
Abstract
Smoking causes various diseases and is a major public health threat worldwide. Therefore, promoting smoking cessation is the most important intervention contributing to maintaining the health of smokers and nonsmokers and saving enormous financial expense. We reviewed existing and emerging smoking-cessation pharmacotherapies from the Cochrane Database of Systemic Reviews, PubMed, Ovid, and ClinicalTrials.gov databases. A literature review revealed that bupropion may be appropriate for patients interested in reducing smoking who dislike, or who have failed, nicotine-replacement therapy (NRT). Additionally, varenicline and NRT are efficacious first-line smoking cessation treatments and should be given to all individuals unless contraindicated.
The reviews of this paper are available via the supplementary material section.
Introduction
An estimated 1.1 billion people use tobacco products worldwide.1,2 In 14 low- to middle-income countries (Bangladesh, Brazil, China, Egypt, India, Mexico, Philippines, Poland, Russia, Thailand, Turkey, Ukraine, Uruguay, and Vietnam), 48.6% [95% confidence interval (CI), 47.6–49.6] of men and 11.3% (10.7–12.0) of women used tobacco. Although a large reduction was observed in the prevalence of daily smoking, the number of cigarette smokers worldwide increased from 721 million in 1980 to 967 million in 2012. 3 Tobacco accounts for 11.5% of deaths, and 7.1 million people die of tobacco-related causes every year. 4 According to a prospective study of British physicians, those who smoked died on average approximately 10 years earlier than lifelong nonsmokers. 5
Smoking is associated with increased mutation burden and increases the risk of ⩾17 classes of human cancer.6,7 Sasazuki and colleagues showed that smoking is associated with an increased risk of a differentiated type of distal gastric cancer. Compared with a group that never smoked, the adjusted rate ratio of gastric cancer for previous and current smokers was 2.0 (95% CI, 1.1–3.7) and 2.1 (1.2–3.6), respectively. 8 Huxley and colleagues showed that the hazard ratio for lung-cancer mortality associated with current smoking was 2.48 (95% CI, 1.99–3.11) in Asia versus 9.87 (6.04–16.12) in Australia and New Zealand for men and 2.35 (1.29–4.28) in Asia versus 19.33 (10.0–37.3) in Australia and New Zealand for women. 9
Smoking increases the adherence of platelets and macrophages and creates a procoagulant and inflammatory environment, which can lead to cardiovascular diseases. 10 Mannami and coworkers demonstrated that the multivariate relative risk (RRs) using 95% CIs for current smokers compared with those for never-smokers after adjustment for cardiovascular risk factors and public health centres were 1.27 (1.05–1.54) for total stroke, 0.72 (0.49–1.07) for intraparenchymal haemorrhage, 3.60 (1.62–8.01) for subarachnoid haemorrhage, and 1.66 (1.25–2.20) for ischaemic stroke. 11 Smoking augments the production of numerous pro-inflammatory cytokines (e.g. tumour necrosis factor-alpha, interleukin (IL)-1, IL-6, IL-8, and granulocyte macrophage colony-stimulating factor) and decreases the levels of anti-inflammatory cytokines (e.g. IL-10). 12 Smoking leads to increased concentrations of immunoglobulin-E and to the subsequent development of atopic diseases and asthma. 12
Smoking increases the severity of asthma, and attenuates the effects of inhaled corticosteroids.13,14 Smoking produces proteases and oxidants from alveolar macrophages and neutrophils, causing tissue damage and contributing to the development of chronic obstructive pulmonary disease (COPD).15,16 Meta-analysis showed that smoking increased tuberculosis infection, and the RR estimate was 1.73 (95% CI, 1.46–2.04). 17 Smoking also increases the risk of contracting spontaneous pneumothorax, respiratory bronchiolitis-associated interstitial lung disease, and desquamative interstitial pneumonia.18,19 Furthermore, smoking is also associated with gastrointestinal disorders (e.g. peptic ulcers, inflammatory bowel disease 20 ),COPD, 21 and diabetes mellitus. 22 However, cohort studies have shown that smoking cessation for 10–15 years can reduce the risk of death and prolong survival.23,24
