
Abstract
Asthma is a chronic inflammatory condition involving the airways with varying pathophysiological mechanisms, clinical symptoms and outcomes, generally controlled by conventional therapies including inhaled corticosteroids and long-acting β2 agonists. However, these therapies are unable to successfully control symptoms in about 5–10% of severe asthma patients. Atopic asthma, characterized by high immunoglobulin (Ig)E or eosinophilia, represents about 50% of asthmatic patients. Interleukin (IL)-5 is the main cytokine responsible of activation of eosinophils, hence therapeutic strategies have been investigated and developed for clinical use. Biologics targeting IL-5 and its receptor (first mepolizumab and subsequently, reslizumab and benralizumab), have been recently approved and used as add-on therapy for severe eosinophilic asthma resulting in a reduction in the circulating eosinophil count, improvement in lung function and exacerbation reduction in asthma patients. Despite these biologics having been approved for stratified severe asthma patients that remain uncontrolled with high doses of conventional therapy, a number of patients may be eligible for more than one biologic. Presently, the lack of head-to-head studies comparing the biological agents among themselves and with conventional therapy make the choice of optimal therapy for each patient a challenge for clinicians. Moreover, discontinuation of these treatments, implications for efficacy or adverse events, in particular in long-term treatment, and needs for useful biomarkers are still matters of debate. In this review we evaluate to date, the evidence on mepolizumab that seems to demonstrate it is a well-tolerated and efficacious regimen for use in severe eosinophilic asthma, though more studies are still required.
Introduction
Asthma is a life-long chronic inflammatory condition involving the airways with varying pathophysiological mechanisms, clinical symptoms and outcomes, which is generally controlled by therapies including inhaled corticosteroids and long-acting β2 agonists (LABAs). 1 However, about 5–10% of asthma patients exhibit a more severe disease process with poor asthma control, frequent severe exacerbations and accelerated loss of lung function, despite intensive treatment.2,3 This more severe form of asthma is associated with significant morbidity and mortality, and contributes to a large part of asthma-related costs. 4 Severe asthma remains the subject of extensive research to identify clinical, molecular and inflammatory subphenotypes;5–7 nevertheless, there still remains pockets of unmet needs. 7
Atopic asthma represents about 50% of asthmatic patients and probably a higher proportion in patients with severe asthma.8,9 It is thought that an excess of Th2-type lymphocytes and their secreted interleukin (IL)-4, IL-5 and IL-13 cytokines are implicated in atopic asthma. Indeed, these cytokines are responsible for the raised immunoglobulin (Ig)E levels (IL-4 and IL-13), eosinophilia (IL-5), mucus hypersecretion and airway hyper-responsiveness (both probably consequences of IL-13).10,11 However, a subgroup of asthma patients show eosinophilia in the absence of an allergic aetiology to their asthma.10,12 Eosinophilic inflammation is associated with frequent asthma exacerbations and disease severity,13,14 and is sustained by the biological activity of IL-5. Due to the pivotal role of IL-5 in the maturation, proliferation, activation and survival of eosinophils, 15 treatments targeting IL-5 have been investigated and developed for their therapeutic effects on patients with severe asthma. 8 Biologics targeting IL-5, mepolizumab (Nucala®, GlaxoSmithKline, UK) and subsequently reslizumab (CINQAIR®; Teva, Israel), have been approved and incorporated into national and international guidelines as add-on therapy for severe eosinophilic asthma.
In this narrative review we discuss licensed biologics in severe atopic asthma, especially anti-eosinophilic agents, and subsequently emphasize our focus on various studies involving mepolizumab, in terms of its efficacy and tolerability, with the aim of attempting to define its best application in clinical practice. We also discuss its limitations with the gaps in the evidence, such as long-term safety and length of use prior to stopping its use.
Search method
We searched the PubMed and Scopus electronic databases with the following keywords terms: ‘severe asthma’, ‘eosinophilic asthma’, ‘biologics’, ‘anti-IL5’, ‘anti-IL5R’, ‘mepolizumab’ with different combinations, and evaluated clinical studies [clinical studies, controlled clinical trials, multicentre studies and randomized controlled trials (RCTs)], observational studies, meta-analyses and post-hoc analyses. We selected only the studies that we judged relevant to the use of mepolizumab in severe asthma. Reference lists from these studies were also examined to identify significant articles. We searched additional information in abstracts presented at scientific congresses (in the fields of respiratory medicine, immunology and allergy) that were available online. Moreover, further research was done in the ClinicalTrials.gov database to identify ongoing RCTs. In total 17 studies were identified as relevant to the search criteria.
