
Abstract
Background:
Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is a widely used, safe, and accurate technique for obtaining pathological specimens to be used in the diagnosis of diseases involving lung hilar and mediastinal lymph node (LN) enlargement. However, application of the suction technique during EBUS-TBNA remains controversial. In addition, the effectiveness of the slow-pull capillary technique for the diagnosis of pancreatic masses was recently reported. The aim of this study was to compare the diagnostic accuracy of EBUS-TBNA using these two techniques.
Methods:
The accuracy, sensitivity, specificity, negative predictive value (NPV), positive predictive value (PPV), and availability of tissue cores of the suction and slow-pull capillary techniques were studied retrospectively in patients who underwent EBUS-TBNA for the diagnosis of diseases involving lung hilar and mediastinal LN enlargement.
Results:
A total of 97 patients with hilar and mediastinal LN enlargement underwent EBUS-TBNA; 30 patients underwent the suction technique, 56 patients underwent the slow-pull capillary technique, 5 patients underwent both techniques, and 6 patients had failed operations. The accuracy, sensitivity, specificity, NPV, PPV, and the number of tissue cores obtained with the suction and slow-pull capillary techniques were 66.67% versus 85.71% (p = 0.039), 43.75% versus 85.42% (p < 0.001), 92.86% versus 87.5% (p > 0.05), 59.09% versus 50% (p > 0.05), 87.5% versus 97.62% (p > 0.05), and 19 versus 50 (p = 0.004), respectively. In both univariate and multivariate analyses, the acquisition of tissue core was significantly associated with the diagnostic accuracy of EBUS-TBNA. Moreover, the slow-pull capillary technique was significantly associated with the acquisition of tissue core in EBUS-TBNA. There were no significant differences between the two groups in the blood contamination of samples.
Conclusions:
Use of the slow-pull capillary technique in EBUS-TBNA can significantly increase the accuracy related to the diagnosis of diseases involving hilar and mediastinal LN enlargement by improving the acquisition of tissue core.
The reviews of this paper are available via the supplemental material section.
Keywords
Introduction
Lung hilar and mediastinal lymph node (LN) enlargement is frequently involved in lung cancer, mediastinal tumors, tuberculosis, and sarcoidosis. Biopsy of the enlarged hilar and mediastinal LNs is necessary for the diagnosis of these diseases. Real-time ultrasound-guided bronchoscopy, termed endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA), was first applied in clinical practice in 2002. 1 This technique allows the enlarged hilar and mediastinal LNs to be visualized in real time, and measures the size of LNs during bronchoscopy, which can be used to guide TBNA. Currently, it is a widely used, safe, and accurate technique for obtaining a pathological specimen from hilar and mediastinal LNs.2–5 It exhibits a diagnostic yield similar to that of surgical mediastinoscopy; however, it is associated with a lower complication rate. 6 The LNs that can be punctured using EBUS-TBNA are at stations 2R, 2L, 4R, 4L, 7, 10R, 10L, 11R, 11L, 12R, and 12L. 7 EBUS-TBNA has improved the results of diagnostic sampling when attempting to diagnose hilar and mediastinal diseases, especially for lung tumors, sarcoidosis, and tuberculosis.8,9 However, Muthu and colleagues reported that, among 151 patients with clinically suspected sarcoidosis, there was no difference in the diagnostic yield of EBUS-TBNA (which is the proportion of patients in whom the technique yielded a definitive diagnosis out of the total number of patients who underwent the technique) between different sizes of aspiration needles. 10 Of note, the diagnostic yield of EBUS-TBNA is the proportion of patients in whom the technique yielded a definitive diagnosis. Nevertheless, the EBUS-TBNA technique requires further optimization.
In general, EBUS-TBNA sampling is performed under negative pressure created by suction, which is produced by applying a syringe to the needle. 11 However, the application of suction during EBUS-TBNA has been controversial. 12 Use of negative pressure created by suction during EBUS-TBNA allows the collection of large cytological samples. 13 However, a comparison of the samples obtained through endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) in LNs with and without suction showed that the quality of the samples without suction was significantly better owing to the lower rate of blood contamination. 14 In line with this, some clinicians suggest that suction may increase tissue damage at the biopsy site, leading to more bleeding and poorer specimen quality, and thereby reducing the diagnostic accuracy of EBUS-TBNA. A randomized controlled study investigated the effects of different EBUS-TBNA techniques (i.e. suction plus a stylet, suction only, and stylet only) on the diagnostic yield. The results did not reveal significant differences among the techniques. 15 Therefore, we explored the availability of another technique for use during EBUS-TBNA that could improve the quality of specimens and increase the diagnostic accuracy.
