
Abstract
Background and Aims:
Physical inactivity is considered an important lifestyle factor for overweight and cardiovascular disease. We aimed to investigate the association between pre-existent physical inactivity and the risk of severe coronavirus disease 2019 (COVID-19).
Methods:
We included 164 (61.8 ± 13.6 years) patients with COVID-19 who were admitted between 15 February and 14 March 2020 in this retrospective study. We evaluated the association between pre-existent physical inactivity and severe COVID-19 using a logistic regression model.
Results:
Of 164 eligible patients with COVID-19, 103 (62.8%) were reported to be physically inactive. Univariable logistic regression analysis showed that physical inactivity was associated with an increased risk of severe COVID-19 [unadjusted odds ratio (OR) 6.53, 95% confidence interval (CI) 1.88–22.62]. In the multivariable regression analysis, physical inactivity remained significantly associated with an increased risk of severe COVID-19 (adjusted OR 4.12, 95% CI 1.12–15.14) after adjustment for age, sex, stroke, and overweight.
Conclusion:
Our data showed that pre-existent physical inactivity was associated with an increased risk of experiencing severe COVID-19. Our findings indicate that people should be encouraged to keep physically active to be at a lower risk of experiencing a severe illness when COVID-19 infection seems unpredicted.
The reviews of this paper are available via the supplemental material section.
Introduction
The coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection has posed a significant threat to the public. 1 It is critical to identify characteristics of people who may be at a high risk of experiencing severe SARS-CoV-2 infection to inform timely intervention. Some factors such as older age, hypertension, diabetes, or a previous history of pulmonary disease increase the severity of COVID-19.2,3 Previous studies also showed that overweight and cardiovascular disease were associated with a poor outcome in patients with COVID-19.4,5 Physical inactivity is considered an important lifestyle factor for overweight and cardiovascular disease. Several studies have shown that patients who took regular physical activity had a lower incidence, severity, and mortality from viral infections.6–8 Physical inactivity might be associated with poor immune response via the vicious cycle between inactivity and obesity,9,10 exerting a negative impact on immune function and host defense. Exercise may affect susceptibility to infection by modifying monocyte and lymphocyte distribution, phenotype, and cytokine release. 11 A previous large-scale general population study showed that physical inactivity [relative risk 1.32, 95% confidence interval (CI) 1.10–1.58] was associated with an increased risk of COVID-19 hospital admission; 12 however, whether pre-existent physical inactivity has a role in the severity of COVID-19 remains unclear. Since regular physical activity reduces the risk of systemic inflammation, a main contributor to pneumonia due to SARS-CoV-2 infection, we hypothesized that physical inactivity may play an important role in mitigating the severity of COVID-19. We therefore investigated the association between pre-existent physical inactivity and severe COVID-19 in this retrospective study.
Methods
Standard protocol approvals, registrations, and patient consent
The ethics committee of Fujian Medical University Union Hospital approved this study. All clinical investigations were conducted according to the principles expressed in the Declaration of Helsinki. Written informed consent was waived due to the nature of our retrospective study of routine clinical data.
Data collection and outcome measures
We analyzed the data of 164 consecutive patients with COVID-19 at the Tumor Center of Union Hospital (Wuhan, China) between 15 February 2020 and 14 March 2020 in this study. The epidemiological, demographic, clinical, laboratory, and radiological data were extracted from a digital database using a standardized data collection form. If data were missing or uncertain from the medical records, we obtained and clarified data by direct communication with attending doctors and other healthcare providers. To assess the pre-existent physically active status, we employed a well-validated Exercise Vital Sign evaluation method. 13 Briefly, we asked participants or their caregivers two questions: “On average, how many days (0–7) per week does the patient engage in moderate to strenuous exercise?” and “On average, how many minutes does the patients engage in exercise at this level?”. We recorded minutes in blocks of 10: 0, 10, 20, 30, 40, 50, 60, 90, 120, and 150 or greater. Physical inactivity was defined as <150 min/week of moderate activity or <75 min/week of vigorous activity. 13 Laboratory confirmation of COVID-19 infection was performed as previously described. 14 Our primary outcome was severe COVID-19 defined as fever or suspected respiratory infection, plus one of: respiratory rate >30 breaths/min; severe respiratory distress; Peripheral capillary oxygen saturation (SPO2) ⩽93% on room air based on World Health Organization clinical management of severe acute respiratory infection when COVID-19 is suspected: interim guidance. 15 Our second outcome was death, which was limited by the end of our observation (14 March 2020).