Biologics in clinical practice
The effort of intensive research in severe asthma has been in the development of specific biological agents that have been added to the conventional therapy in some cases. Currently, the anti-IgE agent, omalizumab (Xolair®, Novartis, Switzer-land), and anti-IL-5 agents, mepolizumab and reslizumab, and the anti-IL-5α receptor, benralizumab (FASENRA™, AstraZeneca, UK) are the biologic drugs approved as add-on therapy for severe asthma (the latter is awaiting the addition to guidelines). Several other biologics targeting the Th2 pathway and also the non-Th2 pathway are under evaluation. 7
Biologics approved for asthma are directed to stratify patients with severe asthma that remain uncontrolled despite high-dose controller therapy. The stratification of these patients is based mainly on clinical endpoints including allergy tests, IgE levels and blood eosinophils. However, there are patients who might be eligible for more than one biologic,10,16 making it challenging for clinicians in selecting the best treatment option(s). Current guidelines provided by the Global Initiative for Asthma (GINA) 17 and the National Institute for Health and Care Excellence (NICE) 18 in the United Kingdom (UK), showed some differences. Of note, there is not only a lack of head-to-head studies comparing the biological agents, but also of comparisons between biologics and pharmacological or nonpharmacological treatments. The establishment of Integrated Care Pathways, as structured multidisciplinary care plans, may aid physicians to better stratify asthmatic patients for the most appropriate biologic. 16
Omalizumab was the first biologic approved by the United States (US) Food and Drug Administration (FDA) and by the European Medicines Agency (EMA) 19 for the treatment of children, adolescents and adults with severe atopic asthma. Hence, it is the most investigated biologic with several studies proving its efficacy and tolerability.8,20 Patients with atopic asthma who respond to omalizumab have had varying degrees of improvements in lung function, clinical symptoms and reduced exacerbation rates, though some nonatopic severe asthma patients have also been reported to benefit from it. 21 Omalizumab is administered every 2 or 4 weeks by subcutaneous injection; the dose is calculated based on baseline body weight and serum IgE levels. 8 Patients with IgE higher or lower than the range of 30–700 UI/ml are excluded (dependent on the country) and also individuals who exceed the weight limits of 150 kg. 22 A population pharmacokinetic (popPK) analysis identified weight as the most important covariate. 23 The omalizumab dosing table which based on individual serum IgE level and body weight, ensures that each patient receives a dose of at least 0.016 (mg/kg)/(IU/ml) on a 4-weekly basis. 22 Importantly, there is still no consensus on the duration of omalizumab therapy in responders. 24
Mepolizumab and reslizumab target the IL-5 signalling pathway and are effective in severe eosinophilic asthma patients with or without allergies;10,25 indeed, they have both been shown to result in a marked reduction in blood eosinophil count. 26 Nevertheless, eosinophilia is heterogeneously defined in severe asthma patients. Indeed, the eosinophil cut-off varies from study to study and remains a topic of discussion. 10 Mepolizumab is indicated as an add-on maintenance treatment for patients with severe asthma aged ⩾12 years, and with an eosinophilic phenotype defined by blood eosinophils of ⩾150 cells/µl (within 6 weeks of dosing); or blood eosinophils of ⩾300 cells/µl (within 12 months of dosing) or a sputum eosinophil count ⩾3%; or exhaled nitric oxide concentration ⩾50 ppb.27–30 It is administered at a dose of 100 mg by subcutaneous injection once every 4 weeks, independent of weight. 31
Reslizumab is indicated as add-on maintenance treatment in patients with severe asthma aged ⩾18 years with an eosinophilic phenotype defined as blood eosinophil count of at least 400 cells/µl32–34 (within 3 to 4 weeks of dosing), though in one clinical trial it was administered to patients with a medium blood eosinophil count of 280 cells/µl. 35 The recommended dosage regimen is 3 mg/kg every 4 weeks administered by intravenous (IV) infusion over 20–50 min. 36
Benralizumab also targets the IL-5 pathway binding to the alpha subunit of IL-5 receptor and was approved by the US FDA in November 2017. Treatment with benralizumab depletes eosinophils by antibody-dependent and cell-mediated cytotoxicity. 37 Moreover, it has been shown that benralizumab markedly attenuates or eradicates tissue eosinophilia with associated improvements in clinical manifestations.38,39 The recommended dose of benralizumab for adults (⩾18 years) with severe uncontrolled asthma is 30 mg by subcutaneous injection every 4 weeks for the first three doses, and subsequently every 8 weeks thereafter. The safety and efficacy of benralizumab in children aged 5 to 18 years have not been established.
