
Abstract
Background:
Coronavirus disease 2019 (COVID-19) has spread globally, and many patients with severe cases have received oxygen therapy through a high-flow nasal cannula (HFNC).
Objectives:
We assessed the efficacy of HFNC for treating patients with COVID-19 and risk factors for HFNC failure.
Methods:
We searched PubMed, Embase, and the Cochrane Central Register of randomized controlled trials (RCTs) and observational studies of HFNC in patients with COVID-19 published in English from January 1st, 2020 to August 15th, 2021. The primary aim was to assess intubation, mortality, and failure rates in COVID-19 patients supported by HFNC. Secondary aims were to compare HFNC success and failure groups and to describe the risk factors for HFNC failure.
Results:
A total of 25 studies fulfilled selection criteria and included 2851 patients. The intubation, mortality, and failure rates were 0.44 (95% confidence interval (CI): 0.38–0.51, I2 = 84%), 0.23 (95% CI: 0.19–0.29, I2 = 88%), and 0.47 (95% CI: 0.42–0.51, I2 = 56%), respectively. Compared to the success group, age, body mass index (BMI), Sequential Organ Failure Assessment (SOFA) score, Acute Physiology and Chronic Health Evaluation (APACHE) II score, D-dimer, lactate, heart rate, and respiratory rate were higher and PaO2, PaO2/FiO2, ROX index (the ratio of SpO2/FiO2 to respiratory rate), ROX index after the initiation of HFNC, and duration of HFNC were lower in the failure group (all Ps < 0.05). There were also more smokers and more comorbidities in the failure group (all Ps < 0.05). Pooled odds ratios (ORs) revealed that older age (OR: 1.04, 95% CI: 1.01–1.07, P = 0.02, I2 = 88%), a higher white blood cell (WBC) count (OR: 1.06, 95% CI: 1.01–1.12, P = 0.02, I2 = 0%), a higher heart rate (OR: 1.42, 95% CI: 1.15–1.76, P < 0.01, I2 = 0%), and a lower ROX index(OR: 0.61, 95% CI: 0.39–0.95, P = 0.03, I2 = 93%) after the initiation of HFNC were all significant risk factors for HFNC failure.
Conclusions:
HFNC is an effective way of providing respiratory support in the treatment of COVID-19 patients. Older age, a higher WBC count, a higher heart rate, and a lower ROX index after the initiation of HFNC are associated with an increased risk of HFNC failure.
Introduction
The SARS-CoV-2 virus, which is responsible for COVID-19, spread rapidly worldwide and created a pandemic in 2019. 1 The high infectivity and exponential spread of SARS-CoV-2, coupled with its potential to develop rapidly into acute respiratory distress syndrome, led to high mortality.2–4 About 15–30% of COVID-19 patients experienced hypoxemia and progress to acute respiratory distress syndrome. 3 Noninvasive respiratory support, including the use of a high-flow nasal cannula (HFNC) and noninvasive ventilation (NIV), is now widely given to these patients.
HFNC is an oxygen supply system capable of delivering up to 100% humidified and heated oxygen at a flow rate of up to 60–100 liters per minute.5,6 It is useful for treating hypoxemic respiratory failure. It may lead to less treatment failure compared to the use of conventional oxygen therapy (COT), 7 and it is better tolerated than NIV. 8
Previous studies, mainly retrospective and with small sample sizes, suggest potential benefits associated with the use of HFNC in treating respiratory failure due to COVID-19.9–11 However, there is a lack of large-sample research on the effectiveness of HFNC for treating COVID-19. Moreover, despite their advantages, the failure rate of noninvasive treatments in patients with COVID-19 is high, and there is a concern that poor patient selection or prolonged trials of HFNC may result in worse clinical outcomes.12,13 Therefore, the main aim of this study was to summarize the characteristics of patients using HFNC and to assess its efficacy. We also compare the characteristics of patients in HFNC success and failure groups and describe risk factors for HFNC failure.
Methods
Search strategy
We searched PubMed, Embase, and the Cochrane Central Register of RCTs and observational studies of HFNC in patients with COVID-19 published in English from January 1st, 2020 to August 15th, 2021. We searched for ( ‘HFNC’ or ‘high-flow nasal cannula’ or ‘high-flow oxygen therapy’ or ‘high-flow nasal oxygen’) and ( ‘COVID-19’ or ‘coronavirus disease 2019’). In addition, we carefully evaluated the reference lists of all primary studies and review articles for other relevant studies.
Study selection
Our inclusion criteria were as follows: i) cohort study, case-control study, or RCT; ii) the inclusion of patients with laboratory-confirmed COVID-19; iii) HFNC used to relieve hypoxemia prior to (invasive or noninvasive) mechanical ventilation; and iv) at least one of the following outcomes: mortality rate, intubation rate, escalation rate (to NIV or invasive mechanical ventilation), and characteristics of patients successfully weaned from HFNC and those not successfully weaned.
