
Abstract
Objectives:
The tobacco epidemic represents one of the most significant public health challenges faced globally. Nicotine replacement therapy was developed to substitute for the nicotine contained in tobacco products temporarily. The objective of this study was to investigate pharmacists’ knowledge, attitudes, and practices regarding the utilization of nicotine replacement therapy in Iraq.
Methods:
This cross-sectional study involved 300 pharmacists across five provinces from October 1, 2023 to December 31, 2023.
Results:
Indicate that 300 pharmacists participated in the analysis, with approximately two-thirds identifying as male. About two-thirds of the participants (95% confidence interval: 65.3%) expressed that they knew how to use nicotine replacement therapy. Furthermore, about half of them (95% confidence interval: 50.3%) reported their awareness of how to make dose titration, with a majority agreeing that the assessment of nicotine dependence influences the selection of nicotine replacement therapy products. Fair knowledge was associated with each degree of education, not attending training programs, and the availability of nicotine replacement therapy in their pharmacies (0.01, 0.002, 0.003, respectively).
Conclusions:
There exists a critical necessity for pharmacists to augment their comprehension of the medications utilized in smoking cessation. Such enhancement is essential to improve their practices and, consequently, to attain superior outcomes in supporting individuals in their efforts to quit smoking.
Introduction
The tobacco epidemic poses one of the most significant challenges to public health on a global scale, impacting over eight million individuals annually. More than seven million deaths are attributable to direct tobacco consumption, while ~1.3 million fatalities occur among nonsmokers due to exposure to secondhand smoke. This underscores our collective capability to effect meaningful change and foster a healthier future for all.1,2 Numerous individuals who engage in smoking and comprehend the associated health risks are often motivated to cease this habit. With the provision of counseling and pharmacological support, they can significantly improve their likelihood of achieving a successful cessation.1,3 A significant and irreconcilable conflict exists between the interests of the tobacco industry and the advancement of public health. The tobacco industry produces and markets a product, that is, scientifically established to be addictive, inflicting disease and mortality while exacerbating societal challenges, including heightened poverty levels. The human and economic consequences resulting from tobacco use are both staggering and preventable. In light of the tobacco industry’s efforts to minimize the risks associated with its products, everyone must remain committed to advocating for a healthier future.
The WHO Framework Convention on Tobacco Control (FCTC) is a monumental achievement in promoting public health. This evidence-based treaty embodies every individual’s right to the highest standard of health, providing a solid legal framework for international health cooperation and setting high standards for compliance. Since its implementation in 2005, the FCTC has united 182 Parties, reaching over 90% of the world’s population. In 2007, the WHO introduced the impactful MPOWER initiative, a practical and cost-effective approach to enhance the implementation of the demand reduction provisions outlined in the FCTC. 1 According to the WHO report, Iraq is one of the countries that has banned electronic nicotine devices. In 2021, the daily smoking prevalence was 17%, and the tax applied on cigarettes was 16.9%. 4 Despite reports indicating that Iraq has implemented a ban on smoking in public transport, the reality is that this regulation is not fully enforced in everyday situations. 4 A significant number of smokers are aware of the risks associated with tobacco use, and the majority expresses a desire to quit. Evidence suggests that utilizing counseling and medication can more than double the likelihood of a tobacco user successfully quitting. Health professionals possess the greatest capacity among societal groups to advocate for and facilitate the reduction of tobacco consumption.5,6 Meta-analyses presented in the 2008 Update unequivocally demonstrate that the combination of counseling and medication yields the most favorable outcomes in smoking cessation efforts. Specifically, research indicates that integrating counseling with medication enhances recovery outcomes, while the addition of medication to counseling also contributes positively to treatment efficacy. Furthermore, the update outlines general guidelines for the utilization of nicotine replacement therapy (NRT) medications. It is noteworthy that a separate meta-analysis within the 2008 Update concluded that providing training to clinicians significantly increases the proportion of smokers who receive comprehensive treatment, which includes discussions regarding the benefits and challenges of quitting, medication options, and necessary support services. 7 NRT was developed to serve as a temporary substitute for the nicotine derived from tobacco. This intervention aims to mitigate the motivation to consume tobacco and to alleviate symptoms associated with nicotine withdrawal, thereby facilitating the transition from cigarette smoking to complete cessation. NRT products exhibit varying levels of efficacy and differing rates of nicotine absorption. Although optimal results are achieved when NRT is used in conjunction with cessation counseling, these products can still prove effective in the absence of supplementary behavioral therapy. 8 NRT products are classified as Group C medications under the Poisons Act of 1952, which permits their dispensing without a doctor’s prescription. 9 In Iraq, the absence of dedicated smoking cessation clinics presents a unique challenge, as community pharmacists play a crucial role in supporting individuals seeking to quit smoking. These pharmacists often take on the responsibility of prescribing and dispensing NRT, yet many lack the necessary training or comprehensive knowledge regarding its proper usage and guidelines. This study aims to delve deeper into the expertise, attitudes, and practices of pharmacists concerning NRT in Iraq, highlighting the importance of equipping them with the right tools and information to effectively assist their communities in quitting smoking.
