
Abstract
Background:
We sought to clarify possibly modifiable risk factors related to pollution responsible for acute bronchiolitis in hospitalized infants.
Methods:
For this observational study, we recruited 213 consecutive infants with bronchiolitis (cases: median age: 2 months; age range: 0.5–12 months; boys: 55.4%) and 213 children aged <3 years (controls: median age: 12 months; age range: 0.5–36 months; boys: 54.5%) with a negative medical history for lower respiratory tract diseases hospitalized at ‘Sapienza’ University Rome and IRCCS Bambino Gesù Hospital. Infants’ parents completed a standardized 53-item questionnaire seeking information on social-demographic and clinical characteristics, indoor pollution, eating habits and outdoor air pollution. Multivariate logistic regression analyses were run to assess the independent effect of risk factors, accounting for confounders and effect modifiers.
Results:
In the 213 hospitalized infants the questionnaire identified the following risk factors for acute bronchiolitis: breastfeeding ⩾3 months (OR: 2.1, 95% confidence interval [CI]: 1.2–3.6), presence of older siblings (OR: 2.8, 95% CI: 1.7–4.7), ⩾4 cohabitants (OR: 1.5, 95% CI: 1.1–2.1), and using seed oil for cooking (OR: 1.7, 95% CI: 1.2–2.6). Having renovated their home in the past 12 months and concurrently being exposed daily to smoking, involving more than 11 cigarettes and two or more smoking cohabitants, were more frequent factors in cases than in controls (p = 0.021 and 0.05), whereas self-estimated proximity to road and traffic was similar in the two groups.
Conclusions:
We identified several risk factors for acute bronchiolitis related to indoor and outdoor pollution, including inhaling cooking oil fumes. Having this information would help public health authorities draw up effective preventive measures – for example, teach mothers to avoid handling their child when they have a cold and eliminate exposure to second-hand tobacco smoke.
Introduction
Bronchiolitis, mainly caused by respiratory syncytial virus (RSV), is the first acute lower respiratory tract infection in infants <12 months of age.1,2 Each year 150 million new cases of bronchiolitis are reported worldwide, and 2–3% of affected infants require hospitalization. Long-standing evidence also underlines the risk of subsequent wheezing bronchitis and asthma. 3
Emerging evidence includes exposure to air pollution among possible trigger factors for pulmonary diseases.4–15 Although many studies recognize the importance of early environmental exposures in the development of asthma,4,11,13 few have investigated exposure to air pollution as a risk factor for bronchiolitis.16–20 Having this information would help public health authorities draw up effective measures for preventing bronchiolitis.
In this case-control study, we investigated whether exposure to various indoor and outdoor pollutants was associated with acute bronchiolitis in hospitalized Italian infants, and sought to identify modifiable risk factors.
Methods
Subjects
The survey was conducted from November 2012 to September 2014 at ‘Sapienza’ University Rome and IRCCS Bambino Gesù Hospital in a specialty care setting. For this case-control study, we enrolled all consecutive infants hospitalized for bronchiolitis over the 2 years and an equal number of controls: 213 children with bronchiolitis (cases: median age: 2 months; range: 0.5–12 months; boys: 55.4%); and 213 children aged <3 years (controls: median age: 12 months; range: 0.5–36 months; boys: 54.5%) hospitalized for various reasons other than respiratory infections (hydrocele, inguinal hernia, phimosis, febrile seizures, constipation).
Bronchiolitis was defined as the first episode of acute lower respiratory tract infection characterized by the presence of auscultator crackles, in infants aged ⩽12 months. 2 Inclusion criteria for cases were a diagnosis of bronchiolitis, without neonatal respiratory disorders or other chronic diseases. Inclusion criteria for controls were no respiratory diseases, and a medical history negative for lower respiratory tract diseases and neonatal respiratory disorders.