One alternative to the suction technique is the slow-pull capillary technique, which involves a minimal suction force. Nakai and colleagues reported that, among 97 EUS-FNA procedures for 93 patients with pancreatic solid lesions, the slow-pull capillary technique was associated with less blood contamination and better diagnostic yield than the suction technique. 16 Lee and colleagues also found that the slow-pull capillary technique had a higher diagnostic yield than the suction technique in pancreatic disease. 17 Although the slow-pull capillary technique is increasingly being used for the diagnosis of digestive diseases, there is currently no evidence regarding its use in respiratory diseases. Therefore, the aim of this study was to compare the diagnostic accuracy of EBUS-TBNA using the suction technique and the slow-pull capillary technique.
Methods
Patients
Consecutive patients with hilar and mediastinal LN enlargement who underwent EBUS-TBNA between January 2016 and November 2018 at the Beijing Friendship Hospital, Capital Medical University (Beijing, China) were studied retrospectively. Inclusion criteria were: age 18–80 years; chest computed tomography showing hilar or mediastinal LN enlargement; no contraindications for bronchoscopy; and signed informed consent provided by the patient. Exclusion criteria were: severe coagulation dysfunction; severe cardiopulmonary dysfunction; acute asthma attack or massive haemoptysis; poor general condition and physical weakness without tolerance for anaesthesia or allergy to narcotic drugs; use of both suction and slow-pull capillary techniques; failure of the EBUS-TBNA procedure; incomplete patient information; and lack of signed informed consent.
LN stations were classified in accordance with the LN map produced by the International Association for the Study of Lung Cancer. 18 We evaluated patient characteristics, including demographic information, complications, and final cytological and histological diagnoses.
This study was approved by the ethics committee of Beijing Friendship Hospital (2018-P2-150-02). The patient enrolment process is shown in Figure 1.
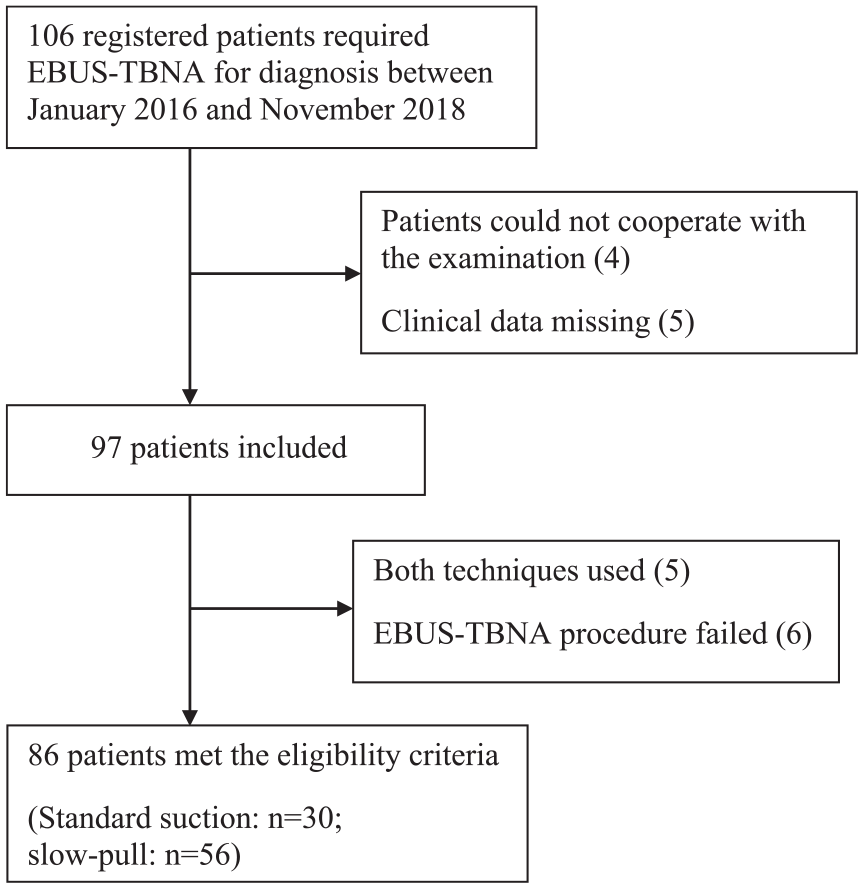
Flow chart of patient enrolment.