Statistical analysis
Data were summarized with mean value with standard deviations or median value with interquartile range and categories data as counts with percentages. We used the t-test or Mann–Whitney U test to compare the differences in continuous variables, and the chi-square test or Fisher’s exact test to compare the differences in categorical variables as appropriate. We used univariable and multivariable logistic regression analysis to evaluate the association between physical inactivity and 30-day severe COVID-19. For multivariable analysis, we chose the variables based on previous findings and clinical constraints to avoid overfitting the logistic regression model. 16 We therefore included hypertension, chronic obstructive pulmonary disease (COPD), coronary heart disease, tumor, renal impairment, decreased leucocytes, decreased lymphocytes, increased lactate dehydrogenase and chest computed tomography (CT) findings as potential confounders each in turn along with age and sex in the regression model. We also included the pre-existent comorbidity with p < 0.05 in the univariable regression analysis along with age and sex into the final multivariable regression model. All analyses were performed using SPSS for Windows (SPSS 25.0, IBM).
Data available statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Results
Of 164 eligible patients with COVID-19, 103 (62.8%) were reported to be physically inactive. The demographics and clinical and radiological characteristics of patients with and without physical inactivity are shown in Table 1. Patients with physical inactivity were similar to those without physical inactivity in comorbidities (except the previous stroke), exposure to wet seafood market, onset symptoms, and laboratory and radiological findings. Patients who were physically inactive were older (63.6 ± 18.8 years versus 58.7 ± 13.9 years), and more likely to have had a previous stroke [6 (5.8%) versus 0 (0.0%)]. Patients who were physical inactive had more severe COVID-19 [26 (25.2%) versus 3 (4.9%)] and mortality [6 (5.8%) versus 0 (0.0%)].