Methods
This cross-sectional study was conducted among 300 pharmacists across five provinces: Karbala, Najaf, Diwaniya, Simawa, and Basra. The study occurred from October 1, 2023 to the end of December 2023. Pharmacists were asked if they would participate, and all participants signed a consent form to confirm their willingness. Each pharmacist independently filled out a questionnaire, and the researcher reviewed the completed questionnaires to determine whether they were biased, legible, and met the inclusion criteria. The criteria for inclusion in this study primarily involved the enrollment of licensed pharmacists who were actively employed in private sector settings at the time of the research. Therefore, the exclusion criteria would be those who do not meet the inclusion criteria. The researcher developed a new tool, the “Questionnaire,” to assess pharmacists’ knowledge, attitudes, and practices regarding the use of NRT in Iraq. To ensure face and content validity, the questionnaire was reviewed by six specialized pharmacists, five of whom were faculty members with experience and expertise in survey instrument development and research. Modifications suggested were considered, and changes were made accordingly. A reliability analysis of the questionnaire, using Cronbach’s alpha, showed an internal consistency reliability of 0.9. Testing the questionnaire among 20 participants (6.6%) revealed that the estimated time required to complete it was ~10 min. Demographic information was collected, and questions were carefully adapted and rephrased to assess pharmacists’ knowledge, attitudes, and practices regarding the use of NRT. This approach was informed by the literature review and aligned with the study’s objectives.3,6,7,10,11 Some suggestions were provided by experts who reviewed the questionnaire for validation. The questionnaire was evaluated and translated in accordance with the Principles of Good Practice for Translation and Cultural Adaptation. 12 Following the preparation of the questions, the researcher commenced the translation process into Arabic. This included stages of reconciliation, back translation, review of the back translations, harmonization, and cognitive debriefing. Subsequently, the researcher undertook a review of the results from the cognitive debriefing, finalized the content, conducted proofreading, and prepared the final report. 12
All results were presented in tables as appropriate. The sample size required for the study was calculated using the equation below13 –15:

where n = the sample size; Z = the statistic for the 95% level of confidence used in the power analyses (Wilson Score),16,17 which was 1.96; p = the expected prevalence or the proportion used, which was (7%) = 0.07 according to the World Bank, Iraq population about 43,557,859 18 and the number of Iraqi pharmacists is about 31,000 pharmacists 19 ; and d = the precision used, which was 0.0.036 (according to Niang d = 1/2 p). 20 Applying these values to the equation, the sample size equals 192. Adding an extra population to avoid bias and missing data will increase the sample size to 300 pharmacists.
Statistical analyses
The data analysis was conducted using the SPSS software package (version 20; SPSS, Inc., Chicago, IL, USA). The age of the participants, the length of their experience as community pharmacists, their weekly working hours, and the average number of patients counseled daily were reported as means ± standard deviations. Categorical variables were summarized in terms of frequencies and percentages. In the knowledge section, which comprises six questions with a maximum score of six points, each correct response (indicated by “yes”) is attributed a score of 1, while incorrect responses (indicated by “no”) receive a score of 0. Participants’ overall knowledge scores are classified using Bloom’s cut-off points. 21 Scores ranging from five to six points are categorized as “good,” scores between three and four points are categorized as “fair,” and scores of two points or less are categorized as “poor.”
In the attitude section, which consists of five questions with a maximum score of five points, each correct response (marked “yes”) is assigned a score of 1, whereas incorrect responses (marked “no”) are awarded a score of 0. Participants’ overall attitude scores are similarly classified according to Bloom’s cut-off points. 21 Scores from four to five points are deemed “good,” scores between two and three points are classified as “fair,” and scores below two points are categorized as “poor.” In the practice section, which comprises six questions with a total possible score of six points, each correct response is awarded one point. It is noteworthy that not all responses that receive approval are necessarily correct, as certain negative statements can also be valid. Incorrect responses are assigned a score of 0. Participants’ overall practice scores are classified according to Bloom’s cut-off points. 21 A score of five to six points is deemed “good,” a score of three to four points is categorized as “fair,” and a score of less than three points is classified as “poor.”
