
Abstract
Background and aims:
Various prediction indices based on the single time point observation have been proposed in chronic obstructive pulmonary disease (COPD), but little was known about disease trajectory as a predictor of future exacerbations. Our study explored the association between disease trajectory and future exacerbations, and validated the predictive value of the modified and simplified short-term clinically important deterioration (CID).
Methods:
This study was a multicenter, prospective observational study. Patients with COPD were recruited into our study and followed up for 18 months. The modified CID (CID-C) was defined as a decrease of 100 mL in forced expiratory volume in 1 second (FEV1), or suffering exacerbations, or increase of 2 units in COPD Assessment Test (CAT) during the first 6 months follow-up. Simplified CID was defined when excluding CAT from the CID-C model.
Results:
A total of 127 patients were enrolled in our final analysis. Compared with patients without exacerbations during the period of the 6th to the 18th month, patients with exacerbations were more likely to have frequent short-term exacerbations in the first 6 months (2.14 versus 0.21, p < 0.001). The short-term exacerbations were the best predictor for future exacerbations [odds ratio (OR): 13.25; 95% confidence interval: 5.62–34.67; p < 0.001], followed by the history of exacerbation before study entry, short-term changes in FEV1 and CAT. CID-C and Simplified CID were both significantly associated with exacerbations (OR: 7.14 and 9.74, both p < 0.001). The receiver operating characteristic curves showed that the Simplified CID had slightly better predictive capacity for future exacerbation than CID-C (0.754 versus 0.695, p = 0.02).
Conclusion:
Disease trajectory, including both the CID-C and the Simplified CID had significant predictive value for future exacerbations.
The reviews of this paper are available via the supplemental material section.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) has been the fourth leading cause of mortality worldwide. 1 Exacerbations are critical outcomes in COPD patients, and they are defined as acute worsening of respiratory symptoms that result in additional therapies. 2 Exacerbations appear to accelerate the rate of hospitalization and readmission, increase the mortality 3 and social economic burden, 4 reduce physical activity, and decrease the quality of life in patients with COPD. 5 Therefore, prevention of exacerbation is one of the most important components of COPD management strategies.
Various individual factors have been proven to be associated with the occurrence of exacerbations in COPD patients, including a history of exacerbations, the severity of COPD, poorer quality of life, and decrease of lung function. 6 Beyond these individual risk factors, the multidimensional indices, such as BODE [body mass index (BMI), airflow obstruction, dyspnea, and exercise capacity] and BODEx (BMI, airflow obstruction, dyspnea, and exacerbations),7,8 ADO (age, dyspnea, and airflow obstruction), 9 B-AE-D and simplified B-AE-D (BMI, acute exacerbation, and dyspnea), 10 have improved the predictive capacity in the outcomes of COPD. These prediction indices were all observed at a single time point, and we knew little about the disease trajectory as a predictor of outcomes. Based on the post hoc analysis of the TORCH (TOwards a Revolution in COPD Health) trial data, researchers found that the occurrence of clinically important deterioration (CID) over 6 months, which was made up of moderate/severe exacerbations, worsening of forced expiratory volume in 1 s (FEV1) or St George’s Respiratory Questionnaire (SGRQ) total score, was associated with increased risk of a new moderate/severe exacerbation and all-cause death. 11 Some researchers also set up the first time to CID over 6 months or the CID status at the sixth month as the endpoint of their studies to assess and quantify individual levels of disease deterioration.12,13 However, none of those studies were prospectively designed to assess the prediction value of CID for COPD outcomes.
SGRQ is one of the most comprehensive disease-specific health status questionnaires in COPD patients, 14 but it is too complex to use in routine practice. The COPD Assessment Test (CAT) is an eight-item, simple instrument of health status for patients with COPD. 15 Studies have found that CAT correlates very closely with SGRQ, and the change of SGRQ also correlates significantly with the change of CAT. 16 At individual patient level, researchers identified –2 units as the minimum clinically important difference (MCID) of change of CAT score when –4 points change in SGRQ was used as anchor. 16
The interesting thing is that nearly all established and validated composite prognostic indices have not included the measure of health status of patients. So, we also wondered whether excluding health status from the CID model would limit risk prediction future exacerbations. In this study, we assessed the association between short-term risk factors and future exacerbations in patients with COPD. We also explored the predictive value of the occurrence of CID based on CAT [CID-C; we used CAT to measure the health status of patients with COPD] for future exacerbations, and whether the new simplified CID status, by removing CAT from the model, limits the risk prediction.
