
Abstract
Pulmonary arterial hypertension (PAH) is a progressively fatal disease, and the goal in treatment is to prevent disease progression. The standard of care often involves medications from multiple therapeutic classes, and there has been significant interest both in the choice of agent as well as the timing of initiation. There is a growing body of support for starting multiple medications at the time of diagnosis, or ‘upfront ’, rather than using sequential addition to prevent clinical deterioration.
Keywords
Introduction
Pulmonary arterial hypertension (PAH) is a disease entity caused by an increase in pulmonary vascular resistance defined as a mean pulmonary arterial pressure ⩾25 mmHg at rest, in which there is no evidence of elevated pressures distal to the pulmonary arterioles [Galiè et al. 2015a]. Initially oral treatment was limited to only those who showed evidence of response to calcium-channel blockers [Rich et al. 1992], but in recent years therapies have focused on more disease-specific therapies, including prostacyclins [Barst et al. 1996] and selective prostacyclin receptor agonists [Sitbon et al. 2015], endothelin receptor antagonists (ERAs) [Rubin et al. 2002; Galiè et al. 2008], soluble guanylate cyclase stimulators [Ghofrani et al. 2013] and phosphodiesterase inhibitors (PDEis) [Galiè et al. 2005, 2009]. Trials have progressively demonstrated the ability of the aforementioned medications to temporarily inhibit disease progression, frequently measured by the delay of decompensating events. However, until recently, these therapies were only tested among those who had advanced disease. As of late, those with newly diagnosed disease and New York Heart Association (NYHA) class II symptoms have been more adequately represented in trials, and the early results are encouraging.
Growth of targeted therapies
For decades after it was recognized as a disease entity, PAH therapy was restricted to supportive measures and a high dose calcium channel blocker if a patient was deemed responsive to vasodilators during a right heart catheterization.
Prostacyclins, the first targeted therapy, were approved for use in 1995 [Barst, 2008]. Epoprostenol, the first drug in its class, did have a statistically significant effect on mortality [Barst et al. 1996]. Given its short half-life, it was initially available only by intravenous infusion requiring a cumbersome infusion setup, with inherent risks of line sepsis. Over the next decade, more chemically-stable prostacyclins were introduced allowing for easier methods of delivery. Most recently selexipag, an oral, highly-selective prostacyclin receptor agonist, demonstrated improvement in time to clinical worsening (TtCW) [Sitbon et al. 2015].
ERAs, piloted by bosentan in 2001, focused on an alternative target in the vasoconstrictive and hyperproliferative pathway. BREATHE-1 randomized 213 patients with class III or class IV symptoms to either placebo or bosentan for 12 weeks [Rubin et al. 2002]. The 6-minute walk distance (6MWD), Borg dyspnea index, and TtCW were all improved in the treatment group. In contrast with prostacyclins, the oral formulation made administration far easier.
Phosphodiesterase-5 (PDE5) inhibitors, which prolong the vasodilatory effects of nitric oxide’s second messenger cyclic guanosine monophosphate, were postulated to have utility in PAH by prolonging the effects of nitric oxide’s second messenger, which is known to be reduced in PAH. The SUPER trial [Galiè et al. 2005] enrolled 278 patients with NYHA functional class II or greater with World Health Organization (WHO) group 1 PAH and randomized to placebo or various doses of sildenafil for 12 weeks. While 6MWD was improved, there was no difference in TtCW (Table 1).
Randomized control trials with a primary or secondary endpoint of TtCW with positive results.