HFNC failure was defined as the need for NIV or invasive mechanical ventilation and/or death while on HFNC support. Demographic, clinical, laboratory, management, and outcome data were obtained from medical records.
Exclusion criteria were as follows: i) patients did not meet screening criteria; ii) the study focused on pediatric patients; iii) non-English study, commentary, review, full text not available, and/or duplicate publications from a single study; iv) data could not be extracted by statistical methods or non-targeted outcomes; and v) the study reused patient data.
The ultimate decision to include a study was made following a full-text review of the article by two investigators focusing on publication date, study type, study design, and outcomes. Discrepancies were resolved by consensus.
Quality control
The Newcastle-Ottawa Scale was used to assess the quality of the eligible studies. Each cohort study was assessed on seven items regarding patient selection, trial design, and measurement of outcomes; each case-control study was assessed on seven other items regarding patient selection, comparability, and exposure. One star was awarded for each quality criterion the study satisfied; the highest quality studies were awarded seven stars. A study was considered of good, normal, and poor quality if it was awarded 6 or 7, 3–5, and 0–2 stars, respectively.
Statistical analysis
Data and basic information from each study were independently extracted and cross-checked by two investigators for further analysis. The dates and hospitals of all included studies were checked in detail to avoid duplication. R (version 4.0.2; Comprehensive R Archive Network, 2020) and Review Manager (version 5.3; Nordic Cochrane Center, Cochrane Collaboration, 2014) were used to pool available data.
Baseline data for HFNC success and failure groups were compared with Z tests. P < 0.05 was taken to indicate a significant difference. Outcomes regarding intubation, failure, and mortality rates were measured as proportions with corresponding 95% confidence intervals (CIs) and then pooled and presented in forest plots. Random-effects models were used in cases of obvious heterogeneity. To investigate the risk factors for HFNC failure, we used DerSimonian-Laird random-effects models to pool odds ratios (ORs) and their corresponding 95% CIs. Definitions of the same risk factor should have been similar across all included studies, and the results of multivariate analysis were preferentially adopted. Because of the short follow-up period (usually only 1 month), hazard ratios expressed similar meaning to ORs and were therefore pooled together in this meta-analysis.
In each analysis, the heterogeneity between studies was measured with the I2 statistical index (range: 0–100%), with 25%, 50%, and 75% corresponding to low, moderate, and high heterogeneity, respectively. Random-effects models were used when obvious heterogeneity existed. Funnel plots, Egger’s test, and Begg’s test were used to evaluate publication bias. Qualitative data were compared with Z tests. P < 0.05 was considered to indicate a significant difference.
Results
Search results
As depicted in Figure 1, a total of 1429 records were identified from the search. After excluding duplicates and evaluating the full texts of articles, we identified 25 eligible studies (1 RCT, 12 case-control studies, and 12 cohort studies).14–38 The search and screening process is described in Figure 1. The main characteristics of the articles included in the meta-analysis are shown in Tables 1, 2, 3 and 4.

Selection of studies for the meta-analysis (PRISMA).
Characteristics of the studies.

Note: COVID-19: novel coronavirus 19 disease; ICU: Intensive Care Unit; AHRF: acute hypoxemic respiratory failure.
ARDS, acute respiratory distress syndrome; CPAP, continuous positive airway pressure; HFNC, high flow nasal cannula; MD, missing data; NIV, non-invasive ventilation.
Characteristics of the studies.