Exposure and clinical factors
At enrolment, after giving written informed consent, parents or legally authorized tutors for each child in both groups were asked to complete a standardized, self-reported questionnaire that was adapted from the ‘Questionnaire on respiratory and allergic health of pupils and on the domestic environment in which they live’ (www.salute.gov.it/imgs/C_17_pubblicazioni_1892_allegato.pdf). The questionnaire comprised 53 items, seeking information on social-demographic and clinical characteristics, indoor pollution, eating habits and outdoor air pollution (additional file 1). The crowding index was calculated as follows: number of cohabitants/number of rooms in the house. To evaluate the role of breastfeeding in two populations differing in age, we reported the mean breastfeeding duration together with the percentage of children breastfed for at least 3 months, or for younger infants the entire lifetime. In families with smoking exposure, to analyse whether the amount of smoking exposure had an additive effect on the development of bronchiolitis, we defined high domestic smoke exposure as being simultaneously exposed to smoking in the house every day, with ⩾11 smoked cigarettes and ⩾2 smoking cohabitants. Parents reported whether their house was located in an unpolluted area far from busy roads (considered as unpolluted areas) or in an area with little traffic or near intense traffic (considered as polluted areas).
Statistical analysis
A descriptive analysis included calculating percentages, mean (SD) and median (range) for variables. Differences between cases and controls were tested for significance using an unpaired t test (two-tailed) for normally distributed data or nonparametric Mann–Whitney test for non-normally distributed data. The chi-squared test was applied to analyse categorical independent variables.
We ran a multiple regression analysis to evaluate how all covariates combined influenced the probability of infants having bronchiolitis. As potential predictors, we used our subjects’ social-demographic and clinical characteristics, indoor pollution, eating habits and outdoor air pollution. In the multiple regression analysis including data only for subjects for whom all information was recorded, the sample size diminished from 426 to 184 observations. According to the standard missing data taxonomy, we assumed that the missing data mechanism was at random and therefore applied multiple imputation procedures. We ran the expectation-maximization (EM) algorithm implemented in the ‘Amelia’ package in R Statistical Software (www.R-project.org). 21 We ran the algorithm until convergence and estimated 300 imputed datasets. A multiple logistic regression model was fit for each imputed dataset and a model averaging procedure was applied to summarize the results.
The study was approved by the research and ethics committee at the Hospital Policlinico ‘Umberto I’, Rome, Italy.
Results
Parents of 213/248 cases (85.9%) and 213/265 controls (80.3%) completed the questionnaire. The main reasons for not answering were the lengthy questionnaire or linguistic problems. In 71.6% of cases and 72.5% of controls, the mother completed the questionnaire. No difference was found for compliance between cases and controls.
Clinical variables
In agreement with the inclusion criteria, the 213 cases were younger than the 213 controls enrolled. The percentage of Caucasians was significantly lower in cases than in controls. Cases and controls were homogeneous for gender, parents’ age, percentage of preterm infants, of twin pregnancy and birth weight. The percentage of children breastfed was similar in cases and controls (80.1% and 73%), but the percentage of children breastfed for at least 3 months was higher in cases than in controls (p < 0.0001, by chi-square test).
The percentage of smoking mothers as well as the number of cigarettes smoked and exposure to smoke during the first 12 months were higher, though not significantly, in cases than in controls. Most cases had older siblings (p < 0.0001). The presence of eczema in the family was higher in cases than in controls (p = 0.047), whereas a family history of asthma and of allergic rhinitis were similar. Controls had suffered more frequently than cases from eczema and otitis (p = 0.013 and p < 0.0001). Among socioeconomic variables, no significant differences were found between the two groups. Almost one
Clinical and socioeconomic characteristics in cases and controls.

Cases, infants hospitalized for bronchiolitis; controls, control children.
p by chi-square test; * = by t test; ns = not significant.