The total economic cost of smoking (from health expenditure and productivity losses combined) totalled a purchasing power parity of US$1436 billion in 2012, which was equivalent to 1.8% of the worldwide annual gross domestic product. 25 The number of labor years lost due to smoking-related mortality (which included the future labor years lost before retirement) was 26.8 million years, with 18.0 million years lost due to mortality and 8.8 million years lost due to disability. 25 Smoking-attributable health expenditures totalled a purchasing power parity of US$422 billion in 2012, and accounted for 5.7% of total health expenditures worldwide. 25
Therefore, tobacco smoking is a major public health and economic threat worldwide. Smoking cessation appears to be the most effective countermeasure against this threat. Here, we describe the molecular basis of nicotine addiction, and review approved drugs and currently investigated clinically relevant agents based on the Cochrane Database of Systemic Reviews, PubMed, Ovid, and ClinicalTrials.gov databases to aid understanding for clinicians and researchers. A search of these databases was conducted using the following terms: ‘smoking cessation’ or ‘nicotine-replacement therapy’. We also searched the following organization’s websites: the Japanese Respiratory Society and the Japanese Circulation Society. Randomized trials in which nicotine-replacement therapy (NRT) was compared with placebo or to no treatment, and trials in which different doses of NRT were compared are reviewed.
This review not only describes the latest clinical trials of smoking cessation treatments but also shows the flow of smoking cessation guidance being conducted in daily practice.
Neurogenetic determinants and mechanisms of nicotine addiction
Nicotine is soluble in lipids, has a binding rate to plasma proteins of ⩽5%, and passes readily through the blood–brain barrier. Nicotine absorbed from the lungs reaches the brain in 2–20 s and binds to the nicotinic acetylcholine receptors present in autonomic ganglia and neuromuscular junctions. The receptor involved in nicotine addiction is the α4β2 nicotinic acetylcholine receptor present in the ventral tegmental area of the midbrain. 26 When nicotine binds to this receptor, ion channels open and dopamine is released from the end of nerve fibres projecting to the nucleus accumbens (which is part of the mesolimbic system). Dopamine produces a momentary sense of pleasure and reward. Then, nicotine is rapidly metabolized to cotinine in the liver and excreted in urine. At 1 h after smoking, the concentration of nicotine decreases, the receptor is closed, and the smoker ‘craves’ nicotine. 27 By smoking again, physical nicotine addiction develops. In addition to dopamine, nicotine is involved in the release of neurotransmitters such as norepinephrine, serotonin, and γ-aminobutyric acid (GABA). 28
Guidance for smoking cessation
For smoking-cessation treatment of smokers, one must understand that smoking behavior is caused by nicotine dependence. The nicotine contained in tobacco can be as addictive as narcotics and alcohol. Smoking behavior is tobacco-dependent, and, in 1992, the WHO International Classification of Diseases 10th Revision (ICD-10) classified nicotine as a psychoactive-substance disorder similar to cocaine. Furthermore, in 1994, the Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV defined ‘tobacco dependence’ as nicotine dependence. The Tobacco Dependence Screener is effective for the diagnosis of nicotine addiction. 29 If nicotine addiction is severe, patients may become mentally unstable and have vague feelings of anxiety. Moreover, for patients who could not quit smoking because of withdrawal symptoms, it is recommended to support smoking cessation while providing information that effective treatment methods have been established for smoking cessation.