Methods
Study design and subjects
This study was a multicenter, prospective observational study based on data collected as part of the Chronic Pulmonary Diseases Database set up by the Second Xiangya Hospital of Central South University (Registration number: ChiCTR-POC-17010431). Patients were recruited during the period from December 2016 to June 2018. The study was approved by an Internal Review Board review from the Second Xiangya Hospital of Central South University (fabh001) and conducted in accordance with the Declaration of Helsinki and its amendments. All patients provided written informed consent.
All patients anticipating in the study accepted four visits. At the first visit (baseline), the clinical characteristics data of patients were collected. The airflow limitation severity and symptoms/risk of exacerbations were graded according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD). 17 After the baseline visit, patients were followed up at the sixth month, respectively, to record the spirometry results, CAT scores, modified Medical Research Council (mMRC), and exacerbations. Then, telephone follow-ups were conducted at the 12th and 18th months to record the rate of exacerbations. In our study, we used the number of events per variable (EPV) to calculate the sample size, and an EPV of 10 or more was applied when recruiting the patients. 18
Subjects recruited into the study were diagnosed with COPD according to GOLD2017. 17 The patients who diagnosed as or with a history of asthma (including asthma-COPD overlap), bronchiectasis, lung cancer, lung fibrosis, upper airway obstruction, tuberculosis or pulmonary infection in the last 4 weeks were excluded from our study.
Study outcomes
Exacerbations were important events in COPD management. In our study, we recorded moderate to severe exacerbations during the baseline visit and follow-ups. The moderate exacerbations were defined as an acute worsening of respiratory symptoms that require antibiotics and/or oral corticosteroid; a severe event was defined as exacerbation requiring hospitalization or emergency room visits for more than 2 days. 19 Frequent exacerbators were recognized if someone had at least two exacerbations or one hospitalization per year, or death during follow-ups. The short term in our study was defined as the period of the first 6 months, and the follow-up year was defined as the period during the sixth month to the 18th month follow-up.
Variables
The demographic characteristics of patients (including sex, age, BMI, education, smoking history), FEV1, CAT, and mMRC at the baseline and sixth month follow-up were all included in our models as variables to predict outcomes. As for smoking history, we defined “Never smoker” as smoking exposure less than 10 pack-years, “Ex-smoker” as not less than 10 pack-years but smoking cessation more than 6 months. 20
The modified CID (CID-C) in our study was defined as (1) the occurrence of moderate to severe exacerbation of COPD, or (2) a decrease of 100 mL in trough FEV1, 6 or (3) an increase of CAT score more than 2 units 16 over the first 6 months during follow-up. Simplified CID was defined when patients met the first two conditions of CID-C but despite the change of CAT score.
Statistical analysis
Descriptive data are reported as means ± SD, or median ± interquartile range, or percentages, as appropriate. Continuous variables were analyzed by Student’s t-test and Mann–Whitney U test, while categorical variables and ranked ordinal data were compared by Chi-square or Fisher’s test and Wilcoxon signed-rank test. For the multivariate logistic regression analyses, a stepwise approach was used. The variables with significant difference between two groups in the univariate model were included in the multivariate model. Age, sex, and BMI were considered in all models. Statistically significant difference was defined as two-sided and p values < 0.05. All analyses were performed by using SPSS (IBM SPSS, version 22.0) and R project.