Indoor pollution
Answers to the questionnaire showed that the percentage of children with houses built before 1990 was higher in cases than in controls (p = 0.031). Most children in both groups lived in apartments. The mean number of rooms in the house was similar in cases and controls. The mean number of cohabitants was higher in cases than in controls (p < 0.0001). The crowding index (number of cohabitants/numbers of rooms in the house) was higher in cases than in controls (p = 0.006). Having renovated their home in the past 12 months was a more frequent finding in cases than in controls (p = 0.021). Having a pet dog in the house was similar, whereas having a cat was less frequent in cases than in controls (p = 0.007). No significant differences were found between the two groups for humidifiers, air conditioners, dampness or mould in the child’s room, dampness or condensation on the windows, garage connected to the house, cockroaches in the house, fireplace in the house, or use of air fresheners. In both groups, children’s rooms were most commonly floored with tiles. The percentage of smoking exposure was significantly lower in cases than in controls. No difference was found in the two groups of children for cigarettes smoked and presence of smoking cohabitants. Among smoking families, the simultaneous presence of daily smoking exposure, ⩾11 cigarettes and ⩾2 smoking cohabitants was higher in cases than in controls (p = 0.05) (Table 2). No significant differences were found between the two groups for having a fume hood, cooking methods, or using olive oil and margarine. Using butter and seed oil for cooking was significantly higher in cases than in controls (p = 0.001) (Table 3).
Data on indoor pollution in the two groups, cases and controls.
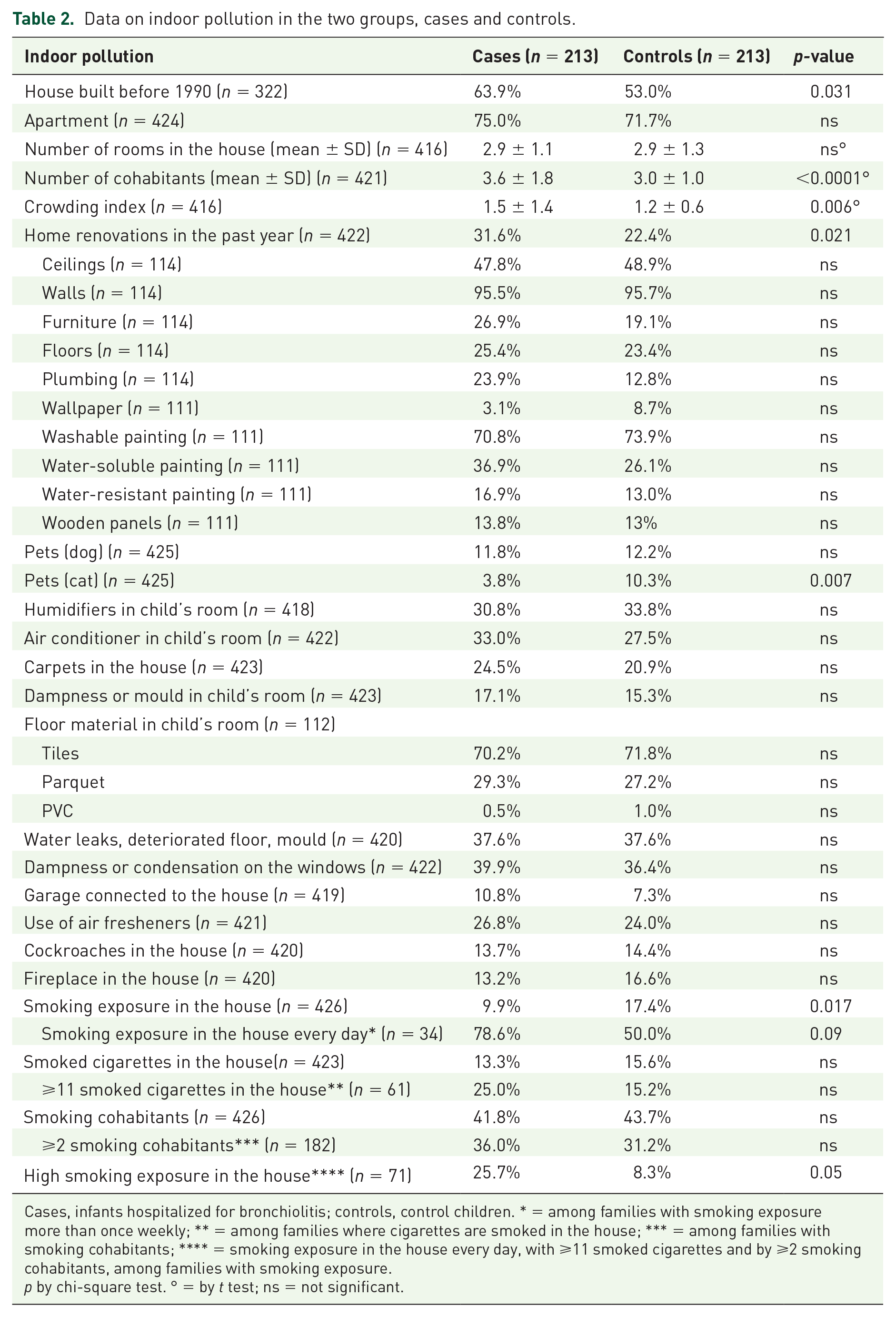
Cases, infants hospitalized for bronchiolitis; controls, control children. * = among families with smoking exposure more than once weekly; ** = among families where cigarettes are smoked in the house; *** = among families with smoking cohabitants; **** = smoking exposure in the house every day, with ⩾11 smoked cigarettes and by ⩾2 smoking cohabitants, among families with smoking exposure.