Prochaska and colleagues proposed a ‘stage model of behavioral change’ that classifies smoking cessation into five stages: precontemplation, contemplation, preparation, action, and maintenance. 30 The efficacy of providing smoking cessation instructions is low for patients in the precontemplation stage who are not interested in smoking cessation, but the success rate of smoking cessation increases at the higher stages. The ‘5A approach’ (ask, advise, assess, assist, and arrange) provides motivation for quitting smoking for patients. The 5A approach can be initiated in a short time in daily outpatient clinics and upon medical examinations.31,32 For smokers not willing to quit, motivational counselling using the ‘5R Approach’ (relevance, risks, rewards, roadblocks, repetition) can be useful. 31
Next, an outline of an intervention to assist smoking cessation is demonstrated for outpatients at the first visit. After the patient completes a questionnaire, they receive instructions on how to deal with smoking cravings, given training on problem-solving skills, and shown how to write a smoking-cessation diary. Then, the patient receives an explanation of NRT. The carbon monoxide concentration in exhaled breath is measured, and its importance explained. The patient and healthcare worker discuss how to cope with ‘re-smoking’ situations. The patient and healthcare worker also set a start date for smoking cessation and set appropriate goals that can be achieved. Finally, the patient and healthcare worker set the next visit date. Counselling by the healthcare practitioners through smoking interventions is more effective if the interview time is long, and interviews occur as frequently as possible.
To address smoking cravings, it is important to promote a correct understanding of tobacco use. To overcome psychological dependence, the patient should learn a way that suits them. Nicotine dependence involves self-titration, so if the patient reduces the number of cigarettes smoked, they will involuntarily take deep and frequent inhalations of the cigarette while smoking. Therefore, reducing the number of cigarettes is not an efficacious means of quitting smoking, and physicians should not recommend reducing the number of cigarettes for patients who cannot quit smoking.
For effective smoking cessation, making regular contact with healthcare workers (similar to treatment for other lifestyle-related diseases) is important. As a key to the continuation of smoking cessation, it is important to provide support for the prevention of re-smoking when relapse is likely to occur (usually 3 months after the start of smoking cessation).
Pharmacotherapeutic interventions/treatments for smoking cessation
Nicotine dependence is closely related to smoking habits. NRT, varenicline, and sustained-release bupropion are regarded as first-choice therapies for smoking cessation in the Clinical Practice Guideline sponsored by the US Department of Health and Human Services. 33
NRT
NRT is particularly effective in patients who are heavily dependent upon nicotine and have severe withdrawal symptoms (i.e. irritability/frustration/anger, anxiety, difficulty in concentrating, restlessness/impatience, depressed mood/depression, insomnia, increased appetite/weight gain). By temporarily replacing the nicotine consumed from cigarettes when smoking, the patient is relieved of the unpleasant withdrawal symptoms that appear during smoking cessation, thereby resulting in easier smoking cessation. Patients with moderate or severe dependence upon nicotine must use a sufficient amount of nicotine in replacement preparations because withdrawal symptoms strongly appear from several days to 2 weeks after the start of smoking cessation. Nicotine preparations (e.g. gum, lozenge, or nicotine patches, and their combination) reduce the intensity of craving and withdrawal symptoms by replacing the nicotine present in cigarettes. 34 Although cigarette smoke contains ~200 toxic agents, NRT contains only nicotine and releases less nicotine than cigarette smoke. Nicotine is harmful to humans, so NRT is contraindicated in nonsmokers as well as in people with unstable angina, acute myocardial infarction, severe arrhythmias, or the early phase of cerebrovascular disease. Continuing to smoke during pregnancy is very dangerous, but NRT may be used for pregnant women if written informed consent has been obtained. One meta-analysis showed the benefits of this intervention [two studies (2261 patients): RR, 1.24; 95% CI, 1.04–1.47; I2 = 56%]. 35
The nicotine concentration in nicotine gum can be adjusted readily by making it smaller (using scissors) or reducing the number of bites. Side effects of intraoral problems, sore throat, and stomach pain have been reported. 36 Furthermore, dependence on nicotine gum has been documented. 37 Nicotine gum can cause symptoms of acute nicotine poisoning if it is chewed quickly. However, the absorption of nicotine is difficult under acidic conditions, so the risk of acute nicotine poisoning is low even if it is consumed accidentally, and it is relatively safe.