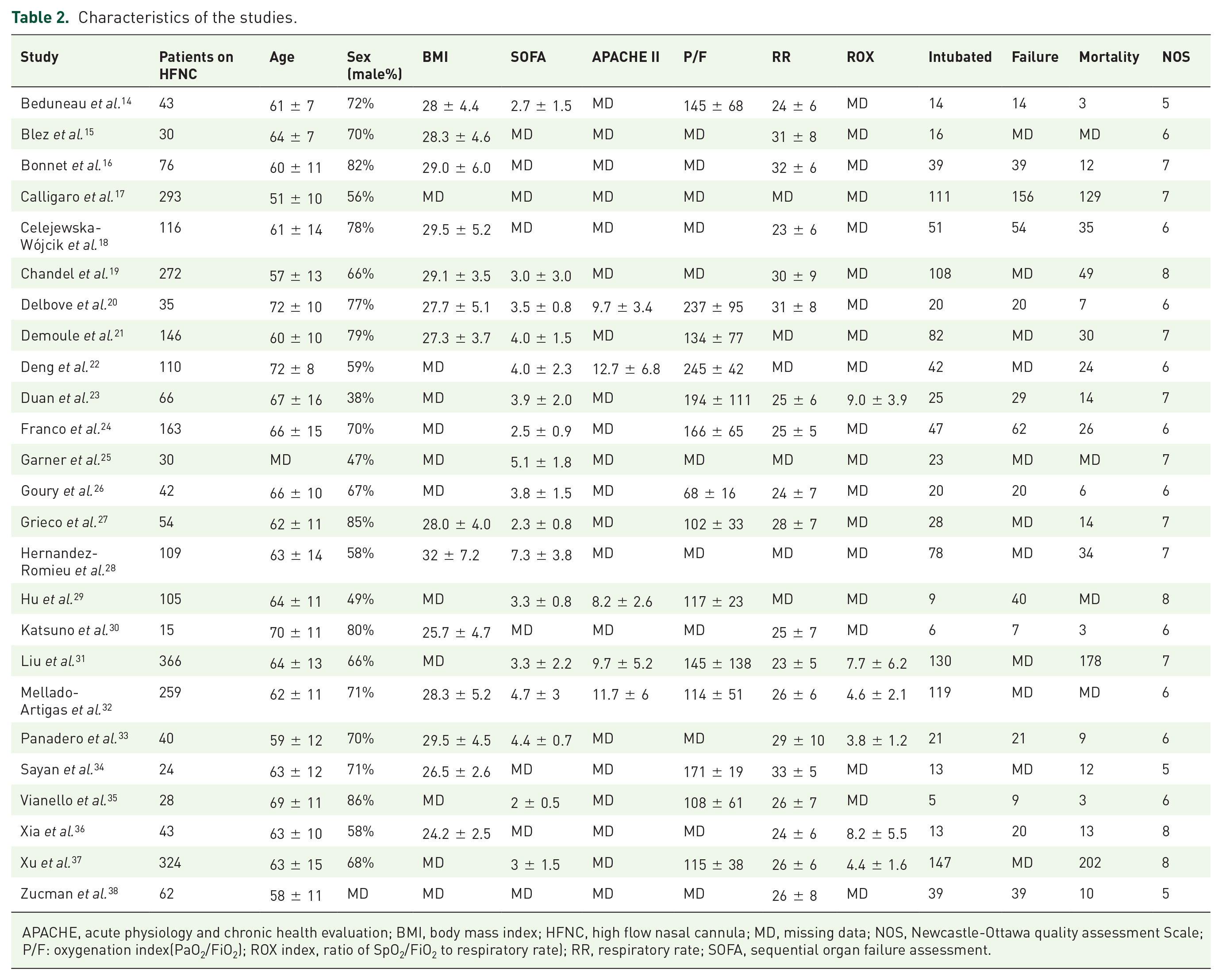
APACHE, acute physiology and chronic health evaluation; BMI, body mass index; HFNC, high flow nasal cannula; MD, missing data; NOS, Newcastle-Ottawa quality assessment Scale; P/F: oxygenation index(PaO2/FiO2); ROX index, ratio of SpO2/FiO2 to respiratory rate); RR, respiratory rate; SOFA, sequential organ failure assessment.
Characteristics of the studies.

Note: (1) Age (2) Sex (3) BMI (Body Mass Index) (4) Obesity (BMI > 30) (5) SOFA (Sequential Organ Failure Assessment) (6) APACHE II (Acute Physiology and Chronic Health Evaluation II) (7) Glasgow score (8) Smoke (9) Hypertension (10) CoroMDry artery disease (11) Diabetes (12) Chronic pulmoMDry disease (13) Chronic kidney disease (14) MaligMDncy (15) White blood cell (16) Lymphocyte (17) C-reactive protein (18) D-dimer (19) Lactate (20) Heart rate (21) Respiratory rate (22) PaO2 (23) PaCO2 (24) SpO2 (25) PaO2/FiO2 (26) ROX index (defined as the ratio of SpO2/FiO2 to respiratory rate) (27) ROX after HFNC initiation (28) Length of HFNC use (29) Length of stay (30) Intubation (31) Mortality (32) HFNC failure.
Characteristics of the studies.
