
Abstract
Introduction
Lower respiratory tract infections, particularly bronchiolitis, commonly cause hospitalisation in infants younger than 24 months. 1 Bronchiolitis is usually preceded by a viral upper respiratory tract infection (rhinorrhea) and progresses to tachypnoea, dyspnoea (working ala nasi, intercostal retraction, subcostal retraction, grunting, and cyanosis), and auscultation. 2 The respiratory syncytial virus is the leading cause of bronchiolitis in developed countries. The diagnosis was made based on history and clinical examination. 1 Treatment consists mainly of oxygen therapy, 3 adequate hydration, and nasopharyngeal suctioning as needed. Additionally, inhalation of hypertonic saline combined with nebulisation of racemic epinephrine may be beneficial for hospitalised patients. Bronchodilators have been found to be ineffective in treating bronchiolitis because they do not reduce hospitalisation time. Corticosteroids and antibiotics are not recommended as regular treatments for bronchiolitis. They can be used in outpatients, severe cases, and patients with asthma. 4 The risk of severe outcomes due to viral infection increases in infants younger than 2 months. (Bacterial bronchiolitis is a bacterial infection that occurs on top of a viral bronchiolitis). Blood culture is the gold standard for the diagnosis of bacterial infections. Contamination, antibiotic use before sampling, low bacteraemia, and insufficient sampling volume influence blood culture accuracy (varies from 8% to 73%) in detecting bacteria. 5 Additionally, the turnaround time for blood culture results is at least 48–72 h, resulting in false-negative reporting and delays in diagnosis. 6 This necessitates the search for reliable and rapid markers for the diagnosis of bacterial infections. FC gamma receptor1 (FcγR1) is designated as a CD64 molecule that is normally present on the surface of monocytes under normal conditions. 7 Studies have shown that CD64 expression on the surface of neutrophils increases during possible bacterial infections and inflammatory conditions, and its value increases 5–10 times the normal value in 1–6 h. 8 Procalcitonin (PCT) is an acute-phase protein normally synthesised and secreted by thyroid follicular cells. Procalcitonin levels increase (within 3–4 h after infection and peak at 6–8 h for at least 24 h) in response to bacterial endotoxins that trigger an inflammatory response during infection. This is in contrast to C-reactive protein (CRP), which increases 24–48 h after bacterial infection. 9 Antibiotic use can affect procalcitonin levels. 10 This is the first study to investigate the use of CD64 in assessing for bacterial infection in bronchiolitis.
Methodology
This prospective observational study was conducted at a university children’s hospital from 12–2019 to 2–2020.
Patients younger than 2 years who were clinically diagnosed with bronchiolitis (patients younger than 2 years who presented with wheezing and lower respiratory tract infection without other causes of wheezing) had blood samples (on the first day of admission) and a chest X-ray. The radiological criterion for diagnosis was hyperinflation without pneumonic patches or aspiration. Demographic data, clinical examinations, and antibiotic therapy results were recorded. CBC, blood culture, procalcitonin, and CD64 surface expression were performed on granulocytes by flow cytometry (the cost of the CD64 surface expression test per sample was 14$). The hospitalisation criteria were as follows: SPO2 <90% in room air, respiratory distress according to the Wood-Downes clinical scoring system modified by Ferres 11 : score >4, which was not relieved by oxygen therapy. Patients with possible bacterial infection met two of the following criteria: procalcitonin level >0.5 ng/dl, total WBCs count >15,000/mm3, or neutrophil count >12,000/mm3. 12 Laboratory diagnosis of infection still depends on diagnostic markers that have been available since 1970s or before, such as total leukocyte counts, neutrophil counts, the presence of myeloid-immature forms in the peripheral blood, and laboratory markers for acute-phase reactants such as C-reactive protein (CRP). And recently, developing new-generation and improved diagnosis for infection has been directed towards markers in the serum or plasma, such as procalcitonin (PCT). Patients with other causes of respiratory distress were excluded from the study. We also evaluated CBC, procalcitonin, and CD64 granulocyte levels in healthy controls (Healthy relatives of the patients; either brothers or sisters of the patients) of the same age and sex. CBC was performed using Micros 60 (HORIBA Medical). Serum procalcitonin (PCT) levels were measured by chemiluminescence using the ADVIA Centaur® XPT immunoassay system. Blood cultures were obtained from all the patients. Sample collection: Peripheral venous blood (5 mL) was collected from each subject and divided into 2 mL EDTA for CBC and flow cytometry. In addition, 3 mL in a Wasserman tube was centrifuged at 2000–3000 rpm for 20 min. The serum was used for the procalcitonin assay. A separate sample was collected in BacT/ALERT paediatric bottles (BioMerieux) and processed using a BacT/ALERT 3D instrument. Growth was evaluated twice on day two and once daily on days three, five, and seven. Samples with clinically significant growth indices were Gram stained and inoculated onto a culture medium according to the Gram stain morphology of the organism. Plates were incubated and growth was determined using routine bacteriological methods. The study was carried out after obtaining the permission of the Ethical Committee of Scientific Research, Faculty of Medicine, University with IRB no17300492. Written informed consent was taken from the parents of the patients and controls for participation in the study.
