
Abstract
Purpose:
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2018 recommendations support maintenance treatment with long-acting bronchodilators in most symptomatic patients with chronic obstructive pulmonary disease (COPD). While restricting the overuse of inhaled corticosteroids (ICS) may influence healthcare utilization required to treat inadvertent respiratory (exacerbations and pneumonia) and diabetes-related events, it may also change the total medication cost. This analysis was performed to estimate the 5-year budget impact of switching from ICS-containing treatment combinations to dual bronchodilation, in line with the recommendations.
Methods:
The model quantified the budget impact of treatment and healthcare resource utilization when COPD patients were anticipated to switch from ICS-containing treatments to dual bronchodilation. Three switch scenarios were calculated with increasing proportions of patients on dual long-acting bronchodilators, to the detriment of ICS-containing double and triple combinations. Clinical and cost input data were based on results from clinical trials and Greek and Portuguese healthcare cost databases.
Results:
Healthcare resource use to manage exacerbations, pneumonia and diabetes-related events were projected to increase between 2019 and 2023 in parallel with the growing COPD patient population and associated costs were estimated at 52–57% of the total disease cost in the Greek and Portuguese base case scenarios. Total cost savings between 21 and 112 million EUR were projected when the proportion of patients on double and triple ICS-containing treatments was gradually reduced to 50% in scenario A, 20% in scenario B and 7% in scenario C. Sensitivity analyses showed that none of the model assumptions had a major impact on the projected savings.
Conclusion:
The alignment of COPD treatment with current recommendations may bring clinical benefits to patients, without substantial cost increases and even cost savings for payers.
The reviews of this paper are available via the supplemental material section.
Introduction
Chronic obstructive pulmonary disease (COPD) is known to be associated with a significant clinical, social and economic burden, which usually needs to be addressed with limited health care funds.1–3
Worldwide prevalence rates of COPD are high and even expected to increase in the aging population, when more people will express the effects of continued exposure to the risk factors, that is, tobacco smoking and air pollution. 1 A systematic literature review of studies conducted between 1990 and 2014 estimated the prevalence of spirometry-diagnosed COPD at 12% of the European population aged 30 years or older. 1 This percentage increased by 22% between 1990 and 2010, which is substantial but slower than in the rest of the world, probably thanks to extensive public smoking cessation campaigns. 4 Although comparison between studies requires caution, data from Portugal found lower prevalence rates compared with other European countries, probably in relation to lower prevalence of smoking; Cardoso et al. found prevalence rates of 9% in 1995 and 5% in 2002 in individuals above 35 years of age. 5 COPD prevalence in Greece was estimated at 8% in the population older than 35 years with a smoking history of at least 100 cigarettes per lifetime. 6 Considering the high smoking degree per capita in Greece, these values are probably an under-estimation of the true prevalence with many patients remaining undiagnosed. 7
Pharmacological treatment aims at reducing symptoms on the one hand and reducing the risk of inadvertent events (e.g. exacerbations) on the other hand to improve patients’ general health status and exercise tolerance. Guidelines for the pharmacological treatment of COPD have gradually evolved over the past decades. Recently, the update of the Global Initiative for Chronic Obstructive Lung Disease (GOLD 2019) recommendations have confirmed the central role of long-acting bronchodilators (LAMA, long-acting antimuscarinics and LABA, long-acting β2-agonists) in the management of stable COPD. 1 While patients may be started on single or dual long-acting bronchodilator therapy, dual bronchodilator treatment is advised if dyspnoea or exercise limitation persist. 1 The use of inhaled corticosteroids (ICS) has been associated with side effects such as pneumonia and, therefore, careful consideration of risks/benefits is required if ICS-containing treatments are prescribed as initial therapy in COPD. 1 Today, the combination of ICS and LABA is considered an appropriate starting treatment in selected patients only, that is, patients with a history of asthma or symptomatic patients who have frequent exacerbations (GOLD classification category D) and high blood eosinophil counts (⩾300 cells/µl). 1 The ‘follow-up’ pharmacological management of COPD includes ICS-containing regimens if patients have further exacerbations despite appropriate treatment with dual long-acting bronchodilators. 1 In these patients, low blood eosinophil counts (<100 cells/µl) may predict a low likelihood of a beneficial response to ICS treatment. 1
Over the years, the uptake of the COPD treatment recommendations into clinical practice has been particularly slow despite significant educational efforts.8,9 ICS continue to be inappropriately prescribed in COPD outside the recommended indications. 10 Such inconsistent implementation of clinical recommendations, however, may induce unnecessary risks and associated costs for patients and health service payers.11–14
The global economic crisis in the last years has severely affected many European countries such as Greece and Portugal. The broader socioeconomic effects of the crisis such as rising unemployment, income reduction, increased out-of-pocket spending (through coinsurance and shared payments) and retrenchment of welfare support were more pronounced in the most affected countries, which had also instituted stringent austerity measures (e.g. Greece, Spain, Ireland and Portugal). 15
Our study is a budget impact analysis (BIA) that quantifies the 5-year economic impact of changes in treatment and healthcare resource utilization related to clinical respiratory events (exacerbations and pneumonias) and diabetes, when patients on ICS-containing treatment regimens are switched to dual bronchodilation, according to current recommendations for the maintenance treatment of COPD according to the current and possible future scenarios, from the perspective of the Greek and Portuguese health care systems.