EBUS-TBNA procedure
In all patients, the EBUS-TBNA operations were performed by the same experienced endoscopic physician. All patients received topical anaesthesia (lidocaine 2%), while their vital signs and arterial oxygen saturation were monitored continuously during the whole operation. EBUS-TBNA was performed using an EBUS device (BF-UC260FW; Olympus Ltd., Tokyo, Japan). Following the detection of an enlarged LN or peribronchial mass by EBUS, color doppler ultrasound was used to determine the optimal biopsy site. The diameters of both the long and short axes of the LN or peribronchial mass were measured and recorded.
The TBNA biopsies were performed using a special 22-gauge needle (ECHO-HD-22-EBUS-O; Cook Ireland Ltd., Limerick, Ireland). The suction technique was performed as follows: after identification and measurement of the target, a needle was used to puncture the LN or peribronchial mass. Immediately after puncture, the stylet was pushed onto the target to reduce the presence of tracheobronchial cells in the specimen. Subsequently, it was completely removed, and a 10-ml negative pressure vacuum syringe was applied. The needle was fanned through the target LN or peribronchial mass, and to-and-fro movements were performed ⩾20 times under continuous doppler ultrasonic monitoring. The slow-pull capillary technique was performed as follows: after identification and measurement of the target, a needle was used to puncture the LN or peribronchial mass with the stylet in place. Immediately after puncture, the stylet was pushed onto the target to reduce the presence of tracheobronchial cells in the specimen. Subsequently, the needle was fanned through the target LN or peribronchial mass, and ⩾20 to-and-fro movements were performed under continuous doppler ultrasonic monitoring. At the same time, the stylet was slowly and continuously pulled to create weak negative pressure. Each LN or peribronchial mass was subjected to ⩾2–3 needle passes to ensure the effectiveness of the puncture technique and quality of puncture specimens (based on rapid-on-site evaluation performed by a pathologist). 19 After each puncture, the stylet was reinserted to push the contents out.
Pathological evaluation of samples
The samples acquired using the suction and slow-pull capillary techniques were processed for cytological and histological evaluation. Tissue cores were immersed in formalin solution and subjected to histopathological examination. In the absence of a tissue core, the contents were pressed onto a glass slide, immersed in 96% methanol for ⩾10 min and subjected to cytopathological examination. Rapid on-site evaluation was performed. All samples were assessed histologically for blood contamination. Blood contamination was categorized as follows: low (no or few blood cells influencing the diagnosis), moderate (sample partially obscured by blood cells, but pathological diagnosis possible), and high (large numbers of blood cells, rendering pathological diagnosis difficult). 20 All pathological diagnoses were reached by pathologists at the Beijing Friendship Hospital, Capital Medical University, Beijing, China.
Diagnosis gold standard
The final pathological diagnosis was based on all available cytological and histological samples. In cases with negative pathological results (i.e. no diagnosis of specific disease), we aimed to follow up the patients for ⩾6 months.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics software version 20.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation. A t test was used to compare continuous data. Pearson’s Chi-square or Fisher’s exact test were used to compare count data. Univariate and multivariate logistic regression analyses were performed to evaluate the diagnostic accuracy and acquisition of tissue core of the two techniques. The potential predictors comprised the long-axis diameter of the LN or mass (<30 mm versus ⩾30 mm), short-axis diameter of the LN or mass (<15 mm versus ⩾15 mm), EBUS-TBNA technique (suction versus slow-pull capillary capillary), acquisition of tissue core, and the final pathology (benign versus malignant result). A p value < 0.05 in a two-tailed test indicated a statistically significant difference.