In the barriers section, which also consists of six questions and a total possible score of six points, each affirmative response (designated as “yes”) is assigned one point, while negative responses (designated as “no”) receive a score of 0. Participants’ overall barriers scores are similarly classified using Bloom’s cut-off points. 21 A score of five to six points indicates that participants are “highly affected” by the barriers, a score of three to four points suggests they are “fairly affected,” and a score of less than three points designates that they are “not affected” by the barriers. The scores for knowledge, attitude, practice, and barriers were calculated, and the Pearson’s chi-square test was used to identify associations between the variables with a 95% confidence interval (CI; Wilson Score).
Results
A total of 300 pharmacists participated in the study, all of whom were included in the analyses. Approximately two-thirds of the participants were male. The study encompassed pharmacists from five provinces, with the majority possessing a bachelor’s degree in pharmaceutical science and identifying as nonsmokers. Demographic data for the participants are presented in Table 1.
Participants’ demographics (N = 300).
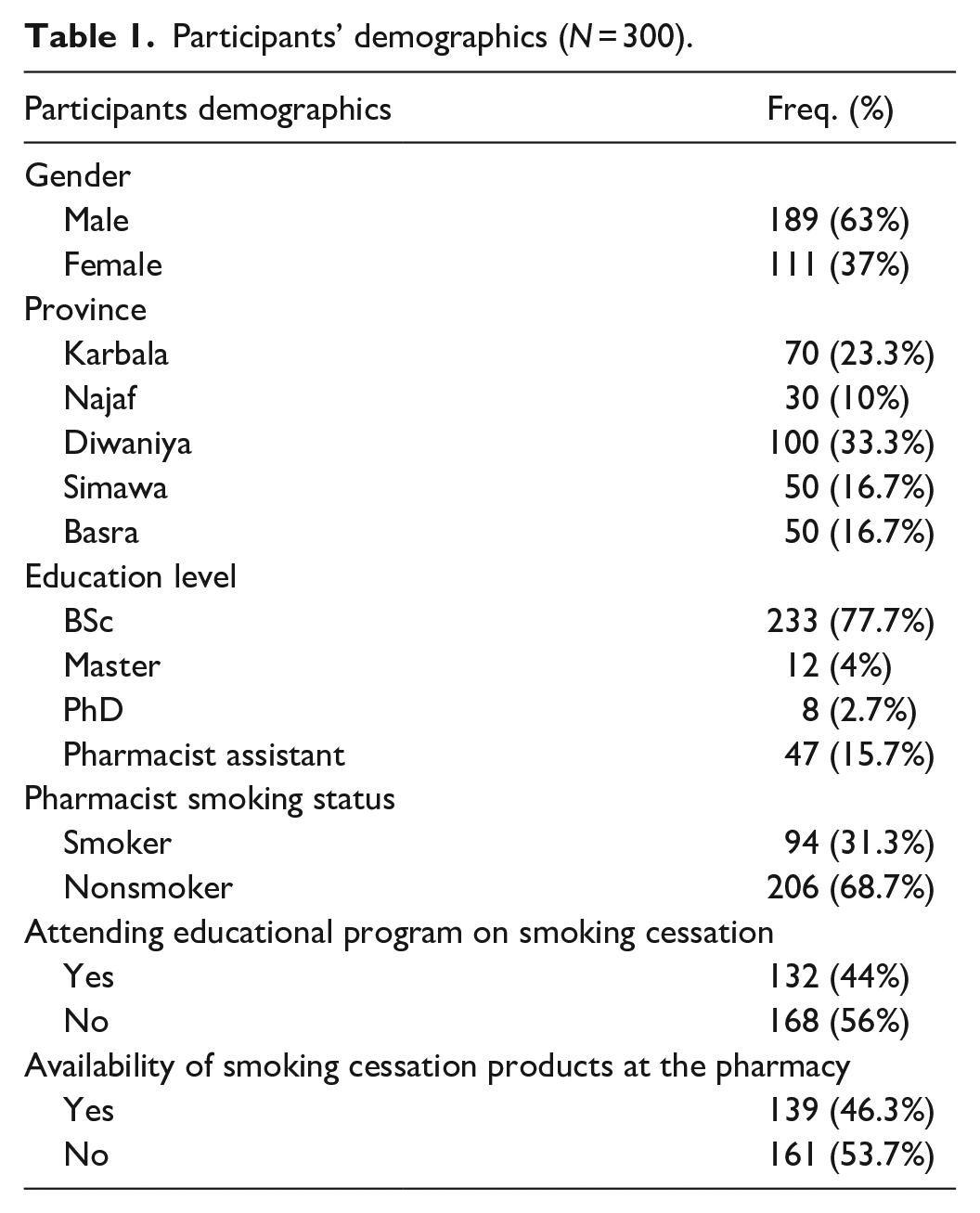
Participants had an average age of 32.8 years (±9.7 years) and had been working in community pharmacy for an average of 9.2 years (±8.6 years). They worked an average of 28.3 h/week (±11.6 h) and counseled ~63.4 patients daily (±61.2 patients).