Procalcitonin (REF 10378883, USA): Principle of the assay
The kit was used to quantify procalcitonin content in the sample by a one-step chemiluminescence immunoassay using three monoclonal antibodies (sandwich principle). The ADVIA Centaur BRAHMS PCT assay is a 20 min antibody sandwich immunoassay in which the solid phase contains monoclonal antibodies against fluorescein covalently bound to paramagnetic particles. The ancillary reagent contains two antibodies against procalcitonin, labelled with fluorescein (detection range: 0.02–75 ng/mL).
Surface CD64
Flow cytometric analysis was carried out on EDTA peripheral blood specimens withdrawn and analyzed in less than 48 h of sample collection time (we measured surface CD64 once during 48 h of the patient’s admission); the test was performed using the Leuko64 assay (Leuko64 kit, Trillium Diagnostics, Beckman Coulter, USA). Data analysis was conducted using a Becton Dickinson FACScan system. The compensation setting was performed using colour-calibrated beads (BD Biosciences). First, we adjusted the sample count for analysis and acquired unstained samples to detect autofluorescence. Isotype controls, mouse Immunoglobulin G (IgG) peridinin-chlorophyll-protein complex (PerCP) control, and IgG1 fluorescein isothiocyanate (FITC) controls were then obtained from BD Biosciences for the setting of nonspecific binding. For each sample, 50 μL of blood was stained with FITC-conjugated anti-human CD64 (Immunotech, Beckman Coulter, Marseille, France) and PerCP conjugated anti-human CD45 (BD Biosciences). After 15 min of incubation in the dark, the samples were washed, centrifuged, and lysed using a BD FACS Lyse (BD Biosciences). (The samples were washed and suspended in 200 μL FACS buffer (BD Biosciences). For gating, using CD45 and side scatter (CD45/SS), we first gated the neutrophil area in the dot plot graph for CD64. Data are shown as percentage (%) and mean fluorescence intensity (MFI) using a single histogram.
Statistical analysis
Data entry and analyses were performed using SPSS version 22 (Statistical Package for Social Science). Data are presented as numbers, percentages, medians, ranges, means, or standard deviations. The chi-square test was used to compare the qualitative variables. The Mann–Whitney U test was used to compare quantitative variables between the two groups, and the Kruskal–Wallis test was used for more than two groups. Spearman’s correlation was used to measure the correlation between quantitative variables in the case of non-parametric data. The MedCalc program was used to calculate the sensitivity, specificity, positive and negative predictive values, and ROC curves. Statistical significance was set at p < 0.05.
Results
This prospective observational study was conducted at a university children’s hospital from 12 January 2019 to 2 January 2020. Sixty-two patients with lower respiratory tract infections diagnosed clinically and by chest radiographs showing bronchiolitis were enrolled. The median age (range) was 4.8 (1.5–18) months, and the mean weight ±SD was 6.79 ± 2.64 kg. Forty-four men and 18 women participated in the study. According to the Wood–Downes clinical scoring system modified by Ferres, 11 54 cases were grade 5, six were grade 7, and two were grade 8. Radiography was performed in 62 cases, and atelectasis and infiltration were found in eight cases. The patients were divided into 34 cases with non-bacterial infection and 28 with possible bacterial infection. The patients who met two or more of the following criteria were included in the PBI group:
Demographic characteristics of the patients and control group.