Results
A total of 106 registered patients required EBUS-TBNA for diagnosis between January 2016 and November 2018. Of those, four patients could not undergo the examination due to severe cough, and five had missing clinical data. A total of 97 patients were included in the study. Among those, 30 patients underwent EBUS-TBNA with the suction technique, 56 patients underwent EBUS-TBNA with the slow-pull capillary technique, 5 patients underwent both the suction and slow-pull capillary techniques, and 6 patients had failed operations. The flow chart for patient enrolment is shown in Figure 1. We observed the patients 48 h after EBUS-TBNA, and there were no serious complications recorded in the two groups. The baseline characteristics of the patients and the final diagnoses are summarized in Table 1. There were no significant differences in age, height, or weight between the two groups. The final diagnosis was malignant tumor for 45 patients (52.3%; suction versus slow-pull, 6 versus 39, respectively), nonspecific inflammation for 20 patients (23.3%; suction versus slow-pull, 13 versus 7, respectively), sarcoidosis for 16 patients (18.6%; suction versus slow-pull, 9 versus 7, respectively), tuberculosis for 3 patients (3.5%; suction versus slow-pull, 1 versus 2, respectively), hemophagocytic syndrome for 1 patient (1.2%; suction versus slow-pull, 1 versus 0, respectively), and cryptogenic organizing pneumonia for 1 patient (1.2%; suction versus slow-pull, 0 versus 1, respectively).
General characteristics of the included patients.

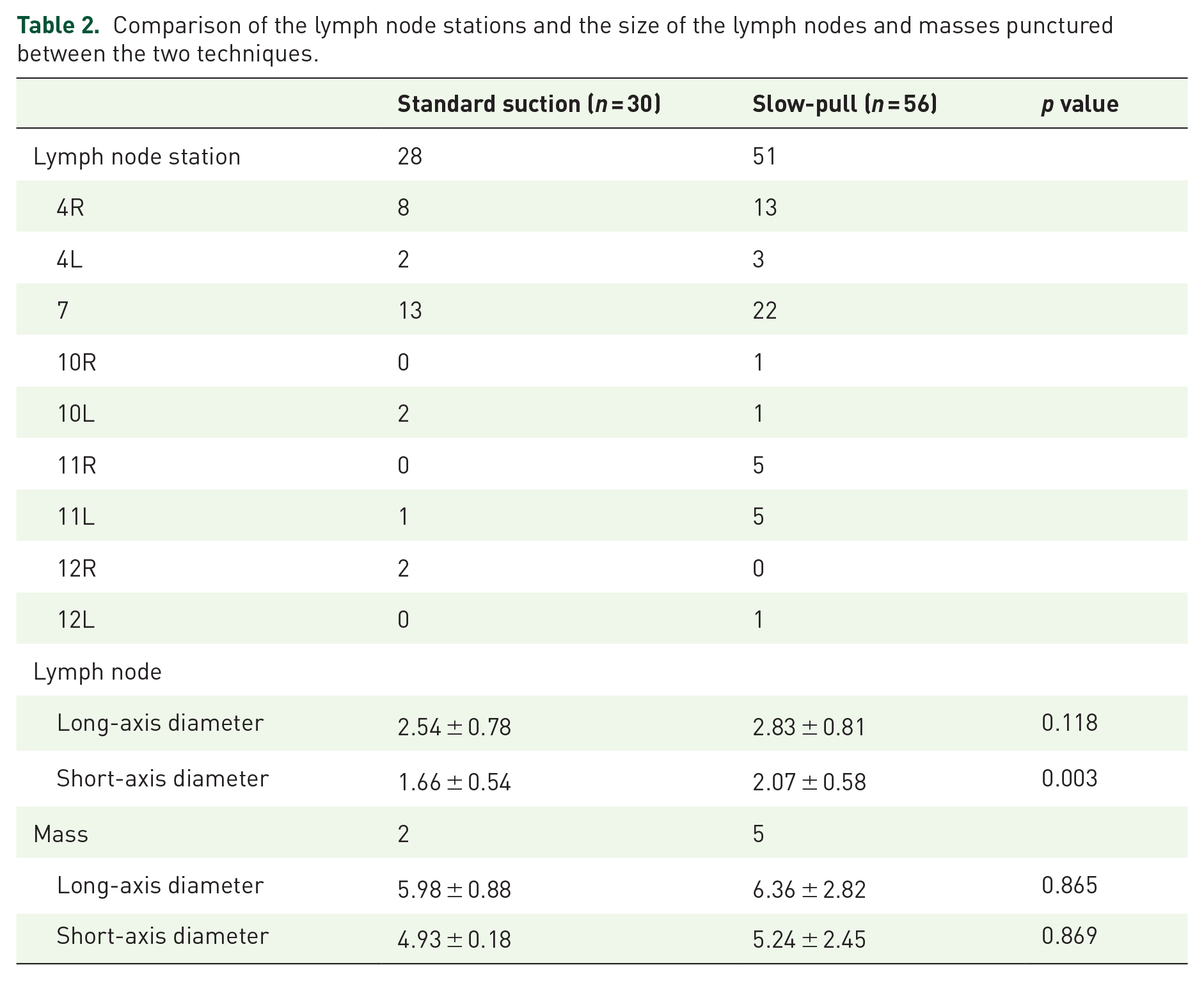
In total, 79 LNs (suction versus slow-pull, 28 versus 51, respectively) and seven peribronchial masses (suction versus slow-pull, 2 versus 5, respectively) were punctured; 21 were at station 4R (suction versus slow-pull, 8 versus 13, respectively), 5 were at station 4L (suction versus slow-pull, 2 versus 3, respectively), 35 were at station 7 (suction versus slow-pull, 13 versus 22, respectively), 1 was at station 10R (suction versus slow-pull, 0 versus 1), 3 were at station 10L (suction versus slow-pull, 2 versus 1, respectively), 5 were at station 11R (suction versus slow-pull, 0 versus 5, respectively6 six were at station 11L (suction versus slow-pull, 1 versus 5, respectively), 2 were at station 12R (suction versus slow-pull, 2 versus 0, respectively), and 1 was at station 12L (suction versus slow-pull, 0 versus 1, respectively). The LN sizes in the suction and slow-pull groups were also compared. The analysis did not reveal a significant difference in the long-axis diameter; however, there was a statistically significant difference in the short-axis diameter (p = 0.003). There was no statistically significant difference in the size of the peribronchial mass between the two groups. The location and size of LNs, as well as the size of the peribronchial mass, are shown in Table 2.