p by chi-square test. ° = by t test; ns = not significant.
Indoor pollution (cooking habits) in the two groups, cases and controls.
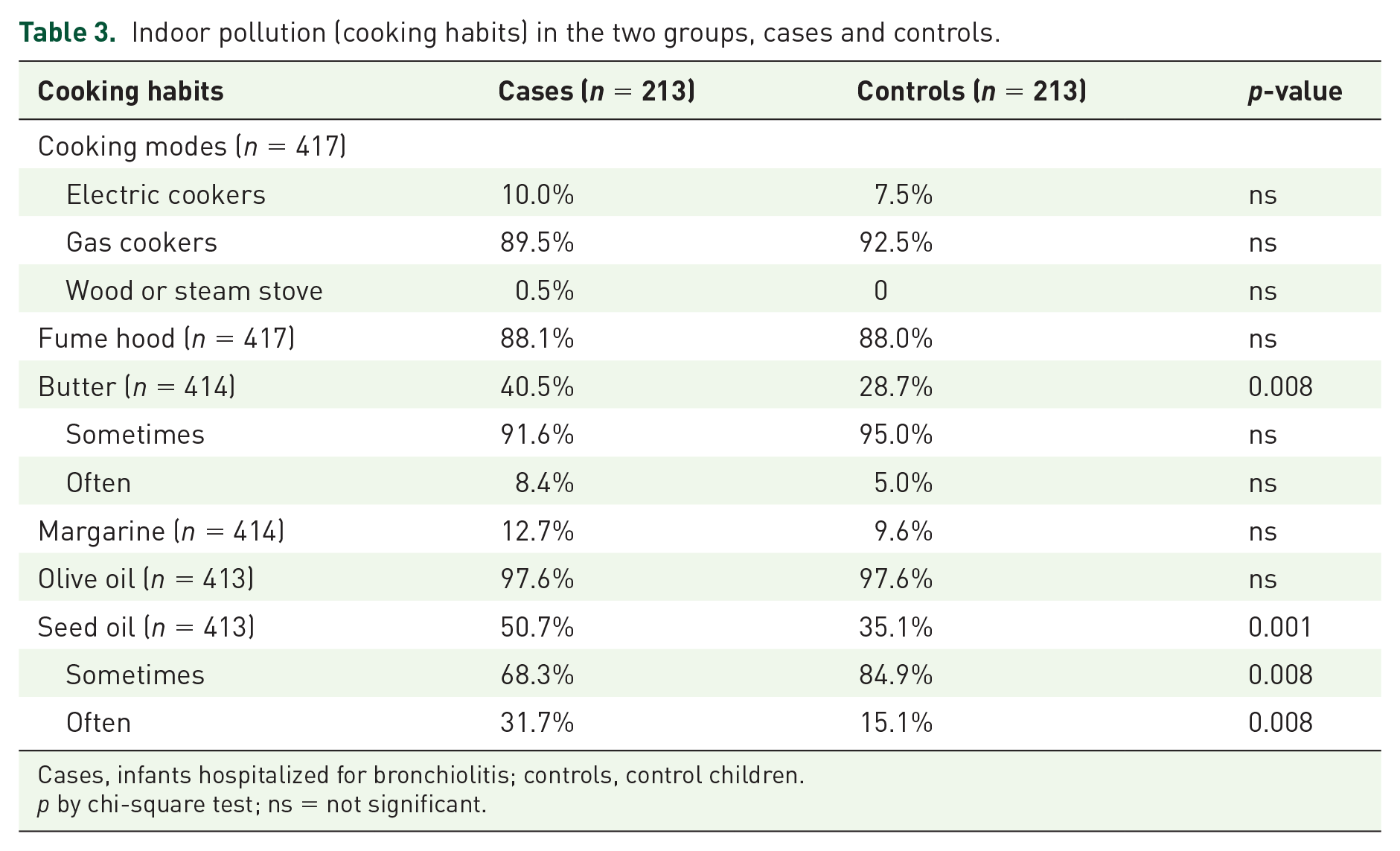
Cases, infants hospitalized for bronchiolitis; controls, control children.