Targeting IL-5
IL-5 is a glycoprotein that belongs to the cytokine superfamily. It is produced by eosinophils, mast cells, Th2 cells, natural killer cells, group 2 innate lymphoid cells (ILC2) and CD34+ progenitor cells. 40 It is pivotal for the proliferation, maturation, activation, recruitment and survival of eosinophils.25,41,42 Human eosinophils differ in the bone marrow, being under the control of IL-5, IL-3 and the granulocyte-monocyte colony-stimulating factor (GM-CSF) resulting in an activation of the IL-5 receptor. The alpha subunit of this receptor (IL-5Rα) specifically binds IL-5, and is highly expressed on the eosinophil surface but less on basophils. 43 Binding of IL-5 to the receptor complex results in the activation of IL-5 signalling systems, which leads to mobilization of eosinophils and their progenitors in the blood circulation, and to eosinophil activation for increased survival and cytotoxicity.41,44 The infiltration and degranulation of eosinophils at the site of inflammation leads to the release of four cationic proteins: major basic proteins (MBP), eosinophil cationic protein, eosinophil-derived neurotoxin, and eosinophil peroxidase (EPX). These proteins have cytotoxic activity, that contributes to airway tissue damage, mucus hypersecretion, and bronchial hyper-responsiveness. Moreover, eosinophils secrete lipid mediators, including cysteinyl leukotrienes (LTC4, LTD4, and LTE4), platelet activating factor, thromboxane B2 (T × B2), prostaglandin (PG) E1, and PGE2.11,45
Thus, IL-5 is a critical regulator of blood and tissue eosinophilia in severe eosinophilic asthma. Concomitant high blood and sputum eosinophilia correlate with poor asthma control and propensity to asthma exacerbation.7,46 Mepolizumab and reslizumab, indirectly reduce blood eosinophilia by neutralising circulating IL-5, however, they seem less efficacious in eliminating sputum eosinophilia. 47 Importantly, several studies have confirmed clinical improvement in lung function and exacerbation reduction in asthma patients treated with anti-IL5 therapies.8,48
Mepolizumab
Mepolizumab was the first anti-IL-5 monoclonal antibody (mAb) approved as add-on maintenance therapy for the treatment of severe eosinophilic asthma in patients aged ⩾12 years. It is a fully humanized IgG1 kappa mAb that can be administered subcutaneously into the patient’s upper arm, thigh, or abdomen with a fixed dose of 100 mg every 4 weeks. 49 Mepolizumab, by binding free IL-5, prevents its interaction with IL-5Rα expressed on the surface of eosinophils which significantly attenuates eosinophilic differentiation in the bone marrow and the amount of extracellular matrix proteins in the reticular basement membrane of the airway mucosa.50,51 Although the detailed route of elimination for mepolizumab is unknown, it is thought that it is degraded by proteolytic enzymes, that are widely distributed throughout the body.52,53 Following subcutaneous administration, mepolizumab has a mean elimination half-life of 16–22 days. 53 In patients with asthma, mepolizumab has an estimated apparent systemic clearance of 0.28 l/day (70 kg individual).