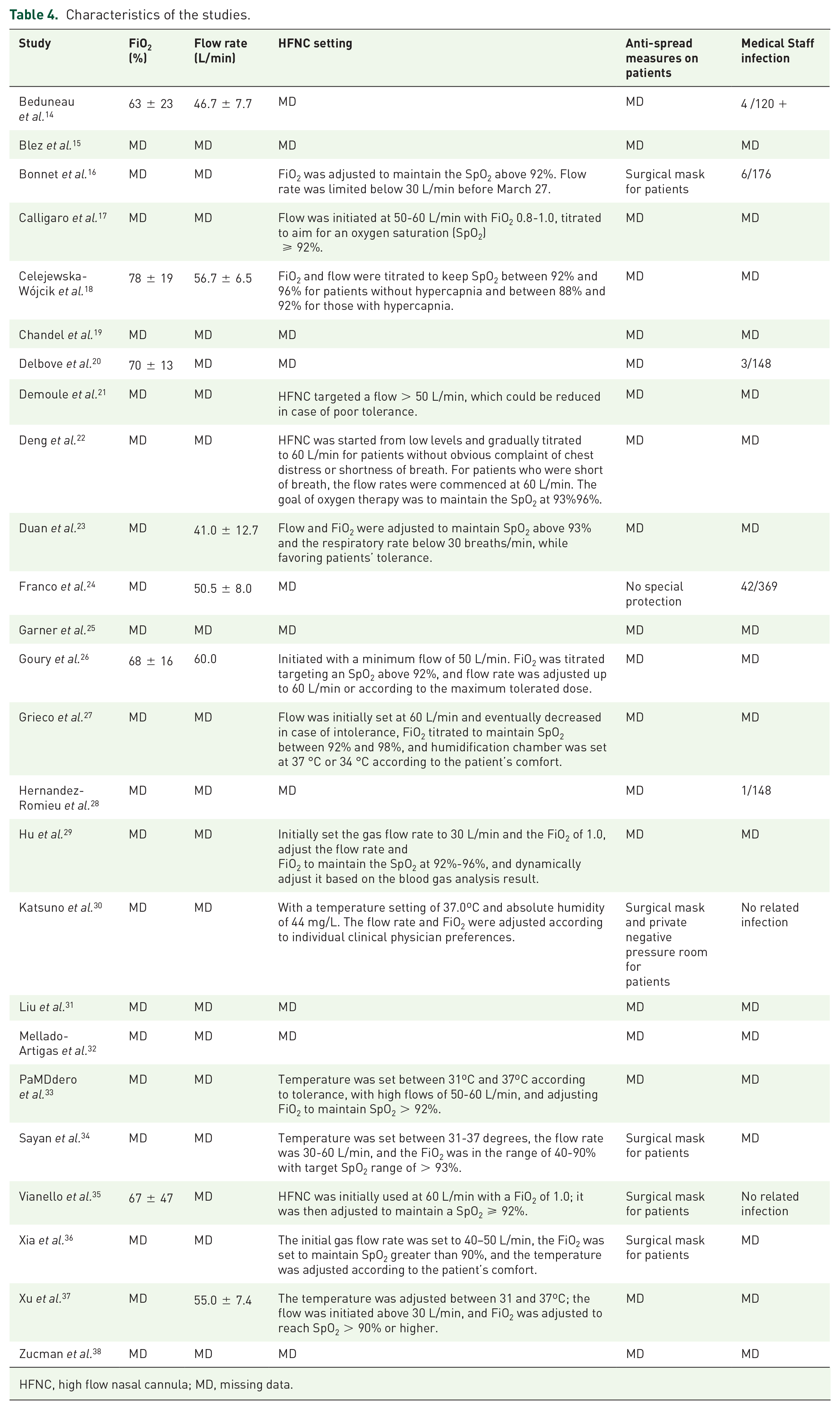
HFNC, high flow nasal cannula; MD, missing data.
Literature quality and bias assessment
Because only one RCT was included in the meta-analysis, and the remainder of the included studies were cohort and case-control studies, the quality of the literature was assessed with the Newcastle-Ottawa Scale. The results are shown in Supplemental Figure S1. All articles were of medium quality (⩾3 stars) or higher; eight articles were considered high-quality studies (⩾6 stars). Symmetry funnel plots of intubation and failure rates indicated no obvious publication bias, a finding corroborated by Egger’s test (P = 0.79 >|t| and P = 0.59 >|t|), whereas plots of the mortality rate did indicate bias (Figure 2).

Funnel plots of the proportion versus the standard error of intubation (a), mortality (b), and failure rates(
Clinical outcomes
A total of 2851 patients from 25 studies, all COVID-19 patients supported by HFNC, were ultimately included in the study. Baseline characteristics and clinical outcomes for the patients are summarized in Table 2. The mean age was 61 ± 13 years, 1603 patients (66.2%) were male, and the mean body mass index (BMI) was 28.9 ± 5.2. The mean Sequential Organ Failure Assessment (SOFA), APACHE II, and Glasgow Coma Scale scores were 3.7 ± 2.5, 11.1 ± 5.7, and 15.0 ± 0.1, respectively. Many patients had underlying comorbidities, including hypertension (1028, 46.3%), coronary artery disease (83, 9.2%), diabetes (655, 29.5%), chronic pulmonary disease (1589, 10.1%), chronic kidney disease (99, 9.4%), and malignancy (55, 4.6%). Inflammatory marker profiles, D-dimer, and lactate are also presented in Table 2. The mean heart rate, respiratory rate, PaO2, PaCO2, SpO2, PaO2/FiO2, and the ROX index at hospital admission were 87.2 ± 16.9, 26.9 ± 7.2, 75.5 ± 23.1, 35.0 ± 7.5, 90.6 ± 6.4, 141.5 ± 70.3, and 5.1 ± 2.9, respectively.
