
Abstract
Aims:
To evaluate the efficacy of medical thoracoscopy-assisted argon plasma coagulation in association with autologous blood pleurodesis in spontaneous pneumothorax.
Patients and methods:
Three male patients with spontaneous pneumothorax were treated; medical thoracoscopy-assisted argon plasma coagulation combined with autologous blood pleurodesis was conducted for all patients whose duration of the air leak exceeded 7 days. We systematically reviewed all of the relevant literature to analyze and sum up the treatments of secondary spontaneous pneumothorax.
Results:
The air leaks were all sealed and no recurrence of pneumothorax was reported. No complications of fever, bleeding, or signs of infection were observed during the process.
Conclusion:
The authors believe that the combination of medical thoracoscopy-assisted argon plasma coagulation and autologous blood pleurodesis is safe and effective. However, due to the number of patients included in this uncontrolled case study, more cases will be collected in the future.
The reviews of this paper are available via the supplemental material section.
Introduction
Spontaneous pneumothorax is defined as the presence of air in the pleural space with no apparent precipitating factor present (such as trauma) and is classified into two types. 1 The first type is primary spontaneous pneumothorax (PSP), and the other is secondary spontaneous pneumothorax (SSP). The classification depends on the absence or presence of any underlying lung disease. PSP is the most common type of pneumothorax that is observed in otherwise healthy young males. In the US, the reported incidence of PSP in men is between 7.4 and 18 per 100,000 individuals per year, while PSP is reported to be 1.2–6 per 100,000 individuals per year in women. 2 SSP refers to pneumothorax that occurs in conjunction with underlying lung diseases such as chronic obstructive pulmonary disease (COPD), cystic fibrosis, or pneumocystis carinii pneumonia. 3
Since SSP is associated with a higher risk of recurrence due to pre-existing lung disease, this results in a higher incidence of complications and mortality.2,4 Therefore, new methods have been developed to more effectively treat SSP. The principle of argon plasma coagulation (APC) is to combine high-frequency electricity and argon gas flow to form a non-contact, high-frequency current between the probe and the tissue. APC is commonly used to control bleeding from a range of lesions. The process uses thermal effects to cause tissues to dry, contract, coagulate, and ultimately become inactivated. 5 APC also is particularly suitable to treat spontaneous pneumopleural alveolar bullae. It has been confirmed that thoracoscopy-assisted APC is an effective treatment for the general Chinese population, and especially for PSP patients. 6
Autologous blood pleurodesis was first reported by Robinson. 7 Dumire et al. 8 reported on the application of this technique for pneumothorax. Since then, autologous blood pleurodesis has been widely used to treat primary and secondary pneumothorax.9,10 This study reports on three patients with SSP who were treated using medical thoracoscopy-assisted APC in association with autologous blood pleurodesis.
Clinical data
Case 1
A 64-year-old male patient exhibited chronic cough, expectoration, and shortness of breath for 5 years. In 2019 he was diagnosed with COPD, but did not undergo regular inhalation treatment. A computed tomography (CT) scan revealed the presence of a barrel chest and bullae in the right lung that were primarily located in the superior lobe. Right pneumothorax had occurred repeatedly in this patient since 2016 and was treated using thoracic drainage. This was the fifth admission for worsening chest distress and shortness of breath for this patient. Physical examination revealed a barrel chest and weakened tactile and vocal fremitus. Percussion on the right chest demonstrated tympanic resonance. Arterial blood gas analysis indicated no hypoxemia. A CT scan revealed hydropneumothorax of the right lung and a 40% pneumothorax. A 35 mm hydrothorax was detected using ultrasound. Thoracic drainage of 24F was conducted after admission. An air leak was still present after two treatments of 60 ml autologous blood pleurodesis on the sixth and eighth day after the patient was first admitted. Assessment of thoracic surgical team was completed, surgery was unavailable 是 as poor lung and cardiac function. Thoracoscopy was performed on the 10th day. Pleural adhesions were observed in the right pleural cavity, and several bullae with diameters greater than 2 cm and one larger bulla with a diameter greater than 5 cm were distributed at the apex pulmonis (Figure 1). The pleural fluid had not been sent for analysis as no lesions in parietal pleura were found. During the thoracoscopy, the bullae were coagulated using argon ions, and the bullae all shrank substantially after coagulation (Figure 2). Autologous blood pleurodesis was performed at the second day after the thoracoscopy, using 60 ml of autologous blood. The air leak was sealed by the fifth day, and the patient was discharged after removal of the chest drain. The patient did not exhibit fever, hemorrhage, infection or tube blockage. A CT scan was conducted after thoracoscopy, no pneumothorax was observed. A 2-month follow-up examination of the patient that included a plain chest radiograph demonstrated that the pneumothorax had not recurred.