Early studies using mepolizumab
Initial studies on the development of mepolizumab (Table 1) reported poor efficacy but no safety concerns. The first RCT assessing mepolizumab was conducted by Leckie and collegues. 54 In this study, three groups of eight patients each received a single IV infusion every 4 weeks of placebo, 2.5 mg/kg or 10 mg/kg of mepolizumab for up to 16 weeks. The authors observed no significant improvements in terms of airway hyper-reactivity, peak expiratory flow (PEF), and forced expiratory volume in 1 s (FEV1), though significant reductions in airway and blood eosinophil counts were observed in the 10 mg/kg group after 4 and 16 weeks compared with placebo. 54 Subsequently, in another small study of 24 mild asthma patients treated with 750 mg of mepolizumab or placebo for 8 weeks, although did not achieve improvements in clinical endpoints of FEV1, PEF and airway hyper-reactivity, reported a marked attenuation in blood, airway and bone marrow eosinophils. 55
Early studies of mepolizumab in asthma patients.
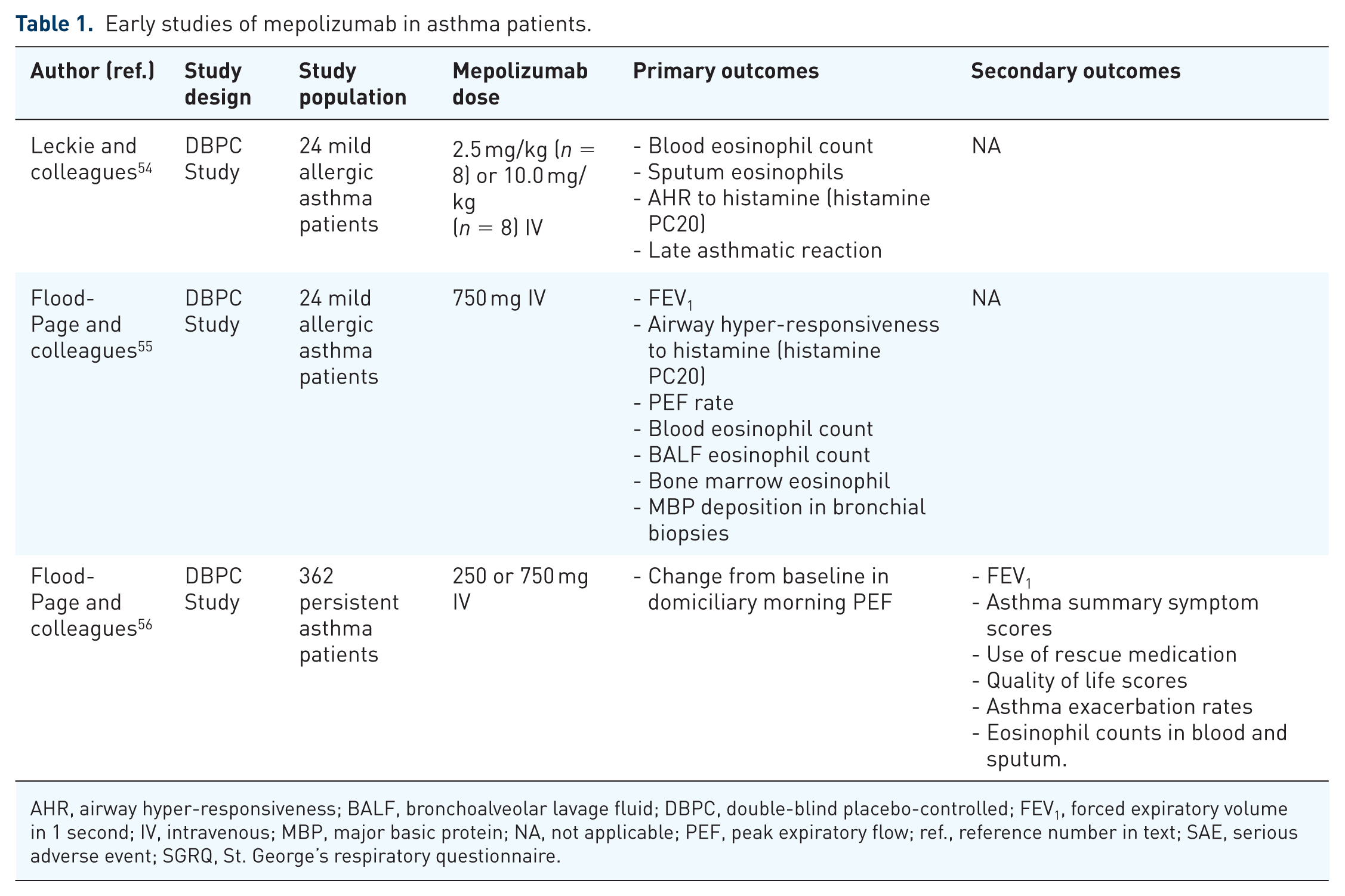
AHR, airway hyper-responsiveness; BALF, bronchoalveolar lavage fluid; DBPC, double-blind placebo-controlled; FEV1, forced expiratory volume in 1 second; IV, intravenous; MBP, major basic protein; NA, not applicable; PEF, peak expiratory flow; ref., reference number in text; SAE, serious adverse event; SGRQ, St. George’s respiratory questionnaire.