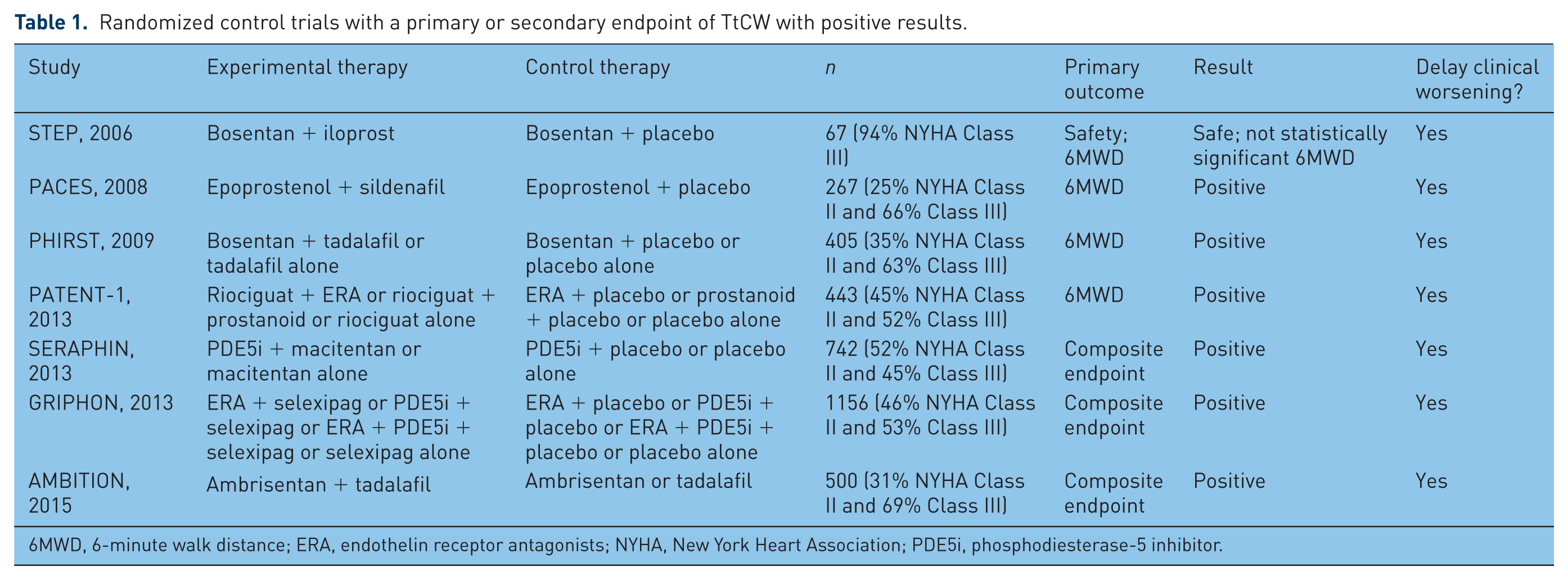
6MWD, 6-minute walk distance; ERA, endothelin receptor antagonists; NYHA, New York Heart Association; PDE5i, phosphodiesterase-5 inhibitor.
Initial trials were focused on showing the drug effect of the experimental agent and so the design of most trials excluded patients already on prostacyclins. Given the promising results of each therapeutic group, the question of combining these agents to achieve synergistic beneficial effects was raised.
Combination therapy in advanced disease: evolution of sequential therapy or add-on trials
In 2007, the first major trial which attempted to assess combination therapy studied the impact of adding inhaled iloprost to regimens of patients with primarily NYHA class III disease already on bosentan [McLaughlin et al. 2006]. A relatively small study, with only 67 patients enrolled, demonstrated a benefit in 6MWD of around 40 m.
It should be noted that the clinical utility of the 6MWD has been an issue of debate, with a recent meta-analysis raising doubts about the relationship between 6MWD and mortality and other long-term outcomes [Savarese et al. 2012]. Furthermore, investigators have shown in a chronic obstructive pulmonary disease cohort that patients will not notice any subjective improvement for distances <54 m [Redelmeier et al. 1997], which is less than the approximate 40 m improvement seen in the prior trials.
Given the low incidence of PAH and the difficulty of enrolling patients who met the widely-accepted inclusion criteria, powering studies for more traditional long-term objective outcomes was challenging. This put pressure on those designing studies to come up with a clinically meaningful endpoint which was also demonstrable in the few months’ duration of these trials. The solution appeared in the form of a composite endpoint, frequently including TtCW defined as the need for hospitalization, parenteral prostanoids, atrial septostomy, lung transplantation, or death.
The Task Force on Endpoints and Clinical Trial Design tried to clarify and standardize this variance and determined the following to be appropriate components for a meaningful composite endpoint of TtCW: (1) all-cause mortality; (2) nonelective hospital stay for PAH, including need for initiation of intravenous prostanoids, lung transplantation, or septostomy; (3) disease progression defined as 15% decrease in 6MWD plus worsening functional class or persistent class IV functional status [McLaughlin et al. 2009]. These conclusions were largely reaffirmed in 2013, with the addition of worsening of PAH symptoms (two out of four of the following: dyspnea, chest pain, syncope, or fatigue) [Gomberg-Maitland et al. 2013].