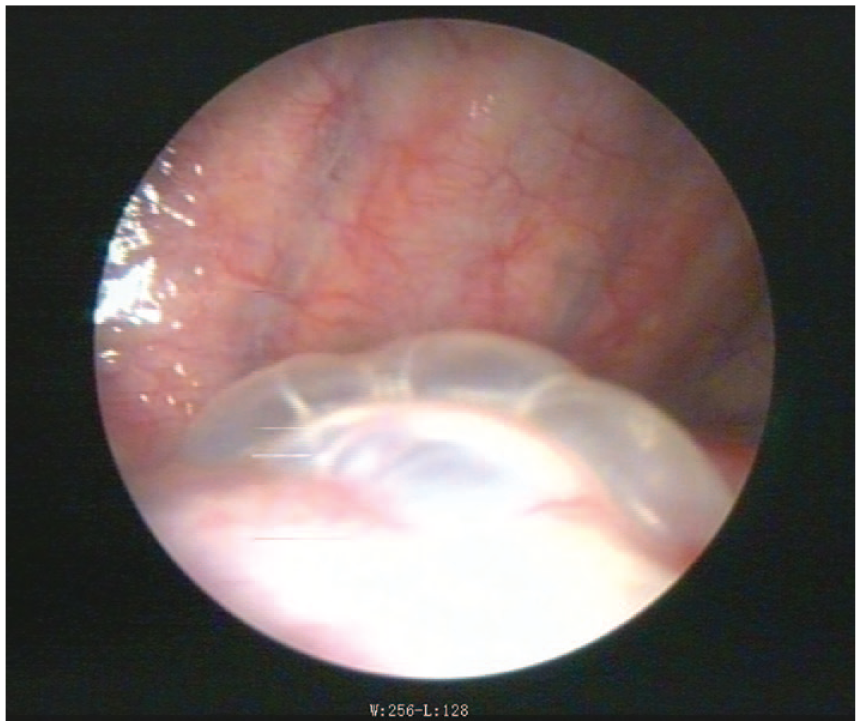
The larger bulla with a diameter >5 cm of Case 1.

The bullae shrank substantially after coagulation.
Case 2
A 72-year-old male presented with a history of pneumothorax that occurred 2 years previously and had experienced chronic cough, expectoration, and shortness of breath for 10 years. He was diagnosed with COPD in 2018 and received regular inhalation treatments of budesonide and terbutaline. The patient was hospitalized with the symptoms described above as well as fever. A CT scan revealed mild hydrothorax and a hydropneumothorax of 70%. Thoracic drainage of 24F was performed, but after 3 days, the air leaks persisted. A CT scan at our hospital revealed multiple pulmonary bullae, as well as reduced and disorganized pulmonary vascular markings. The thoracic surgery department was consulted concerning the poor cardiopulmonary status of the patient associated with his diffuse lung injury and comorbid illness, which could lead to a higher risk of death during or after surgery. Based on our consultations, 60 ml autologous blood pleurodesis was performed on the ninth and 11th days after admission to the hospital, which relieved the patient’s shortness of breath. However, a subsequent CT image revealed a pneumothorax of 20% and bubbles were observed in the water-sealed bottle. Thoracoscopy was performed. Pleural adhesions were observed in the right pleural cavity, several thin-walled bullae with diameters less than 2 cm were observed in the superior lobe, and a larger bulla with a diameter greater than 5 cm was located in the inferior lung lobe. The pleural fluid had not been sent for analysis as no lesions in the parietal pleura were found. The bullae were coagulated using argon ions. All bullae in the right superior lung lobe shrank, and the larger bulla was reduced by approximately 60% after the coagulation. The chest drain was removed 3 days after the procedure; no fever, bleeding or signs of infection and tube blockage were seen. The patient was discharged after an additional 2 days. Follow-up of physical examination and chest radiography had not been taken because he had a long journey to the hospital. At a 10-month follow-up phone interview, no recurrence of pneumothorax was reported.