A nicotine patch is started at the required dose and then reduced according to the degree of ‘craving’. Side effects such as contact dermatitis, headache, general fatigue, and insomnia have been reported. In addition, smoking during simultaneous application of a nicotine patch can cause coronary artery disease, such as myocardial infarction, arrhythmia, and angina. If acute nicotine intoxication appears, the patch should be removed immediately, and the application site should be washed with water. At this time, the use of soap is contraindicated because it promotes nicotine absorption under alkaline conditions. The nicotine concentration in plasma does not decrease immediately because nicotine remains at the same concentration for ~2 h after discontinuation, and then disappears with a half-life of 5–7 h. Therefore, symptom amelioration often requires several hours, and in the case of severe symptoms, medical treatment is indicated.
Nicotine pressurized metred-dose inhalers (pMDI) are a safe, effective, and inexpensive method of pulmonary nicotine delivery, and are commonly used during clinical practice. 38 Caldwell and colleagues showed that the abstinence prevalence of a group using nicotine pMDI plus the nicotine patch was significantly higher than that of a placebo plus nicotine patch group (32% versus 18%, p < 0.001). 38
Sustained-release bupropion
Sustained-release bupropion (amfebutamone) is a non-nicotine agent. Sustained-release bupropion is an efficacious and well-tolerated smoking-cessation intervention. 39 Bupropion has been approved for the treatment of major depressive disorder and seasonal affective disorder. 40 According to population-based studies, 41 smokers are more likely than nonsmokers to have symptoms of affective disorders, so antidepressants or anxiolytics seem to be efficacious cessation aids.
Hurt and colleagues showed that the abstinence prevalence of a group taking 300 mg of bupropion/day for 7 weeks was significantly higher than that of a placebo group (23% versus 12%, p < 0.01). 42 Jorenby and coworkers revealed that the abstinence prevalence at 12 months was 16.4% in a nicotine-patch group, 30.3% in a bupropion group (p < 0.001), and 35.5% in a group given bupropion and a nicotine patch (p < 0.001) compared with 15.6% in a placebo group. 43 One meta-analysis did not show a significant difference between bupropion and NRT with respect to the abstinence prevalence. 44 Therefore, bupropion seems to be appropriate for patients interested in reducing smoking who dislike, or who have failed, NRT. 45 Furthermore, it has been reported that bupropion administration is associated with shorter periods between cessation attempts and that it may increase the prevalence of short-term abstinence. 46 Side effects of insomnia (42.4%) and dry mouth (10.7%) were significantly more frequent in a bupropion group than in a placebo group (19.5% and 4.4%, respectively, p < 0.05) in the study by Jorenby and colleagues. 43
Varenicline
Varenicline acts as a partial agonist/antagonist with affinity and selectivity for α4β2 nicotinic acetylcholine receptors. Varenicline helps patients achieve smoking cessation by reducing cravings/withdrawal symptoms and smoking satisfaction. 47
Varenicline administration was associated with a higher prevalence of continuous abstinence at 4 weeks than placebo [44.0% versus 17.7%; odds ratio (OR), 3.85; 95% CI, 2.70–5.50; p < 0.001] and a higher prevalence of continuous abstinence at 4 weeks than sustained-release bupropion administration (44.0% versus 29.5%; OR, 1.93; 95% CI, 1.40–2.68; p < 0.001) in a study by Gonzales and colleagues. 48 Varenicline in combination with NRT was associated with a higher prevalence of continuous abstinence than placebo at 12 weeks (55.4% versus 40.9%; OR, 1.85; 95% CI, 1.19–2.89; p = 0.007) and at 24 weeks (49.0% versus 32.6%; OR, 1.98; 95% CI, 1.25–3.14; p = 0.004) as well as point prevalence abstinence at 6 months (65.1% versus 46.7%; OR, 2.13; 95% CI, 1.32–3.43; p = 0.002) in a study by Koegelenberg and colleagues. 49 In the combination-treatment group, only skin reactions reached significance (14.4% versus 7.8%; p = 0.03). In a meta-analysis of 14 varenicline trials, when focusing on serious adverse events, no difference was found between the varenicline and placebo arms (RR, 1.06; 95% CI, 0.72–1.55), and subgroup analyses detected no significant excess neuropsychiatric (RR, 0.53; 95% CI, 0.17–1.67), or cardiac (RR, 1.26; 95% CI, 0.62–2.56) events. 44 However, if depressive mood, anxiety, irritability, excitement, behavioral changes, and suicidal ideation are seen, patients must stop taking varenicline and contact a physician promptly.