As shown in Table 5, a total of 1076 out of 2482 patients on HFNC from 24 studies14–30,32–38 ultimately received invasive mechanical ventilation, for a pooled intubation rate of 0.44 (95% CI: 0.38–0.51, I2 = 84%; Figure 3(a)). A total of 586 out of 2055 patients on HFNC from 20 studies14,16–24,26–28,30,33–38 ultimately died, for a mortality rate of 0.23 (95% CI: 0.19–0.29, I2 = 88%; Figure 3(b)). A total of 529 out of 1124 patients from 14 studies14,16–18,20,23,24,26,29,30,33,35,36,38 experienced HFNC failure (escalation to NIV or intubation and/or death), for a failure rate of 0.47 (95% CI: 0.42–0.51, I2 = 56%; Figure 3(c)). When reported, the ROX index after the initiation of HFNC was 5.0 ± 2.4, the duration of HFNC was 4.9 ± 5.0 days, and the length of the hospital stay was 19.6 ± 13.6 days.
Main demographic variables, clinical characteristic, and outcomes of the enrolled patients.
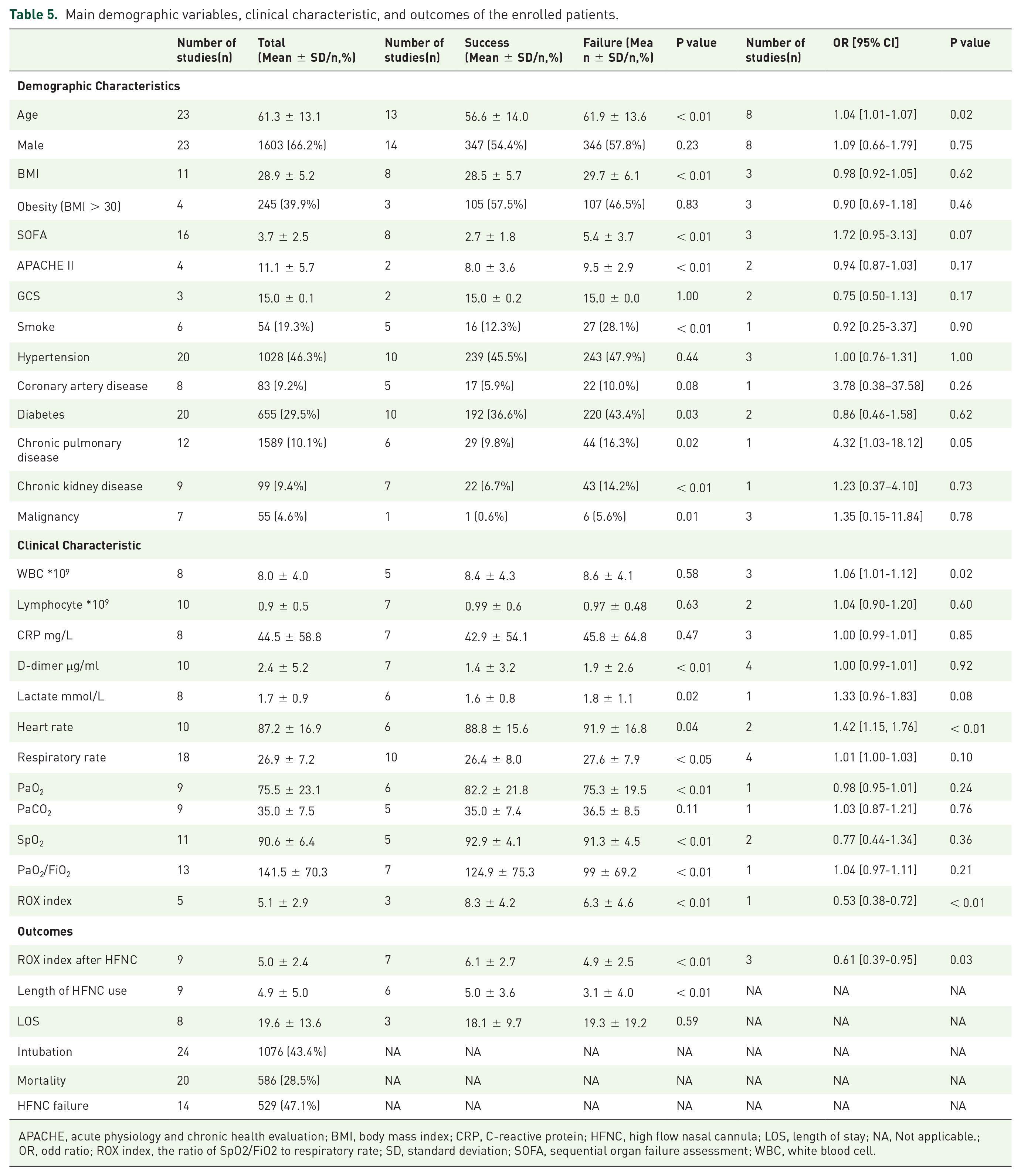
APACHE, acute physiology and chronic health evaluation; BMI, body mass index; CRP, C-reactive protein; HFNC, high flow nasal cannula; LOS, length of stay; NA, Not applicable.; OR, odd ratio; ROX index, the ratio of SpO2/FiO2 to respiratory rate; SD, standard deviation; SOFA, sequential organ failure assessment; WBC, white blood cell.