Material and methods
Model design
This BIA was undertaken in accordance with the Good Practice principles of the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) to estimate the clinical and economic impact of an anticipated change in prescription patterns from ICS-containing medication towards dual bronchodilator treatment in patients taking COPD maintenance treatment. 16 The annual, multi-cohort, transition model was parameterized to include COPD local data from two different health care systems from Greece and Portugal. The model tracked the progression of the 2019 prevalent COPD population and added a new cohort of incident patients. Changes in resource usage were based on reported differences in the risk profile of COPD maintenance therapies, regarding the occurrence of treatment-related respiratory adverse events, which include moderate and severe exacerbations, pneumonia and diabetes-related events.
The time horizon was 5 years, ranging from 2019 to 2023. No discounting was applied. The consideration of direct health care costs for medication, hospitalization, emergency room and ambulatory visits was viewed from the perspective of the national health service. Impact on indirect costs (e.g. work productivity losses) was not considered in the model. The model calculated different scenarios related to the consumption of resources for COPD treatment and for the management of exacerbations and pneumonia.
Patient population
In the model, the studied patient population consisted of patients with COPD (GOLD categories B to D) on pharmacological maintenance treatment with long-acting bronchodilator(s), with or without an ICS component. GOLD A patients were excluded from the analysis since there is no recommendations for ICS in this population, treatment can be either a short- or long-acting bronchodilator and the choice of treatment depends on the effect of breathlessness. 1 The size and growth of the Greek and Portuguese COPD population on maintenance treatment was taken from the literature.6,7,17–19 COPD-related mortality was taken into consideration.
Intervention mix
The most commonly prescribed maintenance treatments in COPD were integrated in the model. These include LAMA mono-treatment, LAMA and LABA dual bronchodilator treatment, LABA and ICS combination treatment and triple combinations of LAMA, LABA and ICS. The current COPD treatment mix (base case) in Greece was estimated to be of 40% for triple combinations (LAMA/LABA/ICS), 35% for LABA/ICS, 15% for LAMA/LABA and finally 10% for LAMA based on published literature and adjusted with market forecast research (Boehringer Ingelheim, data on file).20,21 In Portugal, current patient shares per therapeutic class were estimated to be 41% LABA/ICS, 27% LAMA/LABA/ICS, 17% LAMA and 15% LAMA/LABA based on published literature and market forecast research (Boehringer Ingelheim, data on file). 17
To examine the impact of evolving treatment strategies, three hypothetical scenarios were considered (Table 1). Scenario A reflects a partial switch of patients on ICS-containing regimes to the LAMA/LABA treatment. In scenario B the LAMA/LABA/ICS patient segment represents 15%, while the LABA/ICS segment is reduced to 5%. This scenario mimics the GOLD 2018 recommendations, where ICS are reserved for patients with high (>300 cells/mm3) eosinophil counts, estimated at around 20% of the COPD population.1,22 Finally, more drastic increases of LAMA/LABA patient shares and decreases of ICS-containing regimes are considered in scenario C. In all scenarios, the market share of LAMA mono-treatment regimen was considered to be always 14%.
Current patient share by treatment regimen and evaluated alternative scenarios for future treatment mix.

ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting antimuscarinic drug.