Comparison of the lymph node stations and the size of the lymph nodes and masses punctured between the two techniques.
The accuracy, sensitivity, specificity, negative predictive value (NPV), positive predictive value (PPV), and the number of tissue cores obtained using the suction and slow-pull techniques during EBUS-TBNA were 66.67% versus 85.71%, 43.75% versus 85.42%, 92.86% versus 87.5%, 59.09% versus 50%, 87.5% versus 97.62%, and 19 versus 50, respectively. The accuracy and sensitivity of the two techniques was significantly different (p = 0.039 and p < 0.001, respectively). The acquisition of tissue core was also significantly different (p = 0.004). However, the accuracy of benign conditions, accuracy of malignant conditions, specificity, NPV, and PPV of the two techniques were not significantly different (p > 0.05). The comparison of the accuracy, sensitivity, specificity, NPV, PPV and the acquisition of tissue core between the two techniques is shown in Table 3. There were no statistically significant differences in the blood contamination of samples between the two techniques (p > 0.05) (Table 4).
Comparison of diagnostic accuracy between the two techniques.

NPV, negative predictive value; PPV, positive predictive value.
Comparison of blood contamination between the two techniques.

The univariate analysis of factors affecting the diagnostic accuracy of EBUS-TBNA among all patients enrolled in this study is shown in Table 5. We assessed the associations with the long-axis diameter of the LN or mass (<30 mm versus ⩾30 mm), short-axis diameter of the LN or mass (<15 mm versus ⩾15 mm), EBUS-TBNA technique (suction versus slow-pull), acquisition of tissue core, and final pathology. We found that the slow-pull capillary technique [odds ratio (OR): 3, p = 0.043] and the acquisition of tissue core (OR: 5.244, p = 0.005) increased the diagnostic accuracy of EBUS-TBNA. In the multivariate analysis of factors affecting the diagnostic accuracy of EBUS-TBNA among all patients enrolled in this study, the acquisition of tissue core (OR: 6.673, p = 0.008) continued to exhibit a significant association (Table 5).
Univariate and multivariate analyses of diagnostic accuracy.