Nortriptyline
Nortriptyline is a classic tricyclic antidepressant. It has shown some efficacy in smoking cessation. The abstinence prevalence at 6 months was 14% in a nortriptyline group compared with 3% in a placebo group (p = 0.003; absolute difference, 11%; 95% CI, −18% to −4%) in a study by Prochazka and coworkers. 50
Clonidine
Clonidine was originally used as an antihypertensive agent that acts on the central nervous system to reduce withdrawal symptoms in various addictive behaviors. 51 Franks and colleagues carried out a randomized, double-blind study of clonidine for smoking cessation in a primary care setting. At 4 weeks, 18% of participants receiving clonidine had quit smoking compared with 14% receiving a placebo (chi-squared test = 0.7; 90% CI of benefit from clonidine, −4% to 13%). 52 In a study by Hilleman and coworkers, the number of smokers withdrawing from the study was not greater with clonidine compared with placebo (9% versus 7%, respectively). 53 However, women receiving clonidine had a significantly higher prevalence of abstinence than men receiving clonidine at all follow-up visits. Therefore, clonidine could have a role in women smokers only.
Other agents
Trials evaluating selective serotonin reuptake inhibitors,44,54 anxiolytics, 55 monoamine oxidase inhibitors,56–60 psychostimulants, 61 other nicotinic acetylcholine receptor agonists and antagonists, 62 quinine-methyl valerate-camphor-eucalyptus oil,63–65 opioid antagonists,66–68 selective cannabinoid type-1 receptor inverse agonists,69,70 silver acetate, 71 supplements, 56 other tricyclic antidepressants, 56 5-hydroxytryptamine-3 antagonists,72,73 agonists of α-type peroxisome proliferator-activated receptors, 74 N-methyl-D-aspartate receptor modulators, 75 cycloserine, 76 memantine, 77 dopamine enhancers and receptor modulators, 78 and nicotine vaccines79,80 have failed to show clear benefits for smoking cessation. 81
Trials on new pharmacologic treatments that could aid smoking cessation
New pharmacologic agents to aid smoking cessation are in the early stages of clinical trials. 82 In particular, acetylcholinesterase inhibitors and N-acetylcysteine (NAC) seem to be promising.
Acetylcholinesterase inhibitors
Acetylcholinesterase inhibitors are used to treat the cognitive deficits associated with Alzheimer’s disease. 83 Recently, they have been reported to be efficacious against drug addiction (including nicotine dependence).84,85 Repeated administration of acetylcholinesterase inhibitors (e.g. galantamine and donepezil) attenuates nicotine self-administration in rats. 86 A 12-week, randomized, placebo-controlled trial revealed that the rivastigmine group showed a decrease in daily smoked cigarettes (−30%), exhaled carbon monoxide (−32%), and tobacco craving (−18%), whereas the control group did not show significant changes. 87
Agents affecting GABA receptors
GABA is a nonprotein amino acid. It is an important inhibitor of neurotransmission in the human brain. Topiramate facilitates GABAergic neurotransmission via allosteric modulation of a nonbenzodiazepine site on the GABA-A receptor. A 10-week randomized trial revealed a prevalence of 4-week continuous abstinence of 5% in the placebo group, 26% in the topiramate group, and 37% in a group taking topiramate combined with a nicotine patch. 88 Pairwise comparisons showed a difference between the topiramate combined with a nicotine patch and placebo groups (p = 0.042) and a nonsignificant difference between the topiramate and placebo groups (p = 0.18).