Clinical input
In line with the main differences between the risk profiles of COPD maintenance therapies, the clinical outcomes of interest or inadvertent events, considered in our model were moderate and severe exacerbations, pneumonia and diabetes-related events. 1 The baseline exacerbation risk was altered according to the relative risk of exacerbation associated with prior exacerbation history (relative to no prior exacerbations) and treatment choice (relative to LAMA/LABA). The model assumed that exacerbation history had the same impact on the risk for moderate as for severe exacerbations, and that the proportion of moderate versus severe exacerbations was equal across treatment regimens. It was assumed that, at baseline, 53% of patients had no exacerbations, 25% of patients had one exacerbation and 22% of patients had two or more exacerbations for all treatments. 23 Table 2 summarizes the assumptions that were made regarding the inadvertent events used in the model.
Assumptions concerning the risk of moderate and severe exacerbations, pneumonia and diabetes-related events.

COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting antimuscarinic drug.
Exacerbations
Baseline exacerbation risk (for both moderate and severe exacerbations) was estimated for a population with no prior exacerbations and receiving LAMA/LABA. In the absence of data in a population with no prior exacerbations, the GOLD 2 population was used as a proxy for this patient subgroup. In the TONADO trial, the absolute annual exacerbation risk was of 39% for GOLD 1 and 2 (forced expiratory volume (FEV1) ⩾50% predicted) patients. 24 The distribution of moderate and severe exacerbations was determined using the TONADO trial. In the analysis by Derom et al., in patients experiencing an exacerbation, 15% and 85% were severe and moderate, respectively. 25 Consequently, this resulted in an annual absolute risk of 33% for moderate and 6% for severe exacerbations for GOLD 2 patients not using ICS and with <2 prior exacerbations.
The relative risk of LAMA versus LAMA/LABA was calculated based on the DYNAGITO study, 29 of LABA/ICS based on the FLAME study 28 and of LAMA/LABA/ICS using the data from the WISDOM study.30,31
Pneumonia
As the use of ICS is associated with a higher incidence of pneumonia events, a pneumonia rate of 4.7% was used for non-ICS and 7.4% for ICS treated patients. 32 Using data from a retrospective study of US claims database, 28% of pneumonia cases were considered to require hospitalization while in all other cases outpatient care was sufficient. 37