Intubation (
Differences in demographics and clinical characteristics between patients with a successful outcome on HFNC (success group) and those who experienced HFNC failure (failure group) are summarized in Table 5. When reported, compared to the HFNC success group, patients in the HFNC failure group had higher age, BMI, SOFA scores, APACHE II scores, D-dimer, lactate, heart rate, and respiratory rate and lower PaO2, SpO2, PaO2/FiO2, and duration of HFNC (all Ps < 0.05). Numbers of smokers and patients with diabetes, chronic pulmonary disease, chronic kidney disease, and malignancy were also higher in the failure group (all Ps < 0.05). The ROX index at admission and the ROX index after the initiation of HFNC also differed significantly between patients in the success and failure groups: 8.3 ± 4.2 versus 6.3 ± 4.6 (P < 0.01) and 6.1 ± 2.7 versus 4.9 ± 2.5 (P < 0.01), respectively. We did not find any differences in the number of male patients, the number of obese patients (BMI > 30), certain underlying comorbidities (hypertension and coronary artery disease), inflammatory marker profiles at admission, or PaCO2 at admission between the success and failure groups (all Ps > 0.05). Detailed data and corresponding P values are shown in Table 5.
Several risk factors for HFNC failure were weighed in some studies, and pooled results are shown in Table 5 and Figure 4 . The pooled ORs revealed that older age (OR: 1.04, 95% CI: 1.01–1.07, P = 0.02, I2 = 88%), a higher white blood cell (WBC) count (OR: 1.06, 95% CI: 1.01–1.12, P = 0.02, I2 = 0%), and a higher heart rate (OR: 1.42, 95% CI: 1.15–1.76, P < 0.01, I2 = 0%) were all significant risk factors for HFNC failure. In contrast, a higher ROX index after the initiation of HFNC (OR: 0.61, 95% CI: 0.39–0.95, P = 0.03, I2 = 93%) indicated a lower chance of HFNC failure.
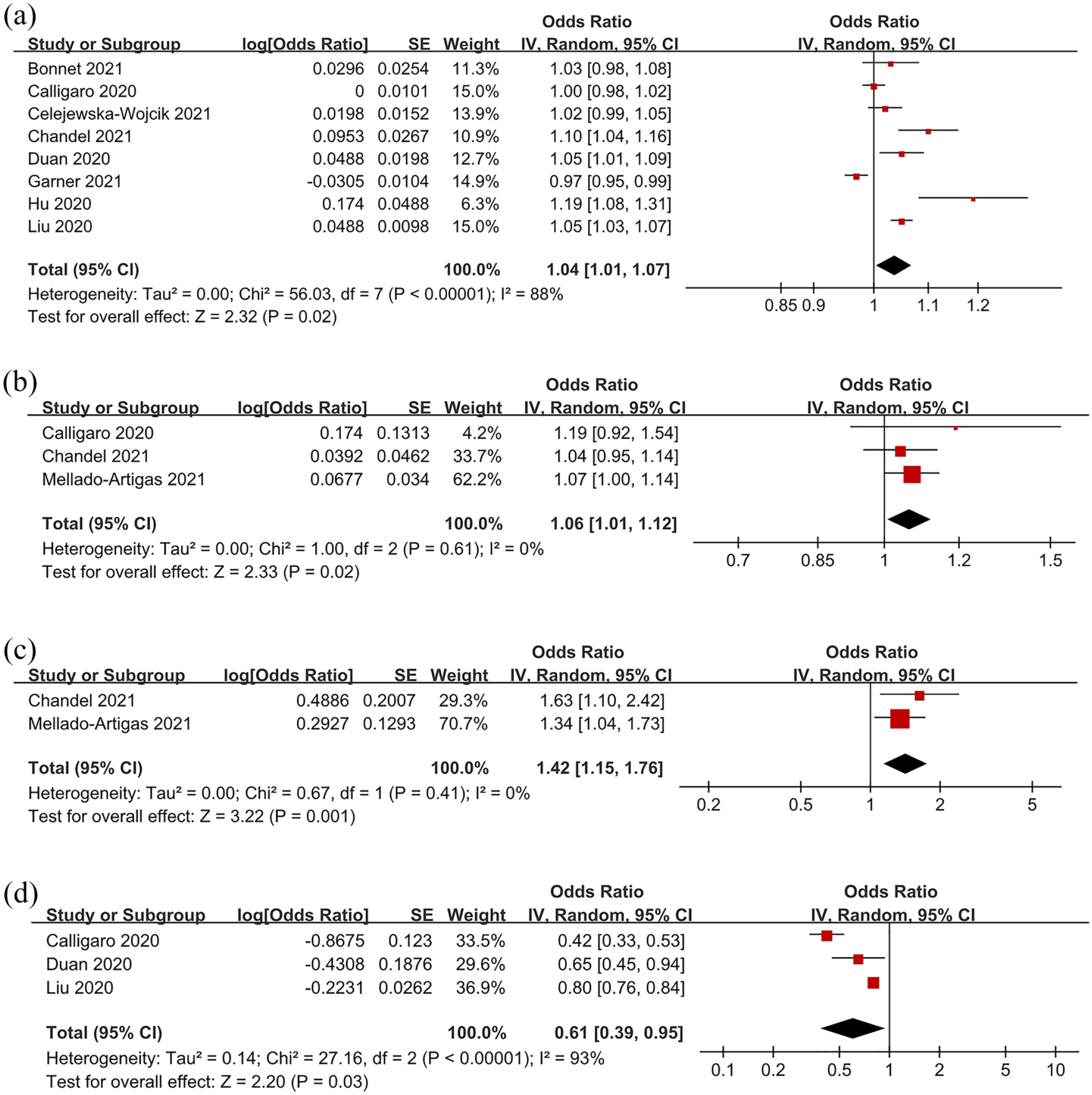
Forest plots of significant risk and protective factors for HFNC failure: age (