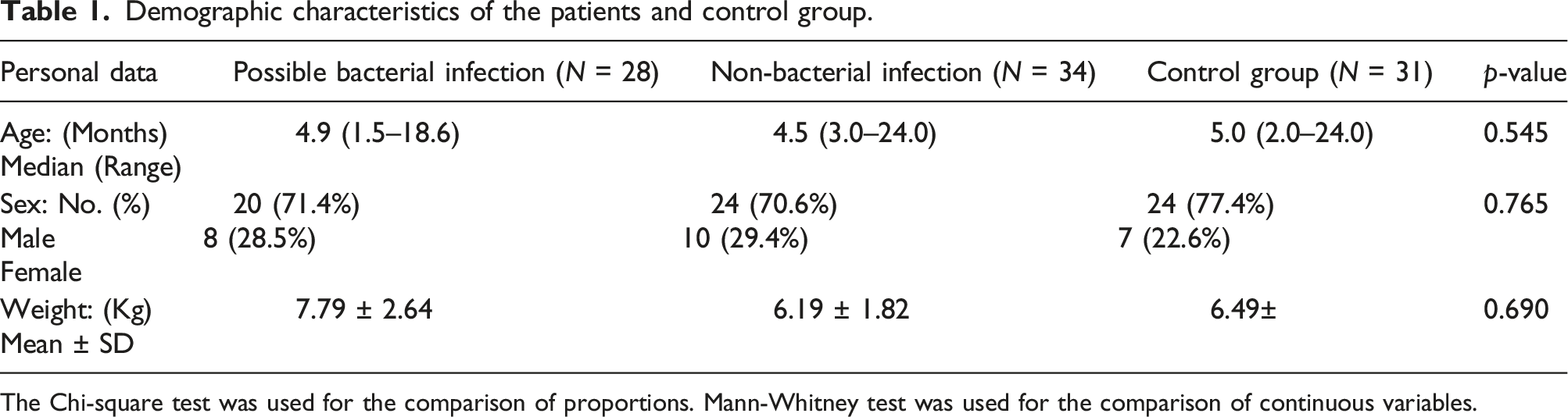
The Chi-square test was used for the comparison of proportions. Mann-Whitney test was used for the comparison of continuous variables.
Mean values and standard deviation of the classical biomarkers and leucocytes CD64 expression in different groups.

P1: significance between the 1st and the 2nd group.P2: significance between the 1st and 3rd group. P3 significance between the 2nd and 3rd group, p < 0.05 is significant.
mCD64, monocytes CD64 mean fluorescence intensity; nCD64, neutrophils CD64 mean fluorescence intensity, %CD64+ neutrophils, CD64 positive neutrophils percentage.
Correlation between classical biomarkers and CD64 expression.

PCT, procalcitonin; mCD64, monocytes CD64 mean fluorescence intensity; nCD64, neutrophils CD64 mean fluorescence intensity %CD64+ neutrophils, CD64 positive neutrophils percentage.
Correlations between CD64 expression in neutrophils and monocytes.

mCD64, monocytes CD64 mean fluorescence intensity; nCD64, neutrophils CD64 mean fluorescence intensity, %CD64+ neutrophils, CD64 positive neutrophils percentage.
Sensitivity, specificity, PPV, and NPV of markers using cutoff value for diagnosis of bacterial infection.

PCT, procalcitonin; mCD64, monocytes CD64 mean fluorescence intensity; nCD64, neutrophils CD64 mean fluorescence intensity, %CD64+ neutrophils, CD64 positive neutrophils percentage. PPV, positive predictive value; NPV, negative predictive value; AUC, area under the receiver-operating characteristic curve.