NAC
NAC is a widely available, tolerable, and affordable nutraceutical supplement that increases the intracellular levels of glutathione (a major antioxidant) and modulates oxidative, immune-inflammatory, glutamatergic, and neurotrophic pathways.89,90 In a study by Prado and colleagues, NAC treatment significantly reduced the daily number of cigarettes used (Δ mean ± SD = −10.9 ± 7.9 in the NAC-treated group versus −3.2 ± 6.1 in the placebo group) and exhaled carbon monoxide (Δ mean ± SD = −10.4 ± 8.6 ppm in the NAC-treated group versus −1.5 ± 4.5 ppm in the placebo group). 91
Cytisine
Cytisine is a plant-based medication. It has been used for >50 years for smoking cessation in central and eastern Europe. A two-arm, parallel-group, randomized, non-inferiority trial is in progress to evaluate the efficacy, safety, and cost-effectiveness of cytisine compared with varenicline for smoking cessation. 92
Other agents
Clinical trials for other agents are summarized in Table 1. Although cigarettes represent ~90% of tobacco/nicotine use, the market for ‘e-cigarettes’ is growing. Recently, a randomized trial revealed that the prevalence of abstinence from tobacco at 1 year was 18.0% in the e-cigarette group compared with 9.9% in the NRT group (RR, 1.83; 95% CI, 1.30–2.58; p < 0.001). 93 However, the long-term safety of e-cigarettes has not been established.
Clinical trials with pharmacologic treatments for smoking cessation.
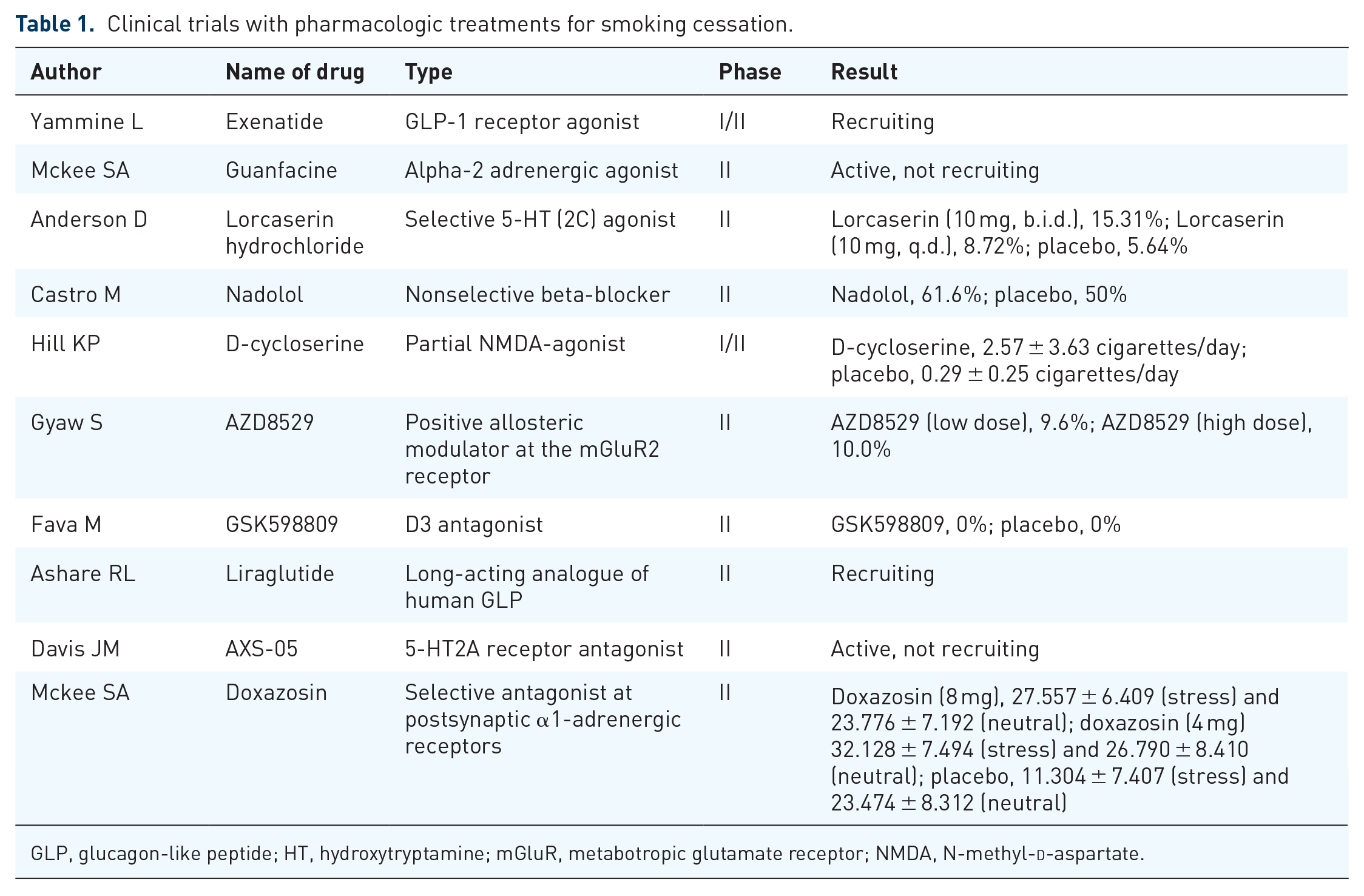
GLP, glucagon-like peptide; HT, hydroxytryptamine; mGluR, metabotropic glutamate receptor; NMDA, N-methyl-
Conclusion
The harmfulness of smoking is indisputable. There is sufficient evidence that smoking has a causal relationship with cancers of the oral cavity, pharynx, larynx, lungs, and various organs. It is desirable for all healthcare workers to know the smoking status of all patients and to provide appropriate, broad, advice regarding smoking cessation to all patients who smoke. NRT will be a great help for patients who wish to quit smoking.
Supplemental Material
Author_Response_to_Reviewer_Comments – Supplemental material for Current pharmacologic treatments for smoking cessation and new agents undergoing clinical trials