The PACES trial [Simmoneau et al. 2008] which came on the heels of STEP, compared the addition of sildenafil with those with PAH on intravenous epoprostenol alone which again showed an improved TtCW. TRIUMPH [McLaughlin et al. 2010], in 2010, looked at the addition of inhaled treprostinil to patients already on either bosentan or sildenafil. Again the 6MWD improved as it did with various other combination therapies in patients with severe disease, such as the addition of macitentan [Pulido et al. 2013] to baseline therapy in the SERAPHIN trial, which did show improvement in TtCW (Table 1).
This exploration of combination therapy spurred on by PACES was not all positive. Trials which explored adding oral treprostinil to an ERA or PDE5 inhibitor did not show an improvement in TtCW or 6MWD [Tapson et al. 2012]. Similarly, adding bosentan to sildenafil only improved N-terminal pro-brain natriuretic peptide (NT-pro BNP) levels without improvement in TtCW or even 6MWD in the COMPASS 2 trial [McLaughlin et al. 2015].
Upfront combination therapy
The next logical step in the progression of combination therapy was earlier initiation of dual targeted therapy in incident WHO group 1 PAH patients. While expert opinion had recommended upfront therapy for some time, AMBITION [Galiè et al. 2015b] was the first study to look at this in a randomized control format for patients newly diagnosed with PAH. Out of the 500 patients enrolled, one third were randomized to tadalafil alone, another third to ambrisentan only and the remaining patients received combination therapy with both ambrisentan and tadalafil. The group receiving both agents simultaneously fared better from the perspective of a composite clinical endpoint of death, hospitalization, initiation of parenteral prostanoid therapy, need for atrial septostomy or lung transplantation, or failure to have a satisfactory clinical response defined as 10% improvement in 6MWD, improvement to or maintenance of WHO functional class I or II, and no events of clinical worsening prior to or at week 24.
AMBITION’s promising results were buoyed by smaller-scale trials testing upfront therapy in different subgroups of patients with PAH. Treatment-naïve patients with PAH associated with scleroderma had improved pulmonary hemodynamics along with 6MWD at 32 weeks when compared with their respective baselines [Hassoun et al. 2015] when treated with upfront therapy, ambrisentan and tadalafil. Another recent pilot study looked at the 3 year outcomes of 19 patients with NYHA class III or IV PAH who received bosentan, sildenafil, and epoprostenol upfront. There were no controls in the retrospective study, which allowed for the possibility of selection bias, and one patient was excluded from analysis due to urgent lung transplantation. Notably, though, all patients were alive at the 3 year mark (where mortality was predicted to be roughly 50%). Furthermore, all 18 patients who remained improved to NYHA Class I or II symptoms [Sitbon et al. 2013]. This has spurred a larger phase III randomized control trial to validate these preliminary findings, which assign treatment-naïve patients to a combination of either macitentan, tadalafil, and selexipag or macitentan, tadalafil and placebo [TRITON trial, 2016].
A meta-analysis included 17 studies (out of just over 2000 reviewed) and nearly 4000 patients with both upfront and sequential therapy again showed strong evidence for combination therapy. However, the authors did not design their review to differentiate between upfront versus sequential therapy [Lajoie et al. 2016]. The overall risk reduction of clinical worsening was 35% on combination therapy, though it should be noted that these trials varied slightly in their definitions of TtCW.
Conclusion
PAH treatment has evolved rapidly over the past decade. It has been clearly demonstrated that upfront combination therapy is well tolerated and superior to upfront monotherapy in terms of meaningful clinical endpoints, mainly TtCW. While the initiation of PAH specific therapy is no longer in doubt, questions remain about the optimal combination regimen for specific subgroups of PAH. Novel therapeutic targets are in the nascent stages of development but may soon provide another avenue of treatment.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Trow has served on Advisory Boards for Bayer (Whippany, NJ, USA), Actelion Pharmaceuticals (South San Francisco, CA, USA), United Therapeutics (Silver Springs, MD, USA), and Lung Biotechnology (Silver Springs, MD, USA) in the past 24 months. He is also a sub-Principle Investigator on the BEAT trial sponsored by Lung Biotechnology and the OPUS Registry sponsored by Actelion Pharmaceuticals.
Dr Griffin has no potential conflicts of interest with respect to research, authorship, or publication of this article.