Results
Patients’ characteristics
A total of 200 patients with COPD were considered for enrollment initially. After 6 months, 42 patients were excluded from our study because of refusing hospital visits (n = 32) and lack of spirometry data (n = 10). At the 12- and 18-month follow-ups, 31 patients dropped out because of losing contact. Finally, we recruited 127 patients for our final analysis (Figure 1). The baseline demographic and clinical characteristics are shown in Table 1, categorized according to the occurrence of exacerbations (including death) during the period of sixth month to18th month follow-up. The mean age of total patients is 59.54 ± 8.43 years old, and the majority of the patients were male (89.8%). Compared with patients without exacerbations, patients with exacerbations during the follow-up year were more likely to have frequent exacerbations (mean rates: 2.73 versus 1.03, p = 0.001) in the previous year before study entry.

Flow chart of the study. A total of 200 COPD patients were considered for enrollment at baseline visit. Forty-two patients were excluded from our study over the first 6 month interval, including 32 patients refusing to visit hospital at follow-up time and 10 patients lacking spirometry data. During the period of sixth to 18th month follow-up, 31 patients were lost to follow-up. Finally, we recruited 127 for our final analysis, including six patients who died during the period between the 12th and 18th months of follow-up.
Baseline characteristics of the patients according to the occurrence of exacerbations.

Data are shown as means (SD) or median(IQR) or % unless noted otherwise noted.
The follow-up year was defined as the period during 6th month to 18th month follow-up visit.
Patients suffering exacerbations included six death who died (from any cause) during follow-up year.
Frequent exacerbators were patients who suffered at least two exacerbations or one hospitalization or death per year.
BMI, body mass index; CAT, COPD Assessment Test; COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICS, inhaled corticosteroids; IQR, interquartile range; LABA, long-acting β-2-agonist; LAMA, long-acting muscarinic antagonist; mMRC, modified Medical Research Council; SD, standard deviation.
Exacerbations and change of spirometry, CAT, mMRC
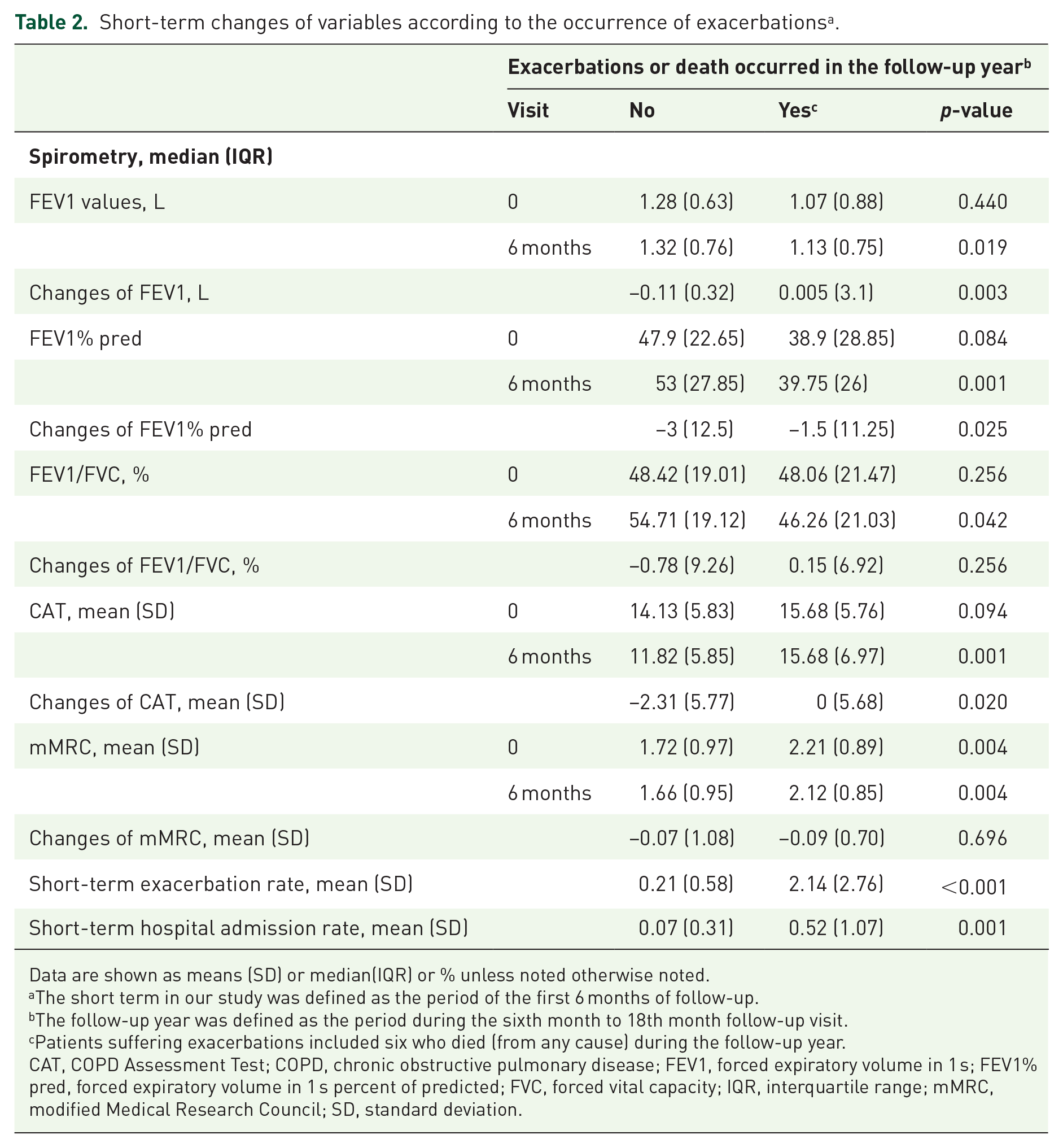