p by chi-square test; ns = not significant.
Outdoor air pollution
No differences were found between the two groups for location of the house (Table 4).
Data on outdoor air pollution in the two groups, cases and controls.

Cases, infants hospitalized for bronchiolitis; controls, control children.
p by chi-square test; ns = not significant.
Multivariate logistic regression analysis
The multivariate logistic regression analysis run in the 184 children with all observations confirmed the results obtained with the simple logistic regression model. The analysis accounting for the effect of age identified as a risk factor for bronchiolitis having older siblings (OR: 2.393; 95% CI: [1.231; 4.651]) and using seed oil for cooking (OR: 1.82; 95% CI: [1.206; 2.741]).
The sensitivity analysis including only a subsample of children younger than 6 months also identified as a significant risk factor for bronchiolitis having older siblings (OR: 2.242; 95% CI: [1.248; 4.026]) but eczema in the family as well as numerous cohabitants increased the probability of having bronchiolitis (OR: 2.868; 90% CI: [2.098; 3.639] and OR: 1.748; 90% CI: [1.364; 2.132]).
Discussion
Our 2-year case-control study conducted in two Italian paediatric centres underlines the close association between exposure to various indoor and outdoor pollutants and acute bronchiolitis in hospitalized Italian infants. We also suggest possibly modifiable risk factors for infant bronchiolitis.
When we analysed our infants’ case histories, we found no factor associated with a higher risk for bronchiolitis. For example, neither mothers’ age nor socioeconomic status differed between the two groups. Previous studies identified both variables as risk factors for bronchiolitis, possibly because disadvantaged mothers had less access to health care services.18,20 In our series we found that both variables were homogeneously distributed in both groups, possibly because everyone in Italy has a right to hospital admission regardless of socioeconomic status.
Among the clinical characteristics we analysed, the first risk factor for bronchiolitis was having older siblings. Older siblings, who are always schooled, are a major vehicle for transmitting viral infections.2,18,20 For this reason, limiting young children’s exposure to cohabitants’ oral secretions may be a valid intervention for preventing bronchiolitis.
An unexpected finding that is difficult to explain was that breastfeeding was more frequent among cases than controls. This difference contrasts with findings in other studies showing that breastfeeding reduces the risk of hospitalization for bronchiolitis, 22 as well as the risk of severe bronchiolitis forms developing, often requiring hospitalization in intensive care units. 2 Given the well-known importance of maternal antibody transfer to infants, 23 we conjecture that our results might reflect mother-to-child transmission of respiratory infection during breastfeeding. As measures to reduce the risk of virus transmission, we always strongly encourage breastfeeding also beyond 3 months of age, and recommend that ill mothers use a mask and wash their hands before handling the child.
When we analysed questionnaire answers referring to indoor pollution, our data showed that the most important risk factor for bronchiolitis was a high number of cohabitants. This finding confirms the previously reported association between crowding and respiratory infections, 7 underlining recommendations to reduce crowding at home as well as in day-care centres.