Case 3
A 58-year-old male patient was diagnosed with COPD for over 10 years and was given regular inhalation treatments since the diagnosis. The patient had been treated with thoracic drainage three times, in 2012, 2017, and 2019, due to recurring pneumothorax. The patient was hospitalized for the presence of cough, expectoration, and anhelation. Chest radiographs demonstrated a right pneumothorax and pneumonia. Physical examination revealed the presence of a barrel chest, a subcutaneous swelling on the right chest, and weak tactile and vocal fremitus. Percussion demonstrated tympanic resonance. A CT scan showed multiple regions of subcutaneous emphysema of the chest wall and multiple pulmonary bullae. Thoracic drainage of 24F was performed and the air leaks did not improve. The thoracic surgery department also suggested conservative treatment rather than surgery because of poor lung function and nutrition status. Thoracoscopy was performed on the sixth day after admission to the hospital. Several bullae with diameters between 3 cm and 5 cm formed a cluster in the superior lobe. The bullae were coagulated using argon ions, and all bullae shrank substantially after the coagulation. On the third day after the thoracoscopy, the drainage tube still was not removed because of worsening anhelation, and air leaks still were present. Subsequently, autologous blood pleurodesis was performed on the eighth and 10th days after thoracoscopy, and the air leaks were sealed. The chest drain was removed on the 13th day after thoracoscopy. No complications of infection, bleeding or tube blockage were observed. The follow-up of physical examination and chest radiography had not been taken as the patient moved to another city after discharging. At a 3-month follow-up phone interview, no recurrence of pneumothorax was reported.
Discussion and literature review
COPD has been cited as the most frequent lung disease that is associated with SSP, with a reported range of 57–70%.11,12 In one report that compared age-matched controls with and without COPD, each pneumothorax occurrence in patients with COPD increased the risk of mortality by 3.5 times. 13 Surgical resection, extending the indwelling time for the drainage, and chemical pleurodesis (including use of hypertonic glucose pleurodesis, tetracycline, talc, and other sclerosing agents) may be preferred if air leaks persist after thoracic drainage. However, most patients with refractory pneumothorax who have poor basic cardiopulmonary function or poor nutritional status are unable to tolerate surgery. Hypertonic glucose, talc, and tetracycline each have serious side effects, and their use can often cause severe chest pain and lung infections, and even result in acute respiratory distress syndrome. 14 Many domestic and international reports have discussed the use of thoracoscopy or autologous pleural fixation, but there are still occurrences of air leaks with these procedures.6,9,15–19 So far no combinations of APC plus talc or other mechanical abrasion were reported. The current opinion concerning persistent or repeated air leaks is that the pulmonary bullae repeatedly rupture, and the resulting wound is challenging to heal. Therefore, to promote healing of lung tissues and benign adhesions in the pleural cavity, as well as block and reduce pulmonary rupture, it is necessary to reduce the incidence of pneumothorax.
All three patients included in this report were older patients with COPD and experienced secondary pneumothorax due to ruptured pulmonary bullae. Video-assisted thoracoscopic surgery requires general anesthesia, a trachea cannula, and using a straight aligner to cut and sew the bullae, which might result in higher risk to the patients. 20 Therefore, because of the age and poor health status of the patients in this study, we used medical thoracoscopy-assisted APC. During the process of thoracoscopy, local infiltration anesthesia was performed to avoid the risk associated with the use of a trachea cannula and general anesthesia. No positive pressure ventilation was needed. For the first two cases, autologous blood pleurodesis was conducted before the thoracoscopy, which had little effect. Hence we combined APC with autologous blood pleurodesis to promote benign pleural adhesions and reduce the occurrence of pulmonary alveolar ruptures. A study by Gan and Liu 18 reported diffuse distribution of bullae in intractable pneumothorax patients when they were examined using medical thoracoscopy and exhaust only treatment was used. If large bullae are not reduced, intermittent alveolar rupture may lead to recurrent pneumothorax. 18 Traditional thoracotomy is traumatic, results in extended hospital stays, and incurs high financial costs. The treatment of bronchial occlusion also has high financial costs, the need for collateral ventilation, and other problems. On the other hand, APC is an effective, safe, and affordable treatment for recurrent pneumothorax, especially in older patients. 21 The depth of tissue penetration can be controlled with APC, and it is possible to treat “around the corner” lesions. 5