The univariate analysis of factors affecting the acquisition of tissue core in EBUS-TBNA among all patients enrolled in this study is shown in Table 6. We assessed the associations with the long-axis diameter of the LN or mass (<30 mm versus ⩾30 mm), short-axis diameter of the LN or mass (<15 mm versus ⩾15 mm), EBUS-TBNA technique (suction versus slow-pull), and final pathology (benign versus malignant result). We found that the slow-pull capillary technique increased the acquisition of tissue core in EBUS-TBNA (OR: 4.825, p = 0.006). In the multivariate analysis of factors affecting the acquisition of tissue core of EBUS-TBNA among all patients enrolled in this study, the slow-pull capillary technique (OR: 4.638, p = 0.023) continued to demonstrate a significant association (Table 6).
Univariate and multivariate analyses of the acquisition of tissue core.

Discussion
In recent years, the slow-pull capillary technique has been applied to EUS-FNA. It was first proposed by Chen and colleagues in 2011. 21 During this sampling process, a weak suction force is created due to the continuous withdrawal of the stylet, and the sample is drawn into the needle. In this study, we compared the outcomes of EBUS-TBNA using the suction and slow-pull capillary techniques. According to the results of the cytological and histopathological analyses, the specificity, NPV, and PPV of the two techniques were not significantly different. However, the accuracy and sensitivity of the slow-pull capillary technique were significantly higher than those of the suction technique. We also found that the diagnostic accuracy of the slow-pull capillary technique was significantly higher than that of the suction technique, and the slow-pull capillary technique was significantly associated with the diagnostic accuracy of EBUS-TBNA in both univariate and multivariate analyses. There was no significant difference in blood contamination of samples between the two groups.
The diagnosis of mediastinal diseases is difficult owing to the complicated anatomy of the mediastinum and the various aetiologies of the potential diseases. EBUS-TBNA is a safe and accurate examination associated with few complications and low rates of nondiagnostic and false-negative biopsies. 3 A meta-analysis of 14 studies on EBUS-TBNA reported an overall sensitivity of 66.2% and a specificity of 99.3%. 22 In the current study, the sensitivity of the suction technique (43.75%) and slow-pull capillary technique (85.42%) was lower and higher than the average, respectively. Of note, the difference between the sensitivity of the suction technique and slow-pull capillary technique observed in this study was statistically significant. However, the diagnostic accuracy of EBUS-TBNA has shown significant heterogeneity between studies in terms of sensitivity and NPV. 23 Numerous factors may contribute to these differences and be related to the underlying disease status of the patients. In particular, the diagnostic accuracy, sensitivity, and specificity of EBUS-TBNA for malignant diseases tend to be higher than the corresponding values for benign diseases; in addition, the results also differed for various types of tumors.24,25 This evidence was also supported by another study involving patients before definitive diagnosis, in which the corresponding values were also different. 26 In the current study, the enrolled patients were not definitively diagnosed prior to the operation, and the final diagnoses included malignant tumor, tuberculosis, sarcoidosis, nonspecific inflammation, hemophagocytic syndrome, and cryptogenic organizing pneumonia. We hypothesized that the differences in accuracy, sensitivity, specificity, NPV, and PPV between our study and other studies may be attributed to the undetermined actual disease condition of patients prior to the operation.
The suction technique with a 10-ml syringe is widely used in EBUS-TBNA, increasing the cellularity of the specimen versus the nonsuction approach. However, there is ongoing dispute regarding the role of suction during EBUS-TBNA. Casal and colleagues compared EBUS-TBNA biopsy with and without suction in 115 patients (192 LNs). They did not show significant differences in sample adequacy, diagnostic yield, and specificity between the two techniques. 12 Similarly, Scholten and colleagues investigated 121 patients (199 LNs), and also concluded that the use of suction or the stylet provided with EBUS-TBNA did not affect the diagnostic yield. 27 Boonsarngsuk and colleagues compared EBUS-TBNA with three levels of negative pressure (i.e. 0, 20, and 40 ml), showing that the diagnostic yield of EBUS-TBNA with suction was higher than EBUS-TBNA biopsy without suction. They also found that higher negative pressure was superior to lower negative pressure for obtaining adequate cytological specimens. 28
Similar to the use of a suction technique during EBUS-TBNA, the use of a suction technique during EUS-FNA remains controversial. Data from a randomized controlled trial conducted by Wani suggest that the suction technique should not be recommended during EUS-FNA of LNs. This recommendation is based on the increased risk of blood contamination of specimens and lack of effect on the overall diagnostic yield. 29 However, a randomized controlled trial of EUS-FNA for pancreatic solid masses with and without suction showed that suction increased the risk of blood contamination but also resulted in higher cellularity and sensitivity. 30 Furthermore, a randomized trial of 352 patients who underwent EUS-FNA for pancreatic masses compared the suction technique with that without suction. The results showed that the suction technique required a greater number of punctures to obtain an adequate sample and was linked to more blood contamination versus the technique without suction. Moreover, the diagnostic accuracy of the suction technique was also lower than that of the technique without suction. 31 In summary, it appears that the negative pressure created by suction in EUS-FNA increases the risk of blood contamination of samples, which may affect the results of the cytological analysis.