Discussion
In this meta-analysis based on 2851 patients from 25 studies hospitalized for COVID-19, intubation, mortality, and failure rates were 0.44, 0.23, and 0.47, respectively. Compared to the HFNC success group, patients in the HFNC failure group were older; had higher BMI, SOFA and APACHE II scores, CRP, D-dimer, RR, HR, and lactate; and had lower PaO2, SpO2, PaO2/FiO2, baseline ROX index, and ROX index after the initiation of HFNC. There were also more smokers and more comorbidities in the failure group. Pooled ORs showed that older age, a higher WBC count, a higher heart rate, and a lower ROX index after the initiation of HFNC were associated with an increased risk of HFNC failure.
HFNC has several positive physiological and clinical advantages in treating acute respiratory failure. 39 A meta-analysis of nine RCTs of acute hypoxemic respiratory failure in the pre-COVID-19 era found that HFNC resulted in lower intubation rates without affecting survival. 40 Preliminary data, mainly from case reports and small case series, also point to its potential utility in treating COVID-19.9–11 In this study, the failure rate of HFNC in COVID-19 patients was 0.47, and intubation and mortality rates were 0.44 and 0.23, respectively. In one of the largest published studies on the effectiveness of NIV for treating COVID-19, failure and mortality rates were 37.6% and 25%, respectively. 41 One meta-analysis found that 26% of COVID-19 patients experienced NIV failure and required intubation, with intra-hospital mortality of 72%. 42 However, compared to NIV and COT, the effects of HFNC on intubation and mortality are not clear. As few studies in our meta-analysis compared HFNC to COT16,34 or NIV,24,27 we did not compare intubation and mortality rates between HFNC and COT or NIV in patients with COVID-19. Whether HFNC can benefit COVID-19 patients clinically must be studied further.