At baseline, there was no significantly statistical difference on FEV1, FEV1% predicted, FEV1/forced vital capacity (FVC) and CAT scores between patients with or without exacerbations in the follow-up year (during 6- month to18-month follow-up). But patients with exacerbations had significantly lower absolute FEV1 value (1.13 versus 1.32, p = 0.019), FEV1% predicted (39.75 versus 53, p = 0.001), FEV1/FVC (46.26% versus 54.71%, p = 0.042), and higher CAT score (15.68 versus 11.82) at 6-month follow-up (Table 2). Throughout the first two visits, the value of FEV1 promoted in patients without exacerbations, while it decreased in patients with exacerbations. CAT score had no much difference between baseline and 6-month follow-up in patients with exacerbations, but significantly decreased in the non-exacerbation group at 6-month follow-up. Significant difference also existed in the short-term change of FEV1, FEV1% predicted, and CAT scores between the patients with or without exacerbations. No significant difference had been found in the change of mMRC scores. The mean rate of short-term exacerbations is much higher in patients with exacerbations (2.14 versus 0.21, p < 0.001) than in patients without exacerbations. Those participants who had exacerbation or hospital admission in the first 6 months of follow-up seemed more likely to suffer exacerbations in the follow-up year, i.e., 84.6% of short-term exacerbators had exacerbations in the following year.
Short-term changes of variables according to the occurrence of exacerbations a .
Data are shown as means (SD) or median(IQR) or % unless noted otherwise noted.
The short term in our study was defined as the period of the first 6 months of follow-up.
The follow-up year was defined as the period during the sixth month to 18th month follow-up visit.
Patients suffering exacerbations included six who died (from any cause) during the follow-up year.
CAT, COPD Assessment Test; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 s; FEV1% pred, forced expiratory volume in 1 s percent of predicted; FVC, forced vital capacity; IQR, interquartile range; mMRC, modified Medical Research Council; SD, standard deviation.
Additionally, among patients reporting no exacerbation in the year before study entry, 80% of patients also had no exacerbation during the first 6 months and 55.6% patients had no exacerbation in the whole follow-up period (sustained non-exacerbators). Among patients with at least one exacerbation in the year before enrollment, 52.4% patients also had exacerbation during the first 6 months and 45.1% patients suffered exacerbations in both periods of the first 6 months and of the 6–18 month interval (sustained exacerbators) (Figure 2).

Association of the history of exacerbations with the occurrence of future exacerbations. Patients with exacerbations in the year before study entry were considered more likely to have future exacerbations during the first 6 months and the whole 18 months of follow-up. The sustained exacerbators were also more frequent in those patients with a history of exacerbations.