The slow-pull capillary technique is a new method involving a very weak suction force. An experimental study showed that the suction force produced by the slow-pull capillary technique with a 22-gauge needle was <2.0 kPa, which is significantly lower than that of the suction techniques involving 10-ml and 20-ml syringes. 32 This slight suction can assist in obtaining sufficient samples with minimal blood contamination.20,33 However, the application of the slow-pull capillary technique in EUS-FNA has been controversial. On the one hand, Kin and colleagues, concluded that the diagnostic accuracy was not significantly different between the suction and slow-pull capillary techniques in 40 patients with pancreatic solid lesions. However, the slow-pull capillary technique allowed the collection of high-quality specimens without blood contamination. 20 Similarly, another study showed that the diagnostic yield of EUS-FNA with the slow-pull capillary technique and suction technique was similar, though the former led to less blood contamination. 34 On the other hand, Wang and colleagues reported that the diagnostic accuracy of EUS-FNA with the slow-pull capillary technique was significantly superior to that achieved with suction using a 5-ml syringe and a 10-ml syringe. 35 In another study of 48 patients, the slow-pull capillary with fanning technique during EUS-FNA for pancreatic masses had a significantly superior diagnostic accuracy than the suction technique (88% versus 71%, respectively, p = 0.044). Moreover, use of the slow-pull capillary with fanning technique significantly reduced the risk of blood contamination of specimens (p = 0.041). 17
Although there has been some controversy regarding the use of the slow-pull capillary technique during EUS-FNA, we found some advantages associated with the use of this technique during EBUS-TBNA. We compared the results of EBUS-TBNA using the suction and slow-pull capillary techniques, and found that significantly higher diagnostic accuracy and sensitivity were obtained when the latter was applied. In addition, there was no significant difference in blood contamination between the two groups. However, in patients eventually diagnosed with malignant tumors or benign conditions, the results showed that there was no significant difference in diagnostic accuracy between the slow-pull capillary technique and suction technique. Regarding the above results, we consider that this was a retrospective study with a small total sample size. Following the independent analysis of cases diagnosed with benign diseases or malignant tumors, the number of cases in each group was much smaller, which affected the statistical results.
Histological specimens can improve the diagnostic accuracy of diseases involving hilar and mediastinal LN enlargement. The complete tissue structure of the material was more comprehensively and clearly observed in the histological specimen compared with the cytological specimen. However, most studies of EBUS-TBNA did not analyze the ability of each technique to provide histological samples. The biopsy specimens were mostly cytological specimens, and the collection of histological specimens was challenging.15,36 Using cell blocks as histological specimens, Žemaitis and colleagues compared the diagnostic accuracy of EBUS-TBNA cytological smears and cell blocks. 37 The results showed that the diagnostic accuracy of cell blocks was higher than that of cytological smears. Furthermore, the results also showed that the diagnostic accuracy of the combined specimens was significantly higher than the individual diagnostic accuracy of each kind of specimen. Hopkins and colleagues compared the diagnostic accuracy on smears and cell block. 38 The results showed that, in terms of diagnostic accuracy, the cell blocks were non-inferior to smears and provided sufficient histological specimens. However, the cell blocks were not strictly histological specimens. Hence, the complete LN structure could not be observed. In this study, we compared the results of EBUS-TBNA using the suction and slow-pull capillary techniques, and found that a significantly higher acquisition of tissue core was obtained following the application of the slow-pull capillary technique. Additionally, the univariate and multivariate analyses showed that the slow-pull capillary technique was an independent factor affecting the acquisition of tissue core of EBUS-TBNA. Moreover, the univariate and multivariate analyses showed that the acquisition of tissue core was an independent factor affecting the diagnostic accuracy of EBUS-TBNA. The results suggest that the slow-pull capillary technique during EBUS-TBNA could significantly increase the accuracy and sensitivity related to the diagnosis of diseases involving hilar and mediastinal LN enlargement by improving the acquisition of tissue core.