Supplemental material, Author_Response_to_Reviewer_Comments for Current pharmacologic treatments for smoking cessation and new agents undergoing clinical trials by Tatsuya Nagano, Masahiro Katsurada, Yuichiro Yasuda, Kazuyuki Kobayashi and Yoshihiro Nishimura in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.1 – Supplemental material for Current pharmacologic treatments for smoking cessation and new agents undergoing clinical trials
Supplemental material, Reviewer_1_v.1 for Current pharmacologic treatments for smoking cessation and new agents undergoing clinical trials by Tatsuya Nagano, Masahiro Katsurada, Yuichiro Yasuda, Kazuyuki Kobayashi and Yoshihiro Nishimura in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_1_v.2 – Supplemental material for Current pharmacologic treatments for smoking cessation and new agents undergoing clinical trials
Supplemental material, Reviewer_1_v.2 for Current pharmacologic treatments for smoking cessation and new agents undergoing clinical trials by Tatsuya Nagano, Masahiro Katsurada, Yuichiro Yasuda, Kazuyuki Kobayashi and Yoshihiro Nishimura in Therapeutic Advances in Respiratory Disease
Supplemental Material
Reviewer_2_v.1 – Supplemental material for Current pharmacologic treatments for smoking cessation and new agents undergoing clinical trials
Supplemental material, Reviewer_2_v.1 for Current pharmacologic treatments for smoking cessation and new agents undergoing clinical trials by Tatsuya Nagano, Masahiro Katsurada, Yuichiro Yasuda, Kazuyuki Kobayashi and Yoshihiro Nishimura in Therapeutic Advances in Respiratory Disease
Footnotes
Acknowledgements
We express our gratitude to the members of the Division of Respiratory Medicine, Kobe University Graduate School of Medicine (Kobe, Japan) for helpful discussions.
Funding
The author(s) received no financial support for the research, authorship, and publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
The reviews of this paper are available via the supplementary material section.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.