Risk factors associated with exacerbations
By univariate logistic-regression analysis, we accessed the risk factors associated with the occurrence of at least one exacerbation in the follow-up year. All available assessments at baseline and the sixth month follow-up were included in the model. The best predictor of an exacerbation in the follow-up year was the short-term occurrence of exacerbation [odds ratio (OR): 13.25; 95% confidence interval (CI): 5.62–34.67; p < 0.001]; second was the occurrence of exacerbations in the year before entry (OR: 2.12; 95% CI: 1.02–4.50; p = 0.0471). Other factors significantly associated with exacerbations are shown in Table 3. Based on the analysis, sex, age, BMI, and other variables which had significant difference between the two groups were all included in the stepwise multivariate model, including exacerbation in the past 12 months (any versus none), FEV1, FEV1% predicted, CAT scores at sixth month follow-up and their changes from baseline, the short-term occurrence of exacerbations, and hospital admission. Interestingly, only the short-term occurrence of exacerbations and the decrease of absolute FEV1 remained in the final model, and the short-term change of CAT had been excluded from our model (Table 4).
Univariate analysis of risk factors’ associations with the occurrence of exacerbations a .

Patients suffering exacerbations included six who died (from any cause) between the 6th month and 18th month follow-up visits.
The short term in our study was defined as the period of the first 6 months of follow-up.
BMI, body mass index; CAT, COPD Assessment Test; CI, confidence interval; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 s; FEV1% pred, forced expiratory volume in 1 s percent of predicted; FVC, forced vital capacity; mMRC, modified Medical Research Council; OR, odds ratio.
Factors associated with the occurrence of exacerbations in the stepwise multivariate model a .

Patients suffering exacerbations included six who died (from any cause) between the 6th month and 18th month follow-up visits.
The short term in our study was defined as the period of the first 6 months of follow-up.
CI, confidence interval; FEV1, forced expiratory volume in 1 s; OR, odds ratio.
CID-C and Simplified CID as an independent factor associated with exacerbation
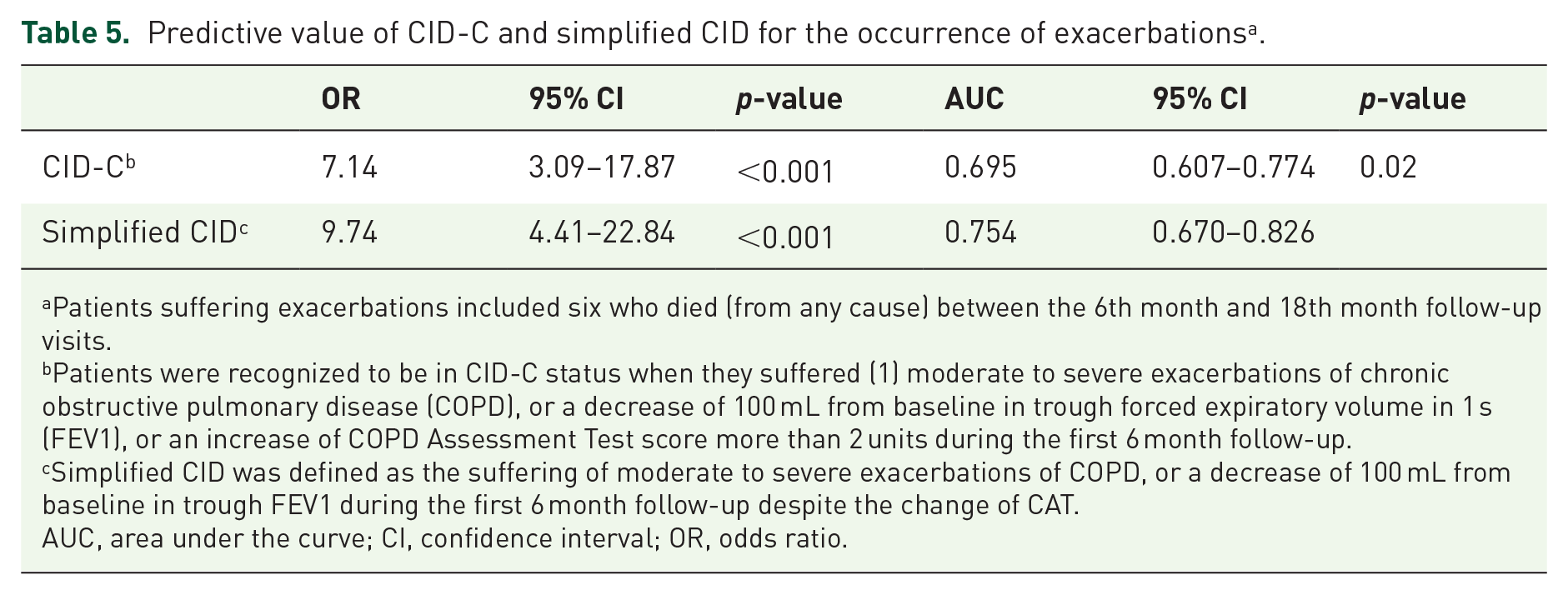