Subsequently, a large multicentre RCT in 362 patients experiencing persistent asthma symptoms despite inhaled corticosteroid therapy was conducted in which IV mepolizumab was administered at a dose of 250 or 750 mg every 30 days for 12 weeks. Akin to the smaller prior studies no significant clinical improvements were observed, despite the marked attenuation in blood and airway eosinophilia. 56 These results were probably due to the short period of mepolizumab treatment, the heterogeneity of patients with mild or moderate chronic persistent asthma and the efficacy outcomes assessed, though importantly there were no safety concerns.
Phase II and III studies using mepolizumab
Successively, two RCTs conducted in small groups of carefully selected phenotypes of chronic severe eosinophilic asthma demonstrated that mepolizumab effectively reduced sputum and blood eosinophils and asthma exacerbations (Table 2).57,58 Additionally, in the work of Nair and colleagues patients were observed to be able to significantly attenuate their oral corticosteroid (OCS) therapy with marginal improvements in FEV1 values. Additionally, in the Haldar and colleagues study, 50 weeks of mepolizumab treatment not only significantly reduced airway wall thickness and total wall area as measured by computed tomography (CT) scanning, but also improvements in asthma quality of life questionnaire (AQLQ) scores were noted in favour of mepolizumab-treated patients. 58
Phase II and III mepolizumab studies in severe eosinophilic asthma.
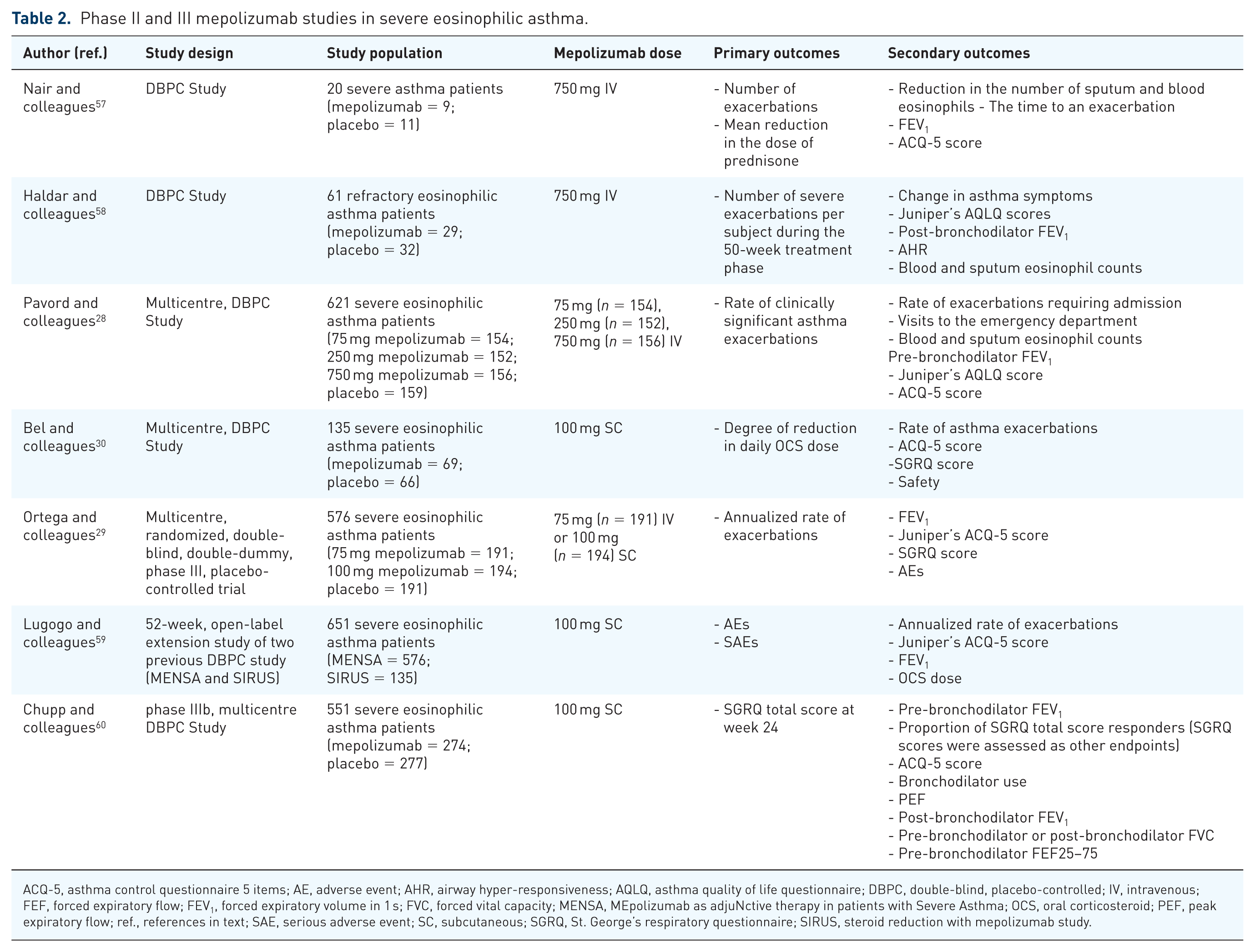
ACQ-5, asthma control questionnaire 5 items; AE, adverse event; AHR, airway hyper-responsiveness; AQLQ, asthma quality of life questionnaire; DBPC, double-blind, placebo-controlled; IV, intravenous; FEF, forced expiratory flow; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; MENSA, MEpolizumab as adjuNctive therapy in patients with Severe Asthma; OCS, oral corticosteroid; PEF, peak expiratory flow; ref., references in text; SAE, serious adverse event; SC, subcutaneous; SGRQ, St. George’s respiratory questionnaire; SIRUS, steroid reduction with mepolizumab study.
Further consistent evidence on the therapeutic potential of mepolizumab was gained from the large, multicentre (81 centres in 13 countries), phase IIb/III DREAM (Dose Ranging Efficacy And safety with Mepolizumab) trial performed by Pavord and colleagues. In this study, 621 severe eosinophilic asthma patients aged 12–74 years, were treated with one of three different doses of IV mepolizumab, 75, 250, and 750 mg, or matched placebo every 4 weeks for 52 weeks (13 infusions). The 75 mg IV dose proved to be the best dose–response profile with decreased blood and sputum eosinophil profile counts and annualized asthma exacerbation rate. 28
In 2014, another two RCTs showed the efficacy of mepolizumab therapy in patients with severe eosinophilic asthma. SIRIUS (SteroId ReductIon with mepolizUmab Study) 30 enrolled 135 patients (age 16–74 years) with severe eosinophilia, requiring a daily OCS therapy as maintenance treatment for at least 6 months. The patients were randomized to receive 100 mg mepolizumab subcutaneously (SC) or matched placebo. When compared with placebo, the mepolizumab-treated group showed a 50% reduction in OCS dosage compared with the placebo group (p < 0.007), a decrease in exacerbation rates and improved asthma symptoms as assessed by the asthma control questionnaire 5 (ACQ-5). In the larger MENSA (MEpolizumab as adjuNctive therapy in patients with Severe Asthma) trial by Ortega and colleagues, 29 576 patients (aged ⩾12 years) with severe eosinophilic asthma were randomized to receive 75 mg IV mepolizumab, 100 mg SC mepolizumab, or matched placebo. Both routes of administration reduced the exacerbation rate (47% in the IV group and 53% in the SC group), and emergency department access (32% in the IV group and 61% in the SC group) compared with placebo. Moreover, significant improvement in quality of life (QoL) and a marginal increase in FEV1 were observed in favour of both mepolizumab doses. A progressive decrease in blood eosinophil levels was also noted from week 4 with the maximal reduction at week 12. Additionally, both the SIRUS and MENSA trials showed good safety and tolerability profiles with headache and nasopharyngitis being reported as common adverse events29,30 and low proportions of injection-site reactions were observed during MENSA study. 29
The evidence for the long-term efficacy and safety of mepolizumab was shown in the COSMOS study, an open-label, phase IIIb extension trial, where 651 patients who had previously completed either SIRIUS or MENSA studies were enrolled for a further 52 weeks of mepolizumab therapy (SC 100 mg every 4 weeks). This study showed the durable clinical improvements, including significant reduction of OCS use and annualized exacerbation rates. Furthermore, low rates of both adverse events (AEs) and serious AEs (SAEs), with no fatalities, were reported. 59
More recently, in the phase IIIb MUSCA study, a double-blind, placebo-controlled trial, examined the effect on health-related QoL in 551 severe eosinophilic asthma patients (aged ⩾12 years) over 24 weeks treated with mepolizumab. Compared with placebo, mepolizumab administration resulted in significant improvements in health-related QoL as assessed using the St. George’s respiratory questionnaire (SGRQ) as the primary endpoint, and ACQ-5 with a safety profile similar to placebo over the study period. These primary outcomes were associated with marked improvements in lung function parameters and asthma exacerbation rates in the favour of mepolizumab. 60
Meta-analyses and post-hoc analyses
A number of post-hoc and meta-analyses (Table 3) have confirmed the efficacy and safety of mepolizumab in severe eosinophilic asthma.61–64 Post-hoc analysis of data from the DREAM and MENSA studies showed a reduction of 47% in the mean exacerbation rate in patients with severe eosinophilic asthma treated with mepolizumab compared with placebo [rate ratio (RR) 0.53, 95% confidence interval (CI) 0.44–0.62; p < 0.0001]. Moreover, the percentage exacerbation reduction with mepolizumab versus placebo increased progressively from 52% in patients with a baseline blood eosinophil count of at least 150 cells/μl to 70% in patients with increasing basal blood eosinophils counts (⩾500 cells/μl). 61
Post-hoc and meta-analyses of mepolizumab in severe eosinophilic asthma.

ACQ, asthma control questionnaire; ACQ-5, asthma control questionnaire 5 items; AE, adverse event; AQLQ, asthma quality of life questionnaire; DBPC, double-blind placebo-controlled; DREAM, Dose Ranging Efficacy And safety with Mepolizumab in severe asthma; FEV1, forced expiratory volume in 1 s; HRQoL, health-related quality of life; IgE, immunoglobulin E; MENSA, MEpolizumab as adjuNctive therapy in patients with Severe Asthma; NA, not applicable; OCS, oral corticosteroid; PEF, peak expiratory flow; ref., references in text; SAE, serious adverse event; SC, subcutaneous; SGRQ, St. George’s respiratory questionnaire; SIRUS, steroid reduction with mepolizumab study; IV, intravenous.