Gan and Liu 18 observed 12 patients with refractory pneumothorax who were treated with thoracoscopic APC, and their air leaks were stopped entirely within 1 week after the procedure. For two patients, the air leak stopped immediately after surgery, in five patients the leak stopped within 3 days after surgery, and in the remaining five patients the leak stopped within 1 week after surgery. 18 In another study that included 14 patients with pneumothorax, all of the patients underwent complete pulmonary re-expansion 24–72 h after medical thoracoscopy. 19 Of those treated, the air leaks in 11 patients stopped within 3 days after surgery, and the other three patients underwent chest radiographs 7 days after surgery that demonstrated no air leaks were present. Both studies indicated that the patients experienced transient fever and chest pain after surgery, but these symptoms were relieved using antipyretic and analgesic treatment. 19 However, one limitation for both studies mentioned above is that they primarily included young male patients, with an average age of 37.7 ± 18.0 years and 29.67 ± 13.79 years, respectively. Also, the above studies mainly discussed the treatment of PSP; these were 11 of 12 cases and nine of 14 cases, respectively. A Japanese study found that the incidence of pneumothorax peaked at 80 years of age for women and 79 years for men. 22 For elderly patients, refractory pneumothorax is often secondary to chronic obstructive pulmonary disease. Elderly patients have poor tolerance of pneumothorax and difficulty in healing air leaks due to low body mass index, weak chest wall muscles, poor basal lung function, extensive lung lesions, low immunity, and other factors. 21 In the study of APC outcomes by Zhang et al. 6 the majority of patients stopped leaking air within 3 days after the surgery. However, some patients continued to leak air after APC, with the leakage in four patients exceeding 1 week. 6 Liu et al. 23 reported on eight patients who underwent thoracoscopy treatment and two of eight patients received two procedures. Three of the eight patients received APC without pleurodesis, and their air leakage continued for 6 days following the surgery. 23 Two of these patients were older men (aged 76 and 69 years). 23 These three patients were injected with autologous blood or erythromycin, which strengthened the formation of aseptic inflammation around the wounds and eventually promoted healing of the air leaks and conglutination between the parietal and visceral pleura. 23 This result supports intrathoracic autologous blood injections as an important procedure to include in the successful treatment of SSP. 23 Thoracoscopic APC plays a role in reducing bullae to prevent pneumothorax recurrence, which may be limited in promoting the formation of aseptic inflammation of the pleura, and autologous blood injection acts as a “patch” to promote benign pleural adhesions. In addition, after APC coagulating the lung bullae, more effective ventilation space will be provided, thereby improving the patients’ lung function in the later stage. Therefore, APC under medical thoracoscopy combined with autologous blood pleurodesis may be a better choice for elderly refractory pneumothorax patients or refractory pneumothorax patients who experience repeated air leaks after surgery.
Robinson, 7 the first to report on autologous blood pleurodesis, treated patients by injecting 50 ml of autologous blood through a chest tube to prevent the recurrence of pneumothorax. Subsequently, autologous blood has often been used as a blocking substance and adhesive rather than chemical pleurodesis because autologous blood is convenient to acquire and provides fibrin-rich self-coagulation. The real mechanism of action of autologous blood pleurodesis appears to be true pleurodesis or a “patch effect” due to the coagulated blood sealing the site of the air leak. 24 There have been many domestic and international reports of the use of autologous blood pleurodesis, including randomized controlled trials and clinical retrospective studies.16,25,26 In the study conducted by Ibrahim et al., 27 the success rate of the experimental group (50 ml autologous blood pleurodesis) was 78.3%, while the success rate of the control group that received a more conservative treatment was 8.33%. Rivas De Andrés et al. 25 used autologous blood pleurodesis to treat six patients with persistent air leaks, and all six cases were completely successful within 24 h after surgery.
However, the recommended dose for autologous blood pleurodesis is still controversial. In a randomized trial by Andreetti et al. 28 two groups of patients were randomly assigned to receive 50 or 100 ml of autologous blood, respectively, and the larger volume group demonstrated better results. Droghetti et al. 16 used larger volumes (100–150 ml) of autologous blood and observed that the pneumothorax was resolved earlier compared with reported cases that used smaller volumes of autologous blood. Akar et al. 29 compared patients who were injected with either 60 ml or 120 ml of autologous blood, respectively, and the results confirmed that patients who received 120 ml of autologous blood had significantly shorter pneumothorax leakage and extubation times compared with the times reported for patients in the 60 ml group. 29 In the Guo et al. 30 study, the patients were divided into four groups that received 0.5 ml/kg, 1 ml/kg, or 2 ml/kg of autologous blood or sterile normal saline, respectively. The results showed that the success rates associated with the larger volumes (1 ml/kg and 2 ml/kg) were significantly higher than the 0.5 ml/kg group. 30 The two groups that received the largest volumes of autologous blood achieved a success rate of 82%. There were no statistical differences in the success rate among the group that received 0.5 ml/kg autologous blood and the normal saline control groups. 30 These results indicated that larger volumes used in autologous blood pleurodesis achieved higher success rates. However, Lang-Lazdunski and Coonar 15 recommended using a maximum volume of 50 ml autologous blood due to a higher risk of septicemia that was associated with the use of larger blood volumes. Droghetti et al. 16 showed that if the first dose of blood failed to prevent air leakage within 48 h, then further treatment was needed. However, none of these reports provide conclusive evidence, as they are all studies that included only small numbers of patients. Large scale research studies are lacking.