Based on multivariate model, the simplified CID (Simplified CID) was defined by removing CAT from the model. Thus, we recognized patients as being in Simplified CID status if they had exacerbations or a decrease of 100 mL in trough FEV1 during the first 6 months of follow-up. Both CID-C and Simplified CID were good predictors of exacerbations (Table 5): the ORs were 7.14 (p < 0.001) and 9.74 (p < 0.001), respectively. The receiver operating characteristic (ROC) curves showed that Simplified CID had a slightly better predictive capacity for the occurrence of exacerbation than CID-C (0.754 versus 0.695, p = 0.02). The sensitivity to identify exacerbations of Simplified CID and CID-C was 80.3% and 83.3%, and the specificity was 70.5% and 55.7%, respectively. In our study, among patients in Simplified CID and CID-C status, 74.6% and 67.1% patients seemed to suffer exacerbations in the following year. Among patients without Simplified CID and CID-C, they possibly had 76.8% and 75.6% chance to not suffer exacerbations in the future year (Figure 3).
Predictive value of CID-C and simplified CID for the occurrence of exacerbations a .
Patients suffering exacerbations included six who died (from any cause) between the 6th month and 18th month follow-up visits.
Patients were recognized to be in CID-C status when they suffered (1) moderate to severe exacerbations of chronic obstructive pulmonary disease (COPD), or a decrease of 100 mL from baseline in trough forced expiratory volume in 1 s (FEV1), or an increase of COPD Assessment Test score more than 2 units during the first 6 month follow-up.
Simplified CID was defined as the suffering of moderate to severe exacerbations of COPD, or a decrease of 100 mL from baseline in trough FEV1 during the first 6 month follow-up despite the change of CAT.
AUC, area under the curve; CI, confidence interval; OR, odds ratio.

Prevalence of exacerbations during the posterior follow-up year in patients with CID-C or Simplified CID. (A) The prevalence of exacerbations during the period of 6th month to 18th month follow-up in patients with CID-C (CID-C+) (69.0%) was higher than that in patients without CID-C (CID-C–) (19.6%). (B) The prevalence of exacerbations during the period of 6th month to 18th month follow-up in patients with Simplified CID (SCID+) (62.2%) was higher than that in patients without simplified CID (SCID–) (20.0%).
Discussion
In the present study, we investigated the relationship between the disease progression in a 6 month interval and future exacerbations. We found that exacerbations and more than 100 mL decrease of FEV1 over 6 months had significantly predictive value for the occurrence of exacerbations in the subsequent year. Patients in short-term CID-C status were more likely to suffer exacerbations in the following year, and the prediction capacity was maintained or even better in Simplified CID when removing CAT from the CID-C model.