Demographic, clinical, laboratory, radiological characteristics, treatment, and outcome between patients with and without physical inactivity.
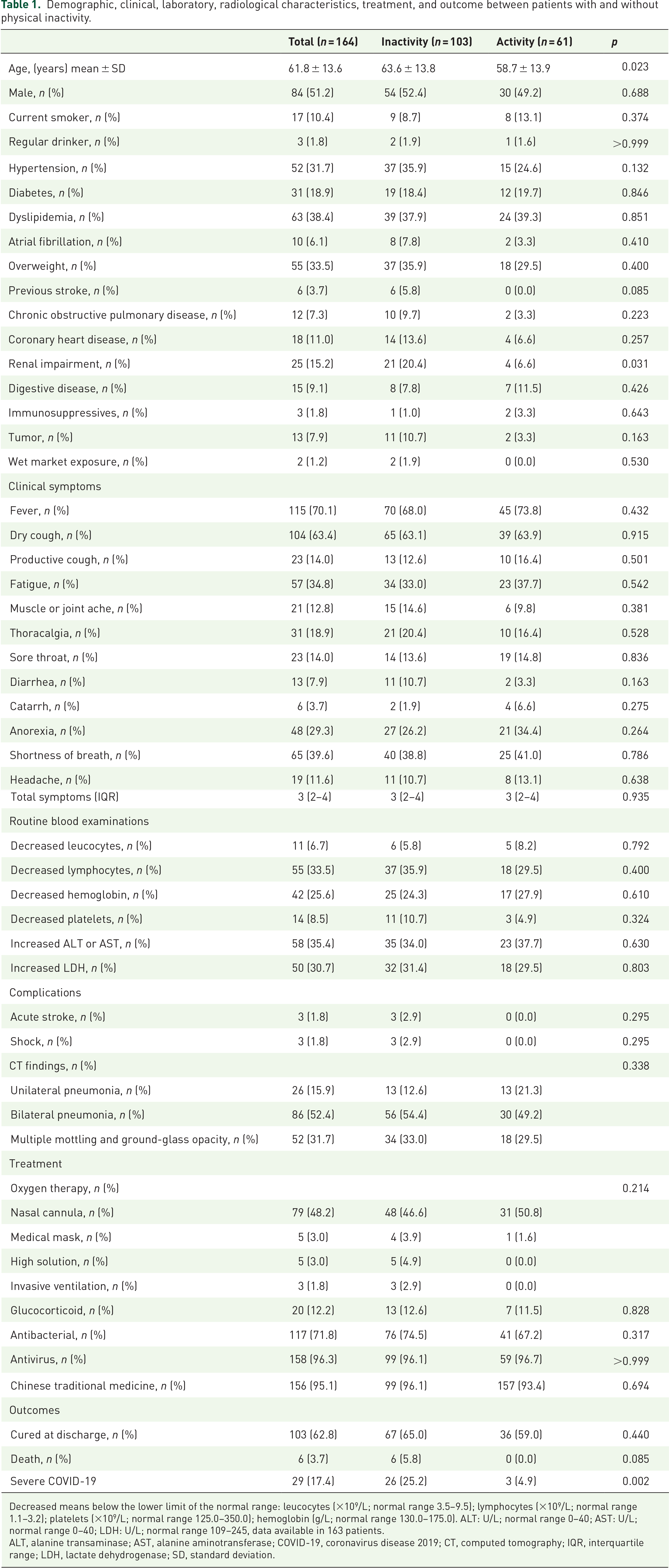
Decreased means below the lower limit of the normal range: leucocytes (×109/L; normal range 3.5–9.5); lymphocytes (×109/L; normal range 1.1–3.2); platelets (×109/L; normal range 125.0–350.0); hemoglobin (g/L; normal range 130.0–175.0). ALT: U/L; normal range 0–40; AST: U/L; normal range 0–40; LDH: U/L; normal range 109–245, data available in 163 patients.
ALT, alanine transaminase; AST, alanine aminotransferase; COVID-19, coronavirus disease 2019; CT, computed tomography; IQR, interquartile range; LDH, lactate dehydrogenase; SD, standard deviation.
A total of 29 patients (17.7%) experienced severe COVID-19 during our observations. In the univariable logistic regression analysis, physical inactivity was associated with an increased risk of severe COVID-19 [unadjusted odds ratio (OR) 6.528, 95% CI 1.88–22.62]. This association remained after adjustment for age and sex (Table 2). Additional adjustment for coronary heart disease, COPD, and tumor or renal impairment separately as confounders in addition to age and sex did not change the relationship between physical inactivity and severe COVID-19. In the multivariable regression analysis, physical inactivity remained significantly associated with an increased risk of severe COVID-19 (adjusted OR 4.12, 95% CI 1.12–15.14).
Association between physical inactivity and severe COVID-19.

Multivariable = adjustment for age, sex, stroke, and overweight.
CHD, coronary heart disease; CI, confidence interval; COVID-19, coronavirus disease 2019; OR, odds ratio.
Discussion
Our main finding was that patients with physical inactivity who had a SARS-CoV-2 infection were at an increased risk of experiencing severe COVID-19, indicating that physical inactivity might be a hazardous behavior for COVID-19 severity.