In a recent meta-analysis by Yancey and colleagues, 63 the rate of exacerbations requiring hospitalization and hospitalization/emergency room visit were evaluated in 1388 patients with severe eosinophilic asthma treated with mepolizumab or placebo in addition to standard care for at least 24 weeks. Reduced exacerbations requiring hospitalization (RR, 0.49; 95% CI, 0.30–0.80; p < 0.004) and hospitalization/emergency room visit (RR, 0.49; 95% CI, 0.33–0.73; p < 0.001) rates were observed in patients with severe eosinophilic asthma treated with mepolizumab compared with placebo. Also, mepolizumab treatment reduced the number of patients with one or more exacerbations requiring hospitalization or emergency room visits each year. Additionally, two Cochrane systematic reviews have evaluated the efficacy of mepolizumab treatment compared with placebo for patients with severe eosinophilic asthma. Data analysis indicated that mepolizumab improves the QoL and reduces the number of exacerbations with a good safety profile.10,66
In a recent post-hoc analysis, Magnan and colleagues assessed the effects of mepolizumab in 711 patients from the MENSA and SIRIUS studies previously treated with the anti-IgE monoclonal antibody omalizumab (576 from MENSA and 135 from SIRIUS). 65 Patients included were those who had been on omalizumab but was discontinued for at least 130 days before participation to the two trials. A total of 75 (10%) and 45 (5%) patients had received omalizumab for a median duration of 12 months and 8 months respectively; and 104 (14.6%) had discontinued omalizumab treatment due to the lack of efficacy. The patients were characterized by a longer duration of asthma, greater level of OCS dosage for maintenance of asthma, lower FEV1, worse ACQ-5 and SGRQ scores, higher IgE and eosinophils levels, and a higher incidence of asthma exacerbation in the previous year compared with patients without prior omalizumab treatment, highlighting the severity of their asthma. 65 In patients pretreated with omalizumab from MENSA the rate of exacerbation was reduced by 57% compared with placebo, whereas patients without prior omalizumab treatment had a reduction of 47%. 65 In the SIRIUS study OCS reduction was similar between the two groups (with and without prior omalizumab treatment), whereas the proportion of patients with no decrease in OCS use, lack of asthma control, or early withdrawal was higher in omalizumab pretreated group. 65 Nevertheless, the efficacy in reducing the OCS use and the exacerbation rate compared with placebo group was similar with and without omalizumab pretreatment. Importantly, the safety profile for patients with and without prior omalizumab treatment was similar. 65
Discussion
Like with the use of omalizumab, the discontinuation of mepolizumab treatment is still a matter of debate. Notably, some studies demonstrated a reversal of the positive benefits on exacerbations and airway eosinophilia within 6 months of mepolizumab withdrawal.58,67 There is an ongoing multicentre, randomized, double-blind, placebo-controlled, parallel group study comparing cessation versus continuation of long-term mepolizumab treatment in patients with severe eosinophilic asthma (ClinicalTrials.gov Identifier: NCT02555371).