Diabetes-related events
Some evidence suggests that the use of ICS is associated with higher incidence of diabetes-related hospitalizations. 36 Estimates for ICS-associated diabetes hospitalizations and costs were derived from a cohort study of COPD patients with comorbid type II diabetes. 36 The model used an annual risk of diabetes-related hospitalization of 4.5% versus 6.0% and an annual risk of progression to insulin of 2.0% versus 4.7% in the non-ICS patients and in ICS patients, respectively. 36
Cost input
All input data used for cost calculations were derived from national literature and expressed in Euros (Table 3). When necessary, costs were inflated to 2019 Euros.
Baseline cost parameters.
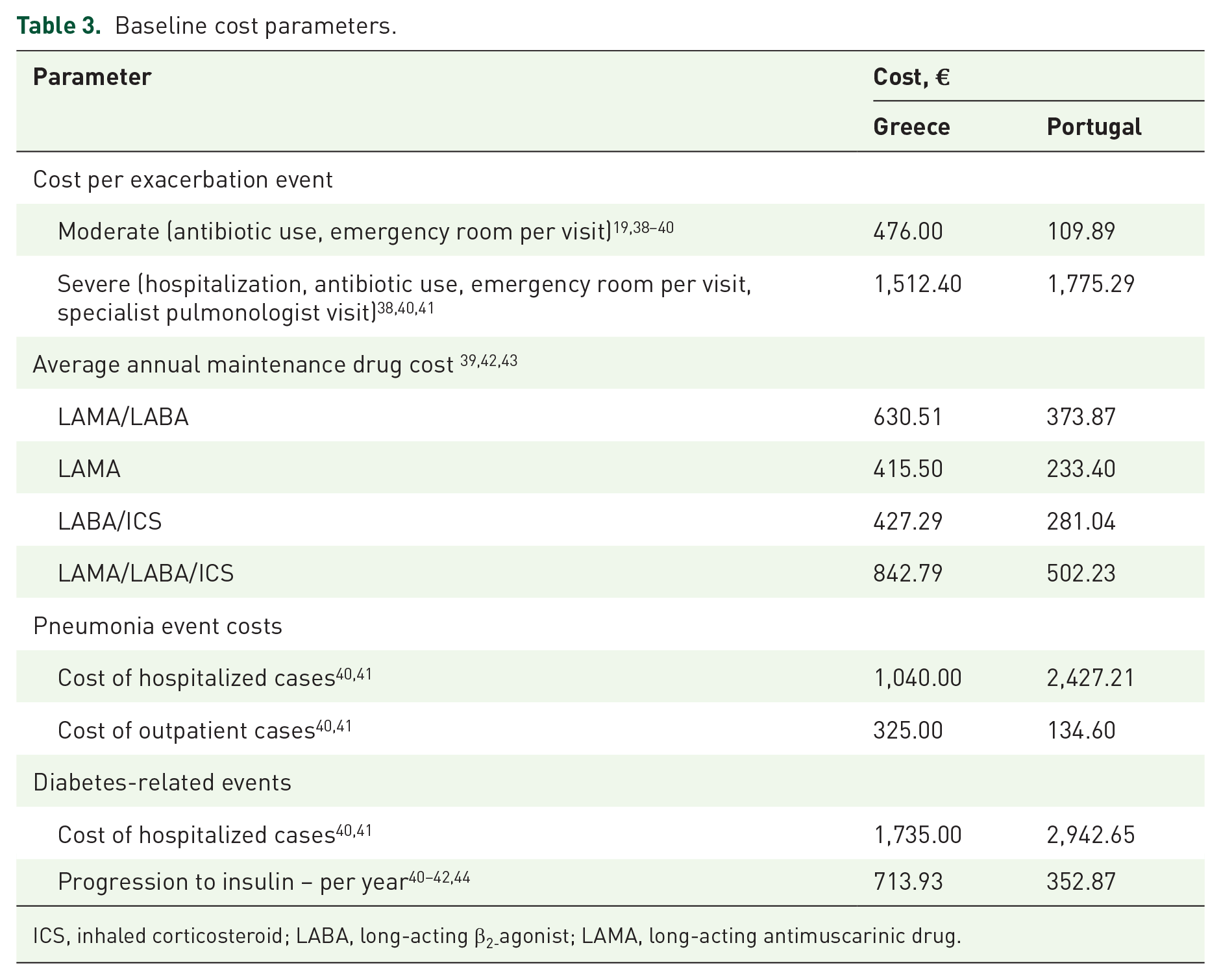
ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting antimuscarinic drug.
Sensitivity analyses
In order to assess the robustness of the model, one-way deterministic sensitivity analyses were conducted. Different model assumptions were tested, including the treatment cost (± 20%), cost of health resources used to manage exacerbations (± 20%) or pneumonia (± 20%), the exacerbation risk [alternative risk 1 (LAMA: 1.08; LAMA/LABA: 1.00; LABA/ICS: 1.22; LAMA/LABA/ICS: 0.86) and risk 2 (LAMA: 1.11; LAMA/LABA: 1.00; LABA/ICS: 1.15; LAMA/LABA/ICS: 0.87) based on published network metanalyses], the pneumonia risk (± 2.5%) and the percentage of patients with pneumonia requiring hospitalization to manage pneumonia (± 1/3).45,46
Results
Population
The number of COPD patients on maintenance therapy in 2019 was estimated at 260,925 in Greece and 132,340 in Portugal. Considering an annual growth of 4.4%, this number is projected to increase to 309,612 in 2023 in Greece. In Portugal, with an estimated annual growth 2.9%, the total number of COPD patients on maintenance therapy will rise to 148,439 in 2023.
Clinical and cost outcomes
The model, presented in Tables 4 and 5, shows that switching from ICS-containing regimens to dual bronchodilation will lead to cost savings in the Greek and Portuguese healthcare system, mainly by reducing the resources needed to treat inadvertent events.
5-year clinical and budget impact of alternative scenarios of treatment strategies (Greece).

k€: thousands €
5-year clinical and budget impact of alternative scenarios of treatment strategies (Portugal).