Exacerbations were one of the most important events of patients with COPD, which increased physical burden in patients and economic burden at both individual and social levels.4,5 A recent study also revealed that severe exacerbation was an independent risk factor to long term mortality of other classical prognostic factors such as age, FEV1, and BMI. 8 Thus, it was necessary to assess the risk factors to the occurrence of exacerbations. Over the past decade, although several studies inconsistently found a range of variables associated with exacerbations, because of their different definitions of exacerbation or different populations in the intervention studies, researchers widely recognized that the major determinant of frequent exacerbations was a history of exacerbation.6,21,22 Consistent with this view, we found that patients with exacerbations in the past year usually had more frequent exacerbations and hospital admissions in the future than those without exacerbation. The occurrence of exacerbations was the best predictor to future exacerbations.
Most of the studies identified predictors to the outcomes of COPD based on an observation at single time points, but few prospective studies were designed to explore the relationship between disease trajectory and future outcomes. 11 In our study, we recorded the short-term change of spirometry, CAT, mMRC, and exacerbation rate over 6 months, and then assessed the predictive value of these variables for future exacerbations. The results showed the short-term changes of FEV1, FEV1% predicted, and CAT scores were significantly different between patients with or without exacerbations in the subsequent year, while the baseline FEV1, FEV1% predicted, and CAT showed no difference between the two groups. A similar phenomenon existed on the univariate analysis of risk factors for future exacerbations. In addition, the OR of short-term exacerbations to predict future exacerbation is much higher than that of the history of exacerbation before study entry. All these results suggested that the disease progression possibly had important predictive value to outcomes of COPD at an individual level, which we usually ignored in clinical practice.
In stepwise multivariate logistic-regression analysis, we found that the occurrence of exacerbation and decrease of FEV1 were significantly associated with future exacerbations in patients with COPD. It was widely accepted that these two variables were risk factors to long-term outcomes of COPD.6,21–23 Patients with frequent exacerbations often had a faster and greater decline in FEV1, 23 and a change in FEV1 of above 100 mL might have an estimated 6.0% reduction in the chance to experience at least one exacerbation in the future. 24
Several multidimensional indices had been proposed to predict outcomes of COPD, such as BODE, ADO, and B-AE-D, but they were all established on a single time point. To our knowledge, the only one composite model using disease trajectory is the CID model, which was based on the post hoc analysis of the TORCH trial. 11 Until now, there were no prospective studies conducted to validate the predictive value of CID, though several studies had used this composite index as outcome or endpoint.12,13,25,26 To make the CID model more practical in clinical application, we replaced SGRQ with the CAT questionnaire, since CAT and the change of CAT had close correlation to SGRQ. 16 Then we assessed the predictive capacity of CID-C for future exacerbation. The results demonstrated that CID-C had a good prognostic prediction of future exacerbation with 83.3% in sensitivity and 55.7% in specificity.
Furthermore, in the multivariate logistic-regression analysis, the change of CAT was excluded from the model. Throughout all the multidimensional indices, neither SGRQ nor CAT had been included in the final model, even though they all appeared to have significant predictive value in univariate analysis.7–10 Thus, we also proposed the hypothesis that the Simplified CID, by removing CAT from the CID-C model, retained the predictive capacity for the occurrence of future exacerbations. Interestingly, the results showed that patients in Simplified CID status were more likely to suffer exacerbation in the future than patients in CID-C status. The comparison of ROC between the two models also demonstrated that simplified CID had slightly better prognostic prediction capacity than CID-C. These findings supported our hypothesis that removing CAT from the CID model would not limit the risk prediction. In fact, both CID-C and Simplified CID had significant prognostic prediction of future exacerbations in patients with COPD. Our results indicated that the patients who experienced exacerbations and a decline in FEV1 of above 100 mL in the short term were more likely to suffer exacerbations in the next year. Prevention of short-term clinical deterioration seemed to be an effective approach to decrease the risk of sustained deterioration in health status in COPD patients. The present study allowed us to establish a very simple COPD-specific composite index for easy use in clinical assessment to predict the risk of future exacerbations based on the disease trajectory.