Table 2 presents the pharmacists’ responses to the knowledge questions. About half of the participants were aware of the contraindications for NRT and understood the dose titration protocol. However, only about (95% CI: 30%) were knowledgeable about how to assess a patient’s level of nicotine dependence and agreed that NRT use should be limited to 2 weeks.
Participants’ knowledge regarding NRT usage.

NRT: nicotine replacement therapy.
Table 3 demonstrates that two-thirds (95% CI: 63%) of the participants felt confident in their ability to help patients quit smoking through consistent advice and follow-up. Additionally, about half of the participants (95% CI: 49.7%) believe that nicotine addiction and drug addiction should be regarded as equally important. Over two-thirds of participants (95% CI: 75.7%) recommend routinely using NRT for all smokers, and most agree that assessing nicotine dependence influences the selection of NRT medication.
Participants attitude and practice regarding NRT usage.

NRT: nicotine replacement therapy.
Table 4 shows that the majority of participants (95% CI: ranged 84%–93%) agreed that a lack of time, a private area for counseling, and training courses on how to use NRT are the primary factors that prevent them from providing counseling.
Pharmacists facing barriers to the usage of NRT.

NRT: nicotine replacement therapy.
Table 5 presents the participants’ knowledge, attitudes, and practices (KAP) regarding NRT, as well as the barriers they encountered. Approximately half of the participants demonstrated a fair understanding of NRT usage and reported being significantly impacted by various barriers. In contrast, about two-thirds of the participants showed a fair attitude and practice concerning the use of NRT.
Participants’ KAP and barriers scoring.

The results indicated a significant association between practice and gender, as well as a significant relationship between knowledge and the educational level of participants (p = 0.01). However, participants’ smoking status showed no significant association with any of the KAP data. There was a fair level of knowledge and attitude among participants regarding their attendance at educational programs on smoking cessation, with a significant disagreement noted (p = 0.002 for knowledge and p = 0.003 for attitude). Additionally, participants demonstrated significant fair practice based on their gender and origin (see Table 6).
KAP association with participants’ demographics.

95% Confidence intervals.
Discussion
Quitting smoking is a powerful choice that can significantly transform your health for the better, no matter your age or how long you have smoked. 22 NRT products can be utilized with or without supplementary counseling. Furthermore, they do not necessitate a physician’s prescription, as they are categorized as Group C medications under the Poisons Act of 1952. 23 In Iraq, the absence of smoking cessation clinics presents a significant challenge. Consequently, community pharmacists are responsible for prescribing and dispensing NRT without formal training or knowing its proper application. Despite this limitation, approximately half of the participants reported having engaged in smoking cessation programs. These results align with the findings of the study conducted by Sakka et al. 10 A study involving pre- and posttraining surveys was conducted with 142 pharmacy students at Texas Southern University. The results indicated that the training program had a substantially positive effect on the students’ perceived abilities and confidence in offering tobacco cessation counseling to patients. This highlights the critical need for specialized tobacco cessation training for all current and future healthcare providers. In particular, pharmacists hold a distinctive position within the community, enabling them to serve all patients, including individuals from medically underserved populations. Therefore, it is imperative to equip pharmacists with the necessary skills and knowledge to effectively aid patients in their efforts to quit smoking, thereby enhancing public health outcomes. 24 In accordance with this, another study demonstrated that comprehensive training significantly enhanced pharmacy students’ perceived confidence and competence in delivering tobacco cessation counseling. 25 Our study results show that around one-third of the participants were active smokers. However, this finding did not reveal a significant connection to any of the knowledge, attitudes, or practices evaluated in the study. This contrasts with the assertions made in Fowler and Godfrey’s book, which states that a person’s smoking status influences their attitudes and behaviors toward smoking cessation. 26 Over half of the participants were aware of the use and contraindications of smoking cessation medications, and approximately half also understood the dose titration of these treatments. These findings align with the results of Sakka’s study. 10
Half of the participants believe that smoking cessation is not their responsibility and that it is less important than drug addiction. They feel they cannot provide professional advice on smoking cessation because they do not consider it part of their job. In contrast, the results of the Sakka study indicate that the majority of participants believe it is their responsibility to offer advice regarding smoking cessation. 10 The findings from our study indicate that ~70% of participants reported receiving satisfactory guidance on smoking cessation. This result underscores the commitment to promoting effective health practices in our community.