Discussion
This study investigated CD64 surface expression patterns in monocytes and neutrophils in children with acute bronchiolitis. We detected a correlation between the expression of CD64 and the traditional markers used to detect PBI. Based on the results, we can better assess the positive and negative predictive value of nCD64 and mCD64 in predicting PBI in bronchiolitis.
Bacterial superinfection is the most significant complication of bronchiolitis in children. 12 Previously, there were no suitable markers to precisely determine when children were superinfected. 13 To identify the risk of bacterial infection, physicians generally base their diagnosis on symptoms and signs, in addition to laboratory markers and chest radiographic findings. 14 Except for procalcitonin, 13 none of these laboratory markers has revealed the ability to distinguish between the presence or absence of bacterial superinfection. The study of CD64 expression in bacterial infections 15 is currently of great research interest.16,17,18 It is a high-affinity receptor expressed in neutrophils and monocytes and has been reported as a helpful marker of suspected bacterial superinfection in cases where the old markers do not provide accurate results. Therefore, it has been investigated in mechanical ventilation pneumonia, mortality in the intensive care unit, and bacterial infections in patients with autoimmune diseases. 19 Changes in its expression in suspected bacterial superinfection could help reduce antibiotic use. In this study, we described the expression of CD64 in neutrophils and monocytes by grouping patients according to the PBI. Both nCD64 and mCD64 levels showed statistically significant differences. 17 In monocytes, where CD64 was expressed, the percentage of CD64 cells did not change, increasing the surface expression measured by MFI. The MFI and positive neutrophil percentage increased in parallel. Recently, CRP and PCT levels have been used for early diagnosis of bacterial infections. 20 PCT was positively correlated with nCD64, mCD64, and the percentage of positive neutrophils. 19 CRP and mCD64 levels have also been used for early diagnosis of bacterial superinfections.
During PICU admission, antibiotic initiation is mainly influenced by clinical signs and diagnostic markers.21,22 Therefore, the exploration of new diagnostic tools to improve the choice of antibiotic therapy is crucial. When considered individually, neutrophil count, CRP, and PCT21,22 do not have high specificity or sensitivity and are generally more useful when studied together. 19 The use of CD64 as a marker of bacterial infection has increased recently. 21 nCD64 is expressed at a very early stage in the host immune response to bacterial infections. It is upregulated within 4–6 h of bacterial infection. Currently, CD64 expression can be rapidly and accurately measured using flow cytometry. The main problem is that there are no suitable cutoff values. 21 زWe found that the sensitivity and specificity results of previous studies vary widely and that our results are similar to those of some studies while they differ significantly from others. For example, our nCd64 sensitivity and specificity were 94% and 73%, respectively, whereas Bernard et al. 23 reported nCd64 sensitivity and specificity of 94.7% and 46.5%, respectively, and Alberto et al. 24 reported sensitivity and specificity of 74% and 90%, respectively.
Conclusion
This study demonstrated that neutrophil and monocyte CD64 expression increases in bacterial infections and deserves further evaluation in the early detection of bacterial infections in bronchiolitis.
Footnotes
Acknowledgements
To the parents of the patients for their participation in the study. To the residents, assistant lecturer, and nursing staff in the emergency unit.
Author contribution
Amira M Shalaby-Patient examination, data collection, result interpretation, and manuscript writing.
Yasser Farook, Safwat M Abdel-Aziz-Examined the Patient examination, data collection supervision, and data interpretation assistance.
Marwa M Thabet-Performed the flow cytometric analysis of samples.
Abeer A Mokhtar-Performed clinical pathology and laboratory work.
Dalia A Nigm, Azza A Fadle-Result interpretation and revision of the whole work.
Asmaa M Ismail-Study design, data collection supervision, result interpretation, and revision of the whole work
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The study was carried out after obtaining the permission of the Ethical Committee of Scientific Research, Faculty of Medicine, Assiut University with IRB no17300492
Informed consent
Written informed consent was taken from the parents of the patients and controls for participation in the study. The study was approved by the Head of Assiut University Children’s Hospital and the Head of the Emergency Unit where the study was carried out