Despite the efficacy of mepolizumab treatment in a large number of severe eosinophilic asthma patients, there remain patients, with an indication for anti-IL5 therapy, who did not respond to mepolizumab therapy. 68 In a retrospective analysis of clinical efficacy of IL-5 antibody therapy a quarter of patients were classified as ‘nonresponders’, though no baseline characteristics (sex, body mass index, smoking history, allergies, baseline level of eosinophils) were identified as predictors of mepolizumab response. Moreover, five nonresponders to mepolizumab treatment were previously treated with omalizumab without treatment benefits. 68 It seems that in mepolizumab, nonresponders switching to IV reslizumab adapted to weight may be beneficial.69,70 The genetic characteristics of these patients may explain the lack in response to mepolizumab.68,71
At present, as mepolizumab (and likewise reslizumab and benralizumab) has only been approved for routine use in severe eosinophilic asthma recently, there are no real-life studies on its use.
With the availability of three anti-IL-5 molecules, a careful evaluation of the optimal anti-IL-5 agent is essential in the future; this is not only from a clinical perspective, but also to keep in mind that the circulating eosinophil activity is not solely in the lungs, but is part of the immune surveillance system. Eosinophils perform a protective action, particularly in parasitic infections, especially from helminths. Importantly, although all three of these anti-IL-5 agents markedly reduced blood eosinophils, benralizumab results in their near complete depletion from the peripheral circulation, whereas in the case of the other two, a small number still persist. 10 The complete or near elimination of eosinophils may lead to considerable side effects over time, given that these cells can induce a protective immune response against helminths, viral and bacterial pathogens and sometimes to cancer cells. 72
Hence, the implications for efficacy or AEs of these anti-IL-5 biologics are still unclear, and need further investigation.
Conclusion
The pharmacological arsenal available to control asthma symptoms and to improve the QoL of asthma patients is constantly growing. It is paramount to intricately define the criteria for selecting the right patient for the correct therapy to be administered to assure the optimal risk–benefit ratio.
Future research is needed to assess the long-term efficacy, the optimal duration and the risk after mepolizumab withdrawal. Additionally, more work is needed to establish biomarkers that enable clinicians to identify the patients who would benefit from its use and the optimal blood eosinophil threshold. With the approval of three anti-IL-5 molecules, it would be prudent to evaluate which one of the three would be the best one in terms of efficacy and safety, and in which circumstances one would be superior to the others; hence conducting head-to-head studies are essential. From the current evidence in the literature to date, mepolizumab seems to be an efficacious and well-tolerated regimen for use in severe eosinophilic asthma, although more studies are still required.
Footnotes
Acknowledgements
Rosalia Emma and Jaymin B. Morjaria contributed equally to the writing of this manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.