The use of HFNC to treat COVID-19 is very controversial. A literature review found that HFNC can reduce the need for intubation in patients with COVID-19 and decrease the length of stay in the intensive care unit and complications related to mechanical ventilation. 43 Some guidelines recommend HFNC over COT or NIV to treat hypoxia associated with COVID-19.44–46 World Health Organization suggest a short trial (about 1 h) of HFNC may be used in selected patients with COVID-19 and mild ARDS, and patient should be in a monitored setting and cared for in case the patient acutely deteriorates or does not improve after a the trial. 47 Besides, there is insufficient evidence to classify HFNC as an aerosol-generating procedure that is associated with transmission of COVID-19. 47 In the studies included in this meta-analysis and in other studies, some measures such as negative-pressure rooms, high-energy particulate accumulator filters, adequate personal protective equipment, and surgical masks may be sufficient to protect staff. 13,30,35,48
Patients at greater risk of HFNC failure are older, have a higher BMI, have higher SOFA and APACHE II scores, have more severe hypoxia, are more likely to be smokers, and have more comorbidities than those who experience successful HFNC. SARS-CoV-2 is capable of infecting people of all ages, but older people and people with preexisting medical conditions are predisposed to infection and severe forms of COVID-19.49,50 The list of comorbidities includes obesity, diabetes, hypertension, lung, liver, and kidney disease, compromised immunity (for cancer patients on chemotherapy, transplant recipients), smoking, and chronic use of steroids. 51 Higher SOFA and APACHE II scores have also been associated with increased mortality in critically ill patients with COVID-19. 52 Careful continuous monitoring of hypoxemic COVID-19 patients treated with HFNC is needed to detect early signs of failure and avoid delays in intubation. The World Health Organization has also pointed out that the oxygenation status of COVID-19 patients on HFNC should be closely monitored to enable timely adjustment of respiratory support.
Using objective criteria when observing patients on HFNC can improve the detection of clinical failure and avoid delays in intubation. Our study suggests that, as in other cases of hypoxemic respiratory failure, 53 the ROX index (defined as the ratio of SpO2/FiO2 to respiratory rate) has high sensitivity in identifying HFNC failure in COVID-19 patients. In a previous study, the ROX index was considered a better predictor of successful HFNC than SpO2/FiO2 or respiratory rate alone when measured 2, 6, or 12 h after the initiation of HFNC in patients with severe community- or hospital-acquired pneumonia. A ROX index ⩾ 4.88 measured within 2–12 h of HFNC was associated with an increased likelihood of successful HFNC in treating nonviral pneumonia.53,54 However, because the studies in this meta-analysis measured the ROX index at very different time points, we only used the latest ROX index after the initiation of HFNC in the analysis. As the condition of COVID-19 patients changes quickly, treatment providers should closely monitor changes in the ROX index after the initiation of HFNC. Whether more sensitive indicators such as ROX-HR and mROX 55 are better than ROX for monitoring COVID-19 patients needs to be studied further.
The inflammatory response associated with mortality appears to be dysregulated in response to COVID-19, and this likely drives the high mortality among critically ill patients with COVID-19. 56 Pooled ORs showed that a higher WBC count was associated with an increased risk of HFNC failure. A previous study found that patients with more severe disease had a higher WBC count. 57 However, we found no difference in inflammatory indices between the failure and success groups (Table 5), although pooled ORs showed that an increased WBC count was a risk factor for HFNC failure. This contradictory result may be due to the fact that these results came from different studies. Further study may be needed to verify this.
The present study has several limitations. First, our results were based mostly on cohort and case-control studies, and the quality of the evidence in the studies was low. The lack of RCTs may have reduced accuracy and increased heterogeneity. Second, as the distribution of resources and recommended guidelines differed in different countries during the COVID-19 epidemic, there was no clear protocol for initiating HFNC. Thus, treatment results depended on the judgment of individual physicians and differences in patient selectivity of HFNC, which may have affected our results. Third, data on biomarkers were incomplete, which reduced the power of the multivariate predictive model. Some important indicators were also incomplete, such as the time of failure and the day of illness, are very important for the failure prediction of HFNC, future research focus on these is needed. Some variables were likely skewed and would best be reported as medians with interquartile ranges and compared using a non-parametric statistical test, but this maybe related to the original data provided by the included study. Finally, we did not examine whether HFNC reduced intubation and mortality rates compared to conventional oxygen therapy or NIV; further studies may be needed.
Conclusions
Our meta-analysis found an aggregated failure rate of HFNC in COVID-19 patients of 0.47 and intubation and mortality rates of 0.44 and 0.23, respectively. Pooled ORs showed that older age, a higher WBC count, a higher heart rate, and a lower ROX index after the initiation of HFNC were associated with an increased risk of HFNC failure.
Supplemental Material
sj-pdf-1-tar-10.1177_17534666221091931 – Supplemental material for Effectiveness of the use of a high-flow nasal cannula to treat COVID-19 patients and risk factors for failure: a meta-analysis
Supplemental material, sj-pdf-1-tar-10.1177_17534666221091931 for Effectiveness of the use of a high-flow nasal cannula to treat COVID-19 patients and risk factors for failure: a meta-analysis by Dong-yang Xu, Bing Dai, Wei Tan, Hong-wen Zhao, Wei Wang and Jian Kang in Therapeutic Advances in Respiratory Disease
Footnotes
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This meta-analysis was funded by the Science and Technology Planning Project, Shenyang (21-172-9-12).
Registration
This review protocol was prospectively registered with PROSPERO (no. CRD42021261541).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.