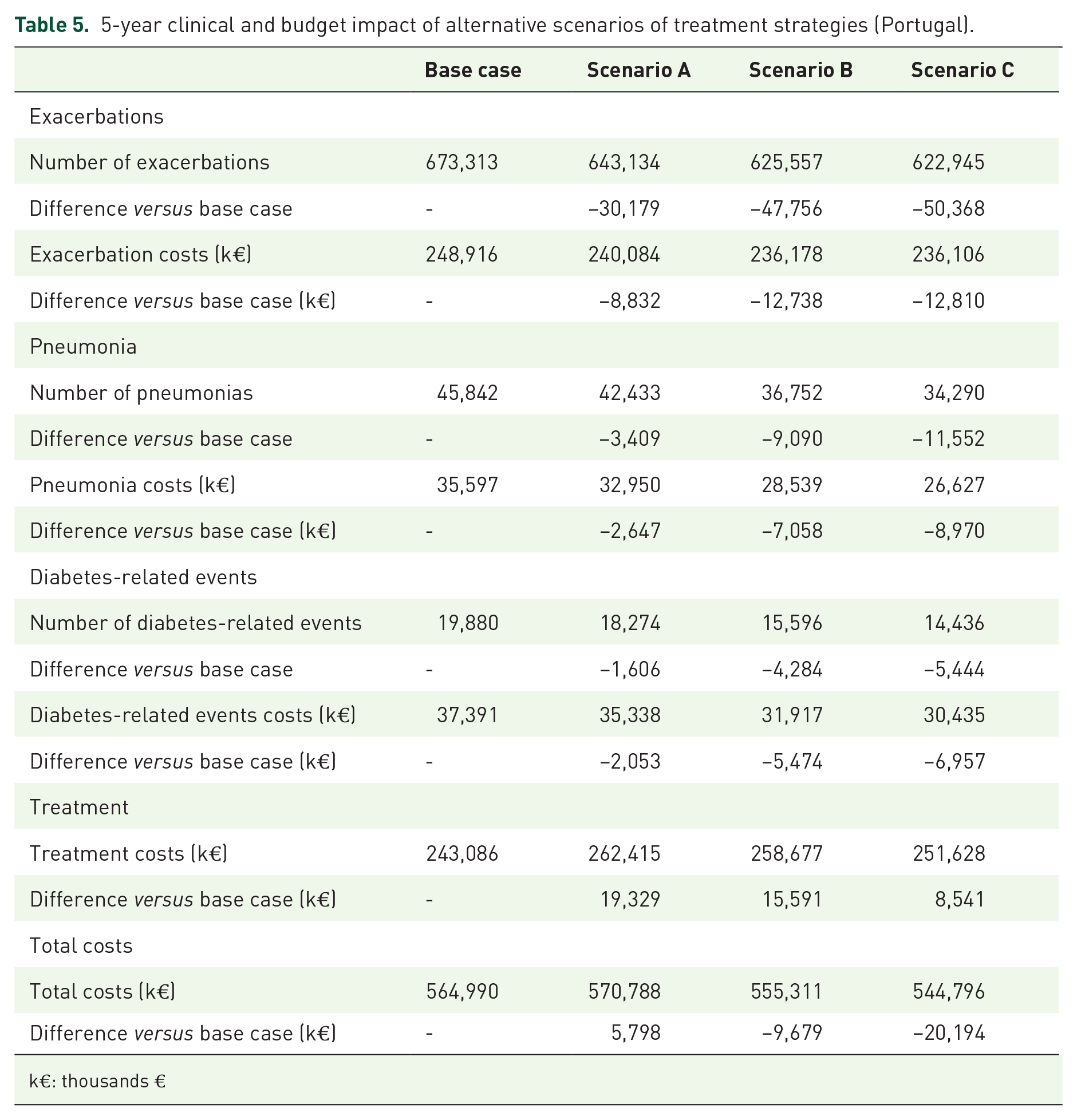
k€: thousands €
Base case
If the current therapeutic approach is left unaltered (base case), the associated number of moderate and severe exacerbations of COPD is projected to reach a total number of 1,335,806 exacerbations over the 5-year period (Table 4). Similarly, the number of moderate and severe exacerbations will amount to 673,313 cases over the period of 5 years in Portugal (Table 5) rising from 127,047 exacerbations in 2019 to 142,501 exacerbations. The related total cost to treat these exacerbations in the base over the 5-year period is calculated to be approximately 850 million Euro in Greece and 250 million Euro in Portugal (Tables 4 and 5). In parallel, the base case expects the number of pneumonia events to increase from 17,547 to 20,821 in Greece and from 8,650 to 9,702 in Portugal, representing more than 140,000 pneumonia events in total for both countries over 5 years, with an associated management cost estimated at more than 85 million Euro. Also in the base case, the number of diabetes-related hospitalizations amounts to 56,330 and 19,980 in Greece and Portugal, respectively, which corresponds with a total treatment cost over 111 million Euro in 5 years of time. COPD treatment costs are estimated to represent between 47.6% and 43.0% of the cost of the disease, which also includes cost of inadvertent event management, in Greece and Portugal, respectively.