Our study results clearly demonstrate that a lack of knowledge and skills is a significant barrier to providing smoking cessation services, as reported by the majority of participants. It is imperative to recognize that smoking cessation interventions are a crucial responsibility of pharmacists. Consequently, we strongly advocate including smoking cessation training, such as the Mandatory Continuing Professional Development Training mandated by the Pharmacists’ Council of Nigeria. 27 Integrating smoking cessation counseling into undergraduate pharmacy curricula is essential. This can be achieved by offering specialized workshops or certification programs, establishing mentorship systems, and utilizing digital learning platforms for continuous education. These approaches will enhance the competence of future pharmacists in addressing smoking-related health issues. A 10-page survey was mailed to all licensed pharmacists in four California counties. The results showed that, out of the 715 pharmacists who have direct patient contact, 93% indicated that receiving specialized training in tobacco cessation counseling would enhance the quality of their counseling. Additionally, 70% believed such training would increase the number of patients they could counsel. However, the study also revealed a negative attitude toward smoking cessation among some pharmacists. Despite this, 88% of respondents expressed an interest in receiving specialized training to develop these skills. 28 Research on public health initiatives that offer free nicotine replacement products through telephone quit lines has shown an increase in both call volumes and smoking cessation rates. This indicates that community pharmacies can serve as effective locations for implementing community-based public health initiatives focused on smoking cessation. 29 The findings of our study indicate a significant correlation between participants’ knowledge and their educational level, which is a logical conclusion. Additionally, a notable association exists between attendance at educational programs and improvements in both knowledge and attitude, with p values of 0.002 and 0.003, respectively. This suggests that as participants engage more in educational programs, their knowledge and attitudes demonstrate marked enhancement. The limitations of our study were not confined to acknowledging potential biases, including self-report bias and the nonrandom sampling method. Additionally, the cross-sectional design restricted our ability to infer causality. Furthermore, the geographic limitation, as the study was conducted in only five provinces, has implications for the national generalizability of our findings. In other words, the wide CI may indicate the need for larger samples in future research.
Conclusion
In conclusion, there exists a critical gap in the landscape of addiction studies in Iraq, coupled with the absence of specialized clinics dedicated to helping individuals quit smoking and overcome addiction. A considerable proportion of study participants, specifically 49.7%, perceive nicotine addiction to be as serious an issue as drug addiction. Regrettably, 61.3% of the participants believe that smoking counseling is an ineffective use of time and resources. These challenges are largely neglected within the country, which reflects a broader indifference toward health issues that necessitate comprehensive treatment, rigorous research, and effective evaluation. Addressing these issues is essential for improving public health and supporting those in need. In addition, the incorporation of NRT training into pharmacy education, along with the implementation of the World Health Organization’s MPOWER initiatives for pharmacist certification, can serve as effective strategies for addressing this issue.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251368246 – Supplemental material for Pharmacist knowledge, attitude, and practice regarding nicotine replacement therapy usage in Iraq
Supplemental material, sj-docx-1-smo-10.1177_20503121251368246 for Pharmacist knowledge, attitude, and practice regarding nicotine replacement therapy usage in Iraq by Khansaa A. Ibrahim Albaroodi in SAGE Open Medicine
Footnotes
Acknowledgements
The author thanks all the pharmacists who participated in and facilitated our work.
Ethical considerations
This study was approved by the Institutional Review Board of Al-Zahrawi University College (ZUC 012 on January 6, 2023). All methods followed relevant guidelines and regulations in compliance with the STROBE Statement.
Consent to participate
All participants agreed to participate and signed an informed consent form upon participation in the study.
Author contributions
Khansaa A. Ibrahim Albaroodi set the study design, data collection, data analyses, reporting results, preparing the article, and reading and approving the final article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
This article file includes all data generated during this study; raw data is available upon request.
Data access statement
The author had complete access to the study data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.