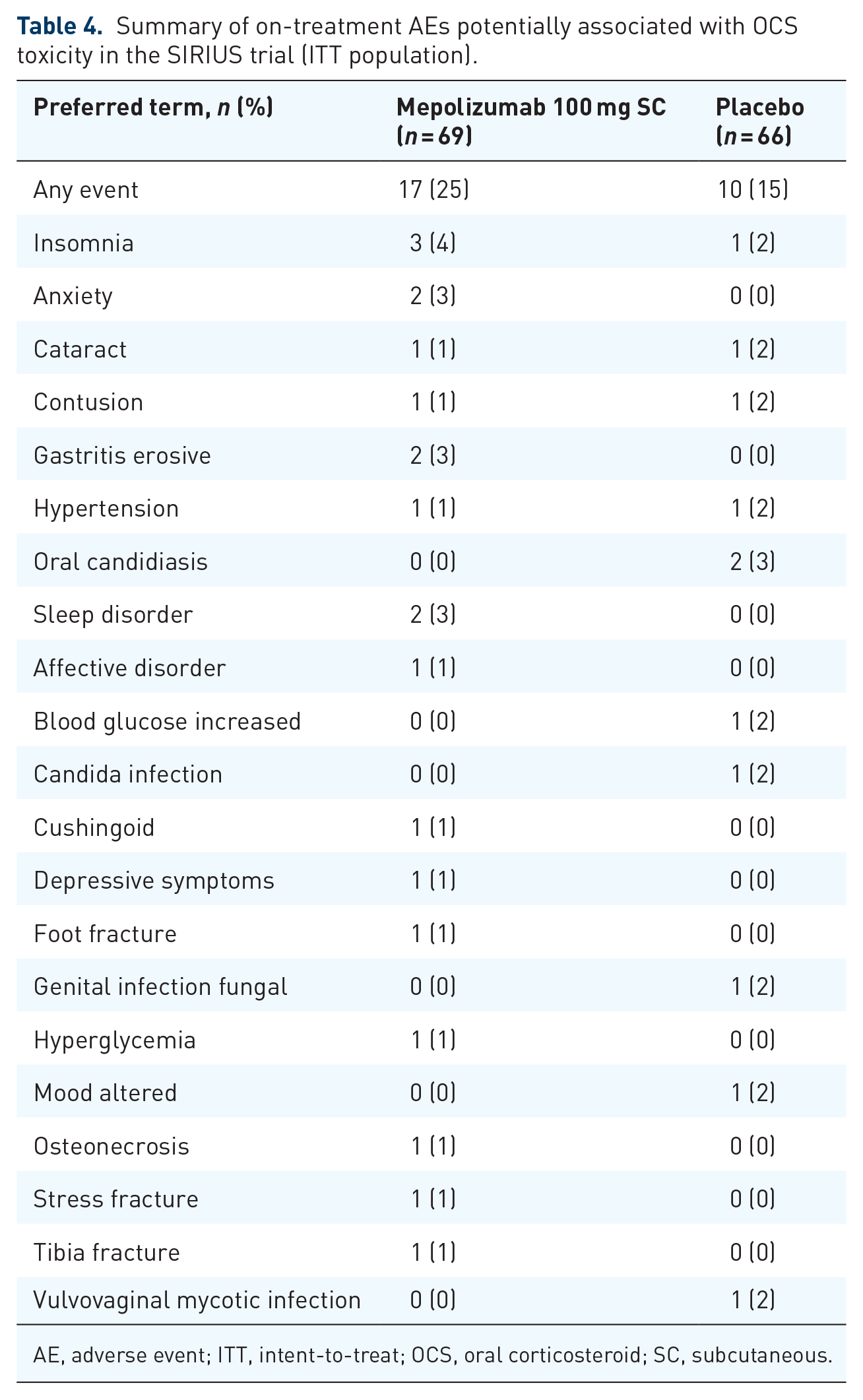
AE, adverse event; ITT, intent-to-treat; OCS, oral corticosteroid; SC, subcutaneous.