Our study has potential limitations. First, we recruited a total of 127 patients in our study. The small population might limit the advance of this model. The majority of patients enrolled in our study were male, which is consistent with the fact that male patients with COPD are much more numerous than female in China. 27 Second, we established the Simplified CID in one cohort and lacked another cohort to validate our model. In a future study, we may recruit more patients to complete the validation. Finally, a longer follow-up period should be conducted in individual patients to assess the long-term outcomes. Our study is a continuous and on-going research, and the prediction of long-term outcomes of COPD will be achieved in the future.
Conclusion
In summary, our study revealed that disease trajectory, especially the short-term exacerbations, had significant predictive value for the occurrence of exacerbations in the following year. The short-term CID-C and Simplified CID both allow a simple and accurate assessment of risk for future exacerbations.
Supplemental Material
sj-pdf-1-tar-10.1177_1753466620977376 – Supplemental material for Modified and simplified clinically important deterioration: multidimensional indices of short-term disease trajectory to predict future exacerbations in patients with chronic obstructive pulmonary disease
Supplemental material, sj-pdf-1-tar-10.1177_1753466620977376 for Modified and simplified clinically important deterioration: multidimensional indices of short-term disease trajectory to predict future exacerbations in patients with chronic obstructive pulmonary disease by Yi-yang Zhao, Cong Liu, Yu-qin Zeng, Ai-yuan Zhou, Jia-xi Duan, Wei Cheng, Tian Sun, Xin Li, Li-bing Ma, Qi-mi Liu, Ying-qun Zhu, Ming Chen, Mei-ling Zhou and Ping Chen in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-2-tar-10.1177_1753466620977376 – Supplemental material for Modified and simplified clinically important deterioration: multidimensional indices of short-term disease trajectory to predict future exacerbations in patients with chronic obstructive pulmonary disease
Supplemental material, sj-pdf-2-tar-10.1177_1753466620977376 for Modified and simplified clinically important deterioration: multidimensional indices of short-term disease trajectory to predict future exacerbations in patients with chronic obstructive pulmonary disease by Yi-yang Zhao, Cong Liu, Yu-qin Zeng, Ai-yuan Zhou, Jia-xi Duan, Wei Cheng, Tian Sun, Xin Li, Li-bing Ma, Qi-mi Liu, Ying-qun Zhu, Ming Chen, Mei-ling Zhou and Ping Chen in Therapeutic Advances in Respiratory Disease
Supplemental Material
sj-pdf-3-tar-10.1177_1753466620977376 – Supplemental material for Modified and simplified clinically important deterioration: multidimensional indices of short-term disease trajectory to predict future exacerbations in patients with chronic obstructive pulmonary disease
Supplemental material, sj-pdf-3-tar-10.1177_1753466620977376 for Modified and simplified clinically important deterioration: multidimensional indices of short-term disease trajectory to predict future exacerbations in patients with chronic obstructive pulmonary disease by Yi-yang Zhao, Cong Liu, Yu-qin Zeng, Ai-yuan Zhou, Jia-xi Duan, Wei Cheng, Tian Sun, Xin Li, Li-bing Ma, Qi-mi Liu, Ying-qun Zhu, Ming Chen, Mei-ling Zhou and Ping Chen in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
Thanks to Ming-yan Jiang from Xiangtan Central Hospital, Ling-mei Huang from the First People’s Hospital of Yue-yang, Wei-min Feng from Hengyang Central Hospital and Yi Liu from Zhu-zhou Central Hospital, for their contribution to recruit patients with COPD in their own hospitals.
Author contributions
PC and YZ contributed to the study conceptualization; YZ, CL, QZ, AZ, JD, WC, TS, XL, LM, QL, YZ, MC and MZ performed the patients screening and collected the data of enrolled patients; YZ and CL contributed to data analysis; PC and YZ contributed to funding acquisition; YZ drafted the manuscript and all authors contributed to critically revising the manuscript for important intellectual content. All authors agree to be accountable for all aspects of the work. All authors read and approved the final manuscript.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation (NSFC) of China under Grant 81770046 and 81970044 to Ping Chen; Hunan Provincial Innovation Foundation For Postgraduate under Grant CX20190157 to Yi-yang Zhao.
Ethics approval and consent to participate
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.