Scenario A
Switching from base case to scenario A avoids 60,461 exacerbations, 13,019 cases of pneumonia and 7,735 diabetes-related events during the 5-year period for both countries taken together. On the other hand, the cost of COPD treatment increases by 0.1% in Greece and 8.0% in Portugal. In scenario A, the total cost of the disease equates to 1,835 million Euro in Greece and 571 million Euro in Portugal, which represents savings of 1.5% and 1.0% for the respective countries compared with the base case.
Scenario B
Switching from base case to scenario B avoids almost twice as many exacerbations (113,717 in total), 30,223 cases of pneumonia and 17,768 diabetes-related events during the 5-year period for both countries. This is in parallel with a 0.1% decrease in the cost of COPD treatment in Greece and an increase of 6.4% in Portugal. In scenario B, the total cost of the disease equates to 1,800 million Euro in Greece and 555 million Euro in Portugal, which represents savings of 3.4% and 1.7% for the respective countries compared with the base case.
Scenario C
Finally, scenario C compared with base case avoids 121,632 exacerbations, 37,692 cases of pneumonia and 22,115 diabetes-related events during the 5-year period for both countries taken together, while the cost of COPD treatment decreases by 2.5% in Greece and increases by 3.5% in Portugal. This scenario brings the total cost of the disease to 1,770 million Euro in Greece and 545 million Euro in Portugal, offering a cost saving of 5.0% and 3.6% versus base case in Greece and Portugal, respectively.
Sensitivity analyses
The results of the sensitivity analyses are shown in Figure 1. None of the tested scenarios had a major impact on the projected savings. The highest effect was seen when exacerbation risk and cost varied; treatment cost had a low impact.

5-year budget impact of alternative scenarios of treatment strategies with different sensitivity analyses (data pooled Greece and Portugal).
Discussion
The COPD patient population is expected to grow steadily from 2019 to 2023, which inherently leads to more patients being treated but also more exacerbations and inadvertent events being managed. 47 Our analysis was performed to better understand the 5-year budget impact on Greek and Portuguese healthcare systems, if COPD maintenance treatment would become better aligned with the current GOLD recommendations. 1 The misalignment with treatment guidelines, particularly the persistent overuse of ICS-containing treatment regimens in COPD patients without appropriate indication, has been extensively discussed elsewhere.13,14,48 It is now well accepted that in COPD, ICS should be restricted to a small group patients with a positive risk/benefit ratio for ICS (e.g. patients with a history of asthma, patients with exacerbations despite optimal bronchodilation). 1 Consequently, there is also increasing interest in ICS withdrawal studies and practical advice on how to implement the switch from current treatment schedules in daily practice.30,49–51 The cost implications of optimization of care are becoming more and more important.
In the current model, the use of long-acting dual bronchodilator medication (LAMA/LABA) was projected to increase from being used in 15% of COPD patients to 36% (scenario A), 66% (scenario B) and 79% of patients (scenario C). This switch would happen at the expense of ICS-containing treatments (either LABA/ICS or LAMA/LABA/ICS combinations). On top of pharmaceutical treatment costs, the model estimated changes in healthcare resource usage, such as moderate and severe exacerbations and pneumonia, including those requiring hospital admission and progression and/or hospitalization of patients with diabetic comorbidity.
Estimations of future exacerbations took into consideration differences in patient’s baseline exacerbation risk, depending on prior exacerbation history as in the ECLIPSE study, as well as the type of treatment regimen. 27 Relative efficacies of COPD maintenance treatments (LAMA, LABA/ICS, LAMA/LABA and LAMA/LABA/ICS) to prevent exacerbations were calculated from large COPD studies, FLAME, DYNAGITO and WISDOM.28–30 Annual rates of pneumonia with ICS- versus non-ICS containing treatments were taken from the meta-analysis of Singh et al. 32 Moreover, it was assumed that one in three pneumonia cases would require hospitalization. 33 By using different studies to assess the impact of different scenarios on pneumonia and exacerbations, and considering the potential lack of differentiation between both events, it is possible that our analysis double counted events and therefore overestimated the cost benefits of the switch to LAMA/LABA.