Other factors we found associated with a higher risk of bronchiolitis were living in an older house or having a recently renovated home. These domestic factors suggest that some indoor pollutants in older houses as well as some materials used for renovations may act as lower airway irritants. The association between house renovation and risk of bronchiolitis may depend on volatile organic compounds. 24 Viruses causing bronchiolitis, particularly RSV, are more stable at cold temperatures. Cold temperatures also drive populations indoors, where they are exposed to indoor pollution sources as well as to outdoor pollutants that have penetrated the building. 12 Consequently, during the winter, the season when respiratory viruses often circulate, and infants spend most of the time at home, they are more exposed to pathogens as well as to indoor air pollution.
Another finding that is difficult to explain is the slightly higher tobacco smoke exposure during pregnancy and neonatal life in infants with bronchiolitis than in controls, and the higher smoking exposure in the house in controls than in bronchiolitis infants. These findings may reflect the fact that parents of children with respiratory diseases tend to underreport their own smoking habits. Ample evidence shows that second-hand tobacco smoke in children decreases lung function and increases airway responsiveness, thus possibly predisposing infants to more severe infections. 8 Equally important, convincing evidence suggests that smoking during pregnancy is itself associated with bronchiolitis. 18 When we analysed questionnaire data only for families with smoking habits, we found that high smoke exposure, as measured by smoking frequency, number of cigarettes and number of smoking cohabitants, was significantly higher in infants with bronchiolitis than in controls (p = 0.05). These differences suggest that the amount of smoking exposure has an additive effect on the development of bronchiolitis.
Another variable we studied, having pet cats in the house, seems to protect infants from bronchiolitis. Others report that contact with pets either increases the risk of allergic diseases or induces sensitization or protects against them, or has no association at all.4,5 To our knowledge, no studies have yet correlated pet exposure and bronchiolitis.
In our study, questionnaire answers referring to fats used for cooking showed that families of infants with bronchiolitis used butter and seed oil for cooking more often than did controls. A possible explanation is that children often inhale fumes from overheated butter and oil used for cooking. Exposure is particularly high among women and young children, who spend a long time in the kitchen. 15 For example, a substance released by butter during cooking, diacetyl (2,3butanedione), caused bronchiolitis obliterans in workers who inhaled this volatile butter flavouring in high amounts. 25 Oil fume extracts collected from heated edible oils can also cause lung cell cytotoxicity and genotoxicity. 26 Exposure to fumes from combusted cooking fats is a possible cause of dyspnoea and short-term reduction in spirometric values. 15
Among environmental factors that are presumably hard or impossible to modify, the infants with bronchiolitis we studied frequently, though not significantly more frequently, lived in houses located in highly polluted areas. Epidemiological studies show that exposure to vehicular traffic increases the prevalence of bronchitis and can exacerbate pre-existing asthma, especially in children, because of their developing lungs, immature metabolic pathways, increased time exercising outdoors and high ventilation rates per body weight.10,19 We also suggest whenever possible taking children to parks and open spaces far from highly polluted areas.
A possible limitation in our study is that because we used self-reported data we cannot verify whether parents answered the questionnaire truthfully. Another limitation is that because the interviewed parent reported only the child’s age in years, we could not evaluate the season of birth. Hence, being unable to compare the month of birth in the two groups possibly biased these results. Finally, we could not consider the additional role of the child’s extra-family contacts with infected individuals, possible viral infection carriers, who come to visit newborns.
In conclusion, our self-reported questionnaire identified several risk factors for acute bronchiolitis related to indoor and outdoor pollution. A new risk factor we identified was inhaling cooking oil fumes. Several changes, mainly in the mother’s behaviour towards their children, might reduce the risk of bronchiolitis eventually developing. Mothers should, for example, avoid allowing the child to come into contact with siblings’ oral secretions, use a facial mask during feeding and try not to handle the child when they are ill. Anyone in contact with children should eliminate exposure to tobacco smoke, avoid letting children inhale cooking oil fumes and regularly take children to parks and open spaces far from highly polluted areas. From a public health perspective, our findings might help public health authorities draw up guidelines related to indoor and outdoor pollution that would help reduce acute bronchiolitis in infants.
Footnotes
Acknowledgements
The authors thank Prof. Giovanni Viegi for his critical review of the paper and Alice Crossman for language revision.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplementary Material
Supplementary material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.