Our findings were in line with a large sample observational study (n = 48,440) that showed patients with COVID-19 who were consistently physically inactive had a higher risk of admission to the intensive care unit (OR 1.73; 95% CI 1.18–2.55) and mortality (OR 2.49; 95% CI 1.33–4.67) than patients who were consistently meeting physical activity guidelines. 17 Several physiological processes might explain the relationship between physical activity and improved immune and respiratory function, supporting the association between physical inactivity and higher risk of severe COVID-19. Regular physical exercise can increase immune cells and improve immune health. Prolonged moderate aerobic exercise has been previously proven to contribute some positive benefits on influenza (or pneumonia) immunization. Possible mechanisms of exercise-induced benefits may include the role of endogenous opioids, inflammatory biomarkers, or memory to naïve T lymphocyte ratio. 18 Moreover, regular physical exercise could upregulate the expression of antiviral immunity markers, lead to higher activation and proliferation of T cells, and proper balance of T-helper responses, enhancing natural killer cell activity that optimizes the systemic immune response. 19 Some researchers proposed that even a small increase in baseline maximal oxygen uptake across the population may have the effect of shifting a significant proportion of high-risk patients into a lower risk category. 20 Further investigations are needed to determine whether physical exercise would confer immune protection to patients with COVID-19 with cardiovascular and metabolic disorders. 11
During the COVID-19 pandemic, people worldwide were encouraged to stay at home to avoid contact with individuals outside to minimize the spread of SARS-CoV-2. People therefore had very limited access to physical and sports facilities due to lockdowns, so the risk of physical inactivity increased. Our findings suggest physical inactivity is a modifiable risk factor for severe COVID-19 outcomes. We therefore propose that people should keep structured activity as a critical strategy for optimizing the immune system’s functional integrity to prevent severe COVID-19 infection. Indoor or home-based physical exercise is a low-cost approach to maintaining appropriate immune responsiveness that might contribute to prevention or remediation of COVID-19. 20
The main limitation of our study was that it was a retrospective study conducted at a single-centered hospital with a limited sample size. Moreover, physical inactivity was assessed by two simple questions, so their prevalence may be misestimated. However, data from a previous study supported the use of this self-reported exercise assessment in diverse patient populations in clinical practice. 13 Notably, this approach can be finished within 1 min, without additional staff and medical resources, and can generally be used in most medical institutions worldwide, even under the unprecedented COVID-19 pandemic conditions. Lastly, we only included Chinese patients with COVID-19 during the first wave of the pandemic in the present study; caution should be taken about generalizing our findings to other COVID-19 populations.
Conclusion
Pre-existent physical inactivity seems to influence the course of COVID-19 infection. Our findings indicated that adopting simple lifestyle changes could lower the risk of severe COVID-19; people should keep physical active to be at a lower risk of experiencing severe illness if a COVID-19 infection occurs.
Supplemental Material
sj-pdf-1-tar-10.1177_17534666211025221 – Supplemental material for Does pre-existent physical inactivity have a role in the severity of COVID-19?
Supplemental material, sj-pdf-1-tar-10.1177_17534666211025221 for Does pre-existent physical inactivity have a role in the severity of COVID-19? by Qilin Yuan, Hua-yao Huang, Xiao-ling Chen, Rong-hua Chen, Yixian Zhang, Xiao-bin Pan, Jun-nian Chen, Nan Liu and Houwei Du in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-2-tar-10.1177_17534666211025221 – Supplemental material for Does pre-existent physical inactivity have a role in the severity of COVID-19?
Supplemental material, sj-pdf-2-tar-10.1177_17534666211025221 for Does pre-existent physical inactivity have a role in the severity of COVID-19? by Qilin Yuan, Hua-yao Huang, Xiao-ling Chen, Rong-hua Chen, Yixian Zhang, Xiao-bin Pan, Jun-nian Chen, Nan Liu and Houwei Du in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-3-tar-10.1177_17534666211025221 – Supplemental material for Does pre-existent physical inactivity have a role in the severity of COVID-19?
Supplemental material, sj-pdf-3-tar-10.1177_17534666211025221 for Does pre-existent physical inactivity have a role in the severity of COVID-19? by Qilin Yuan, Hua-yao Huang, Xiao-ling Chen, Rong-hua Chen, Yixian Zhang, Xiao-bin Pan, Jun-nian Chen, Nan Liu and Houwei Du in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
We thank all the patients for their data for this analysis. We thank the medical workers who are on the front line of caring for patients.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fujian Natural Science Foundation (2018J01309) and the Fujian Provincial Natural and Science Innovation Project (No. 2016B014).
On behalf of the Fujian Medical Team Support Wuhan for COVID-19.
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.