We also integrated into the model the evidence of Price’s cohort study, showing that COPD patients with type II diabetes had a higher risk of progression to insulin use and hospitalization when using ICS. 36 In that study, there was no description on the reason for hospitalization so we used the tariff of a diabetes-related hospitalization in our cost analysis. In clinical practice, it is possible that such hospitalizations are coded with a different primary cause for admission, which would lead to a different cost of the disease. In our analysis, changing the cost of diabetes-related hospitalization would not change the direction of the results.
Overall, the model predicted that the healthcare resources needed to manage moderate and severe exacerbations, pneumonias and progression or hospitalization of diabetic patients would consume more than 50% of the total disease cost. However, these inadvertent events were projected to occur less frequently with decreasing proportions of patients taking ICS-containing treatments from scenario A to C. While in Greece the switch of ICS-containing regimen patients to LAMA/LABA would lead to savings due to less inadvertent events and less treatment costs, the results for Portugal lead to increase in pharmaceutical expenditure that is largely compensated with the decrease in inadvertent events and their relative costs. In the most drastic scenario (scenario C), the savings obtained with the withdrawal of ICS in COPD patients correspond to an extra 29,300 Greek patients and 10,800 Portuguese patients who could be treated.
The sensitivity analysis showed that the model was robust. Compared with the base case, reducing ICS use was cost-saving in all scenarios. However, the model also has its limitations. First, diagnosis of COPD patients is often delayed and, therefore, the number of patients on maintenance treatment may be underestimated, particularly in the less severe groups. Second, the baseline exacerbation risk and treatment shares were taken from the literature and may be slightly outdated. Finally, while comparing ICS and non-ICS containing treatments, this model largely focused on ICS-related avoidable adverse events.
This budget impact model, applied to the Greek and Portuguese health systems, demonstrated that reducing inappropriate use of ICS in COPD patients, according to the guidelines, not only has a positive impact on clinical outcomes, but may equally provide cost savings to the payers. Therefore, not only clinical but also cost considerations underline the need for better adherence to the guidelines.
Conclusions
The GOLD 2018 recommendations support LAMA/LABA dual bronchodilation treatment in most symptomatic COPD patients. Our budget impact model shows that the switch from ICS-containing regimens to LAMA/LABA, while reducing the number of COPD exacerbations, pneumonias and diabetes-related events, provides cost savings to both the Portuguese and Greek national health systems. In two countries where the financial crisis put much pressure on healthcare expenditure, aligning COPD treatment with the current recommendations is thus not only beneficial for patients’ clinical outcomes, but also constitutes a critical cost saving strategy for payers.
Supplemental Material
Author_Response_1 – Supplemental material for The cost-saving switch from inhaled corticosteroid-containing treatments to dual bronchodilation: a two-country projection of epidemiological and economic burden in chronic obstructive pulmonary disease
Supplemental material, Author_Response_1 for The cost-saving switch from inhaled corticosteroid-containing treatments to dual bronchodilation: a two-country projection of epidemiological and economic burden in chronic obstructive pulmonary disease by Kyriakos Souliotis, Luís Silva Miguel, Georgios Hillas, Margarida Borges, Giannis Papageorgiou, Diogo Viana, Joao Malhadeiro and Stéphane Soulard in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1 – Supplemental material for The cost-saving switch from inhaled corticosteroid-containing treatments to dual bronchodilation: a two-country projection of epidemiological and economic burden in chronic obstructive pulmonary disease
Supplemental material, Reviewer_2_v.1 for The cost-saving switch from inhaled corticosteroid-containing treatments to dual bronchodilation: a two-country projection of epidemiological and economic burden in chronic obstructive pulmonary disease by Kyriakos Souliotis, Luís Silva Miguel, Georgios Hillas, Margarida Borges, Giannis Papageorgiou, Diogo Viana, Joao Malhadeiro and Stéphane Soulard in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
Medical writing assistance was provided by Hedwig Stals of HD Consultancy. James Harris, Ian Koblbauer and Eddie Gibson from Wickenstones ltd supported with the calculations.
Author contribution(s)
Conflict of interest statement
KS, LSM, GH and MB received grants from Boehringer Ingelheim. GP, DV, JM and SS are employed by Boehringer Ingelheim.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Boehringer Ingelheim.
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.