In the three cases reported here, all three patients were in poor general health, their GOLD classification was a grade 4, and their air leaks could not be resolved using medically conservative treatments such as prolonged closed chest drainage time (Table 1). After medical thoracoscopic APC combined with autologous blood treatment, even though some patients experienced a long extubation time, all three patients were successfully treated. No recurrence of pneumothorax and no severe complications have been reported thus far for any of the three individuals. Therefore, for patients with refractory pneumothorax and underlying COPD or poor pulmonary function for other reasons, and who experience persistent pleural air leakage associated with pulmonary bullae, medical thoracoscopic APC combined with autologous blood therapy should be considered. Unfortunately, one limitation of this study is that only a small number of cases were observed. Also, additional systemic responses, such as inflammatory markers, were not evaluated after the procedure. Additional cases are expected to be collected in the future, which will provide more clinical evidence to resolve this challenging clinical problem.
Patient baseline characteristics.

APC, argon plasma coagulation; BMI, body mass index; CAT, COPD assessment test; COPD, chronic obstructive pulmonary disease; mMRC, modified British medical research council.
Supplemental Material
sj-pdf-1-tar-10.1177_1753466620986390 – Supplemental material for Assessment and review of treatment for secondary spontaneous pneumothorax using medical thoracoscopy-assisted argon plasma coagulation in association with autologous blood pleurodesis
Supplemental material, sj-pdf-1-tar-10.1177_1753466620986390 for Assessment and review of treatment for secondary spontaneous pneumothorax using medical thoracoscopy-assisted argon plasma coagulation in association with autologous blood pleurodesis by Lei Zhang, Tian Xie, Yihui Fu and Haihong Wu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-2-tar-10.1177_1753466620986390 – Supplemental material for Assessment and review of treatment for secondary spontaneous pneumothorax using medical thoracoscopy-assisted argon plasma coagulation in association with autologous blood pleurodesis
Supplemental material, sj-pdf-2-tar-10.1177_1753466620986390 for Assessment and review of treatment for secondary spontaneous pneumothorax using medical thoracoscopy-assisted argon plasma coagulation in association with autologous blood pleurodesis by Lei Zhang, Tian Xie, Yihui Fu and Haihong Wu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-3-tar-10.1177_1753466620986390 – Supplemental material for Assessment and review of treatment for secondary spontaneous pneumothorax using medical thoracoscopy-assisted argon plasma coagulation in association with autologous blood pleurodesis
Supplemental material, sj-pdf-3-tar-10.1177_1753466620986390 for Assessment and review of treatment for secondary spontaneous pneumothorax using medical thoracoscopy-assisted argon plasma coagulation in association with autologous blood pleurodesis by Lei Zhang, Tian Xie, Yihui Fu and Haihong Wu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-4-tar-10.1177_1753466620986390 – Supplemental material for Assessment and review of treatment for secondary spontaneous pneumothorax using medical thoracoscopy-assisted argon plasma coagulation in association with autologous blood pleurodesis
Supplemental material, sj-pdf-4-tar-10.1177_1753466620986390 for Assessment and review of treatment for secondary spontaneous pneumothorax using medical thoracoscopy-assisted argon plasma coagulation in association with autologous blood pleurodesis by Lei Zhang, Tian Xie, Yihui Fu and Haihong Wu in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-5-tar-10.1177_1753466620986390 – Supplemental material for Assessment and review of treatment for secondary spontaneous pneumothorax using medical thoracoscopy-assisted argon plasma coagulation in association with autologous blood pleurodesis
Supplemental material, sj-pdf-5-tar-10.1177_1753466620986390 for Assessment and review of treatment for secondary spontaneous pneumothorax using medical thoracoscopy-assisted argon plasma coagulation in association with autologous blood pleurodesis by Lei Zhang, Tian Xie, Yihui Fu and Haihong Wu in Therapeutic Advances in Respiratory Disease
Footnotes
Author contributions
Haihong Wu designed the research. Haihong Wu and Tian Xie performed the thoracoscopy, and Yihui Fu collected the data. Lei Zhang analyzed the data and wrote the paper.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Hainan Provincial Natural Science Foundation of China(819QN354).
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.