This study had several limitations. It was a single-center retrospective study, with a small total sample size and a relatively small number of patients that underwent the suction technique. These facts may have reduced the statistical power of this study to detect true differences between groups. In particular, there was a certain difference between the two groups in the number of patients eventually diagnosed with malignant tumors, which may result in statistical bias. However, all patients enrolled in this study had hilar or mediastinal LN enlargement due to unknown causes; the researchers were not biased in selecting the method of operation. Moreover, the results of this study were analyzed for the comprehensive accuracy, including those of the final diagnosis of benign and malignant diseases. Therefore, the results of this study have certain applicability and reference value in clinical practice. We plan to conduct a large, randomized, controlled trial to confirm the results of the present study. However, this study was the first to compare the suction and slow-pull capillary techniques during EBUS-TBNA.
In conclusion, EBUS-TBNA led to a high diagnostic accuracy and was safe for the diagnosis of diseases involving mediastinal and hilar LN enlargement. Compared with the suction technique, the slow-pull capillary technique during EBUS-TBNA can significantly increase the diagnostic accuracy related to diseases involving hilar and mediastinal LN enlargement by improving the acquisition of tissue core. Therefore, this technique has clinical significance in increasing the accuracy for the diagnosis of diseases involving mediastinal and hilar LN enlargement, and is worthy of application in EBUS-TBNA examinations.
Supplemental Material
Author_Response – Supplemental material for Slow-pull capillary technique versus suction technique in endobronchial ultrasound-guided transbronchial needle aspiration for diagnosing diseases involving hilar and mediastinal lymph node enlargement
Supplemental material, Author_Response for Slow-pull capillary technique versus suction technique in endobronchial ultrasound-guided transbronchial needle aspiration for diagnosing diseases involving hilar and mediastinal lymph node enlargement by Xin He, Yanjun Wu, Haoyan Wang, Ganggang Yu, Bo Xu, Nan Jia and Zhigang Yao in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1 – Supplemental material for Slow-pull capillary technique versus suction technique in endobronchial ultrasound-guided transbronchial needle aspiration for diagnosing diseases involving hilar and mediastinal lymph node enlargement
Supplemental material, Reviewer_1_v.1 for Slow-pull capillary technique versus suction technique in endobronchial ultrasound-guided transbronchial needle aspiration for diagnosing diseases involving hilar and mediastinal lymph node enlargement by Xin He, Yanjun Wu, Haoyan Wang, Ganggang Yu, Bo Xu, Nan Jia and Zhigang Yao in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1 – Supplemental material for Slow-pull capillary technique versus suction technique in endobronchial ultrasound-guided transbronchial needle aspiration for diagnosing diseases involving hilar and mediastinal lymph node enlargement
Supplemental material, Reviewer_2_v.1 for Slow-pull capillary technique versus suction technique in endobronchial ultrasound-guided transbronchial needle aspiration for diagnosing diseases involving hilar and mediastinal lymph node enlargement by Xin He, Yanjun Wu, Haoyan Wang, Ganggang Yu, Bo Xu, Nan Jia and Zhigang Yao in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
Authors Xin He and Yanjun Wu contributed equally to this work, and are co-first authors. We thank Zhang Qian, a statistician from the Clinical Epidemiology and EBM Unit, National Clinical Research Center for Digestive Disease, Beijing Friendship Hospital, Capital Medical University (Beijing, China), for helpful discussions.
Author contributions
Study design: ZY, XH, and YW; EBUS-TBNA performance: ZY; data collection: XH, YW, HW, GY, BX, and NJ; statistical analysis: XH, YW, and GY; data interpretation: XH, YW, HW, BX, and NJ; manuscript writing: XH and YW; manuscript revision: ZY, XH, YW, HW, GY, BX, and NJ.
Funding
The author(s) received no financial support for the research, authorship, and publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
The reviews of this paper are available via the supplemental material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.