Future directions and important unanswered questions
While the success of OCS tapering and the associated benefits have been demonstrated in mepolizumab trials and real-world settings, there are some important avenues of further investigation to ensure that reducing OCS use is widely achievable. Importantly, OCS tapering should be attempted in all patients with asthma receiving maintenance OCS therapy and any attempted reduction in OCS should be tailored to individual patients to ensure safety and optimize effectiveness. 50 However, as evidenced in the SIRIUS study, 35 OCS discontinuation is not always achievable. As such, information regarding the clinical characteristics of patients most likely to tolerate OCS dose reduction would be useful. There is some evidence that patients with high baseline doses of OCS and those who have received OCS treatment for ⩾ 1 year achieve smaller OCS dose reductions than patients who are not in these categories. 70 Furthermore, clinical factors such as adrenal insufficiency, suboptimal treatment guideline adherence, the presence of eosinophilic granulomatosis with polyangiitis, under-recognition of the cumulative burden of OCS, and the lack of a standardized approach for OCS tapering can hamper OCS reduction.47,50,71 Likewise, patients with a non-type 2 asthma endotype may be refractory to OCS treatment and are unlikely to benefit from biologics that target components of the type 2 pathway. 72 It would be interesting to assess the size of the impact of adrenal insufficiency on the OCS-sparing effect of mepolizumab in real-world populations. The development of treatment guidelines that shepherd tailored and effective OCS dose tapering73,74 after biologic therapy initiation is a priority and more formal algorithms that assess adrenal insufficiency as part of the OCS reduction protocol have been developed. 71 However, even with prolonged attempts to reduce OCS, it is apparent that not all biologic add-on therapy in severe asthma is effective in enabling a dose reduction in OCS therapy.35,37,75
It will also be important to determine whether any OCS reductions achieved during biologic therapy use are sufficient to prevent or at least decrease the incidence of OCS-related AEs; studies to evaluate this are beginning. 76 Finally, it will be important to determine whether the OCS-sparing effect of mepolizumab extends to other eosinophilic diseases, such as eosinophilic granulomatosis with polyangiitis, hypereosinophilic syndrome, and chronic rhinosinusitis with nasal polyps, in which the clinical benefits of mepolizumab have already been shown.
Conclusions
In both randomized clinical trials and real-world studies, mepolizumab therapy resulted in clinically significant reductions in maintenance OCS use that were associated with clinical benefits in patients with severe eosinophilic asthma. Use of mepolizumab to reduce OCS dose may mitigate the major adverse health consequences associated with OCS use in patients with severe asthma. The OCS-sparing effect of mepolizumab should be considered when selecting treatment options for patients with severe asthma. While treatment guidelines provide recommendations for tapering OCS dose in patients with severe asthma, the potential adverse effects experienced during tapering must be monitored and further guidance on tapering strategies should be developed as a priority.
Supplemental Material
sj-docx-1-tar-10.1177_17534666221107313 – Supplemental material for Oral corticosteroid-sparing effects of mepolizumab in severe eosinophilic asthma: evidence from randomized controlled trials and real-world studies
Supplemental material, sj-docx-1-tar-10.1177_17534666221107313 for Oral corticosteroid-sparing effects of mepolizumab in severe eosinophilic asthma: evidence from randomized controlled trials and real-world studies by Thomas B. Casale, Autumn Burnette, Arnaud Bourdin, Peter Howarth, Beth Hahn, Alexandra Stach-Klysh and Sandhya Khurana in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
Editorial support (in the form of writing assistance, including preparation of the draft manuscript under the direction and guidance of the authors, collating and incorporating authors’ comments for each draft, assembling tables and figures, grammatical editing and referencing), and submission support was provided by Katie Crossland, PhD, at Fishawack Indicia Ltd., UK, part of Fishawack Health, and was funded by GSK. All authors have authorized the submission of this manuscript and approve all statements and declarations.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.