
Abstract
Background:
Bronchial occlusion with an Endobronchial Watanabe Spigot (EWS) has been shown to be useful in managing prolonged bronchopleural fistulas and intractable hemoptysis. EWS bronchial occlusion using a curette is less technically demanding. This retrospective study evaluated the clinical utility and simplicity of this method.
Methods:
A total of 18 consecutive patients (15 men, 3 women, aged 47–85 years) who underwent bronchial occlusion using an EWS from April 2012 to August 2014 were evaluated. The method involves sticking the tip of a curette into an EWS to the first joint, allowing it to be turned in any direction or at any angle. The time required to occlude the target bronchus was measured on routinely recorded digital videos. Other parameters evaluated included success rates, complications, and clinical outcomes.
Results:
Of the 18 patients, 11 underwent bronchial occlusion for intractable pneumothorax, 5 for postoperative bronchopleural fistula, two for intractable empyema, and one for hemoptysis. Each patient required 1–7 EWSs (median 4). Target bronchi included the right upper (n = 8), left upper (n = 5), right lower (n = 2), left lower (n = 2), and right middle (n = 1) bronchi. The success rate of EWS insertion into the target bronchus was 100%. Time per EWS occlusion ranged from 65–528 sec (median 158.5 sec). Of the 62 insertions, 36 (58.1%) were completed within 3 min, and 58 (93.5%) within 5 min. Successful outcomes were observed in 15 (83.3%) of the 18 patients.
Conclusions:
EWS bronchial occlusion using a curette is a simple method for managing intractable bronchopleural fistulas in daily clinical settings.
Introduction
Many endobronchial intervention techniques have been introduced recently into daily clinical practice. For example, bronchial stenting using silicone or metallic stents, and endobronchial therapies using neodymium yttrium aluminum garnet (Nd: YAG) lasers, argon plasma coagulation or microwave coagulation have been well established [Niwa et al. 2009; Dalar et al. 2016; Miller et al. 2013]. An Endobronchial Watanabe Spigot (EWS) is a silicone bronchial blocker developed by Watanabe and colleagues [Watanabe et al. 2003]. Bronchial occlusion with an EWS has been reported to be highly effective for the management of intractable pneumothorax and thoracic empyema with persistent bronchopleural fistula [Sasada et al. 2011; Ishida et al. 2015; Dalar et al. 2013]. As this procedure is relatively less invasive, it is suitable for patients who are elderly or unfit for surgical procedures. No special device is required for inserting an EWS into a target bronchus. In most cases, bronchoscopists use grasping forceps to hold a spigot tightly and insert it into the target bronchus. However, there may be difficulties inserting the bronchoscope into an arbitrary bronchus while holding an EWS. Moreover, operators should master a special technique such as ‘heel-kick method’ to plug the spigot into any target bronchus [Kida et al. 2016]. This report describes the advantages of a simple method that uses a curette to insert an EWS into a target bronchus. Using this method, we were able to insert an EWS into any bronchus of 18 consecutive patients (22 procedures) within a very short time.
Materials and methods
Patients
The medical records of consecutive patients who underwent bronchial occlusion with an EWS at Fujita Health University Hospital from April 2012 to August 2014 were retrospectively reviewed. All bronchoscopic procedures were recorded on a digital video recorder. The institutional review committee (Fujita Health University Institutional Review Board) approved this study protocol, which was conducted in accordance with the tenets of the Declaration of Helsinki (approval number Fujita-14-230).
Endobronchial Watanabe Spigot
EWSs, the silicone endobronchial plugs originally developed by Watanabe and colleagues, can be purchased from Novatech SA, France. They are made of medical-grade silicone dyed with barium sulfate for radiodiagnostic visibility, with studs on the outside to prevent migration. EWSs are available in three different sizes according to the diameter of the plug (small, 5 mm; medium, 6 mm; large, 7 mm) [Sasada et al. 2011]. EWS size was based on the diameter of the target bronchus measured on thin slice computerized tomography (TSCT), adjusted by direct bronchoscopic findings during the procedure.
Bronchoscopic procedures and EWS insertion
After administration of local pharyngeal anesthesia, all patients were lightly sedated with individually calculated doses of intravenous midazolam [Ogawa et al. 2014]. Before the bronchoscopic procedures, all patients were intubated and underwent chest TSCT (0.5 mm slices) using a nonenhanced multidetector CT system (Aquilion One Vision Edition; Toshiba Medical Systems, Tokyo, Japan). TSCT images were analyzed to detect the bronchus responsible for persistent bronchopleural fistula or hemoptysis. The responsible bronchi in patients with pneumothorax were detected by bronchial occlusion test using a balloon catheter (Disposable balloon catheter C, Olympus Medical Systems Co. Ltd., Tokyo, Japan). Responsible bronchi were defined as those showing a reduction or cessation of air leakage through the chest drainage tube following obstruction. Bronchoscopes with a 2.0 mm diameter working channel (BF-260 and BF-P260F; Olympus Medical Systems) and Cytology Curettes (Olympus Medical Systems) were used for insertion of an EWS into targeted bronchi (Figure 1). Briefly, a small cut was made at the thick end of the EWS to insert the tip of the curette. As EWS spigots are elastic, it was easy to make a cut using a tip of an 18-gauge injection needle (Figure 1A).

Photographs showing the method of EWS insertion using a cytology curette.
As the Cytology Curette has a tapered tip, it could be inserted into a cut made on the tip of the EWS. Equipped with an EWS, a curette could be rotated and bent at any angle and in any direction (Figure 1B). Following curette insertion through the biopsy channel of a bronchoscope, a spigot was attached to the tip of the curette, and the bronchoscope equipped with an EWS was inserted via an intubated tube into the target bronchus (Figure 1C, 1D). After reaching the target bronchus, the EWS was inserted into the bronchus by adjusting the angle and direction of the spigot. Once the EWS blocked the target bronchus, the curette was withdrawn while pressing the EWS with the bronchoscope into the target bronchus (Figure 1E).
Data acquisition
The time required for insertion of one EWS into the target bronchus during each procedure was retrospectively evaluated. All bronchoscopic procedures had been recorded by a digital video recorder. The time from insertion of the bronchoscope into the endobronchial tube to the successful insertion of an EWS into the target bronchus was measured on each video recording. Patient outcomes were determined by reviewing their medical records.
Results
During the study period, 18 consecutive patients (15 men and 3 women), of median age 69 years (range, 47–85 years) underwent bronchial occlusion using an EWS. Patient background and target disease for EWS insertion are shown in Table 1. The most frequent target disease responsible for bronchial occlusion was intractable pneumothorax due to persistent air leakage, followed by persistent postoperative bronchopleural fistula.
Demographic and clinical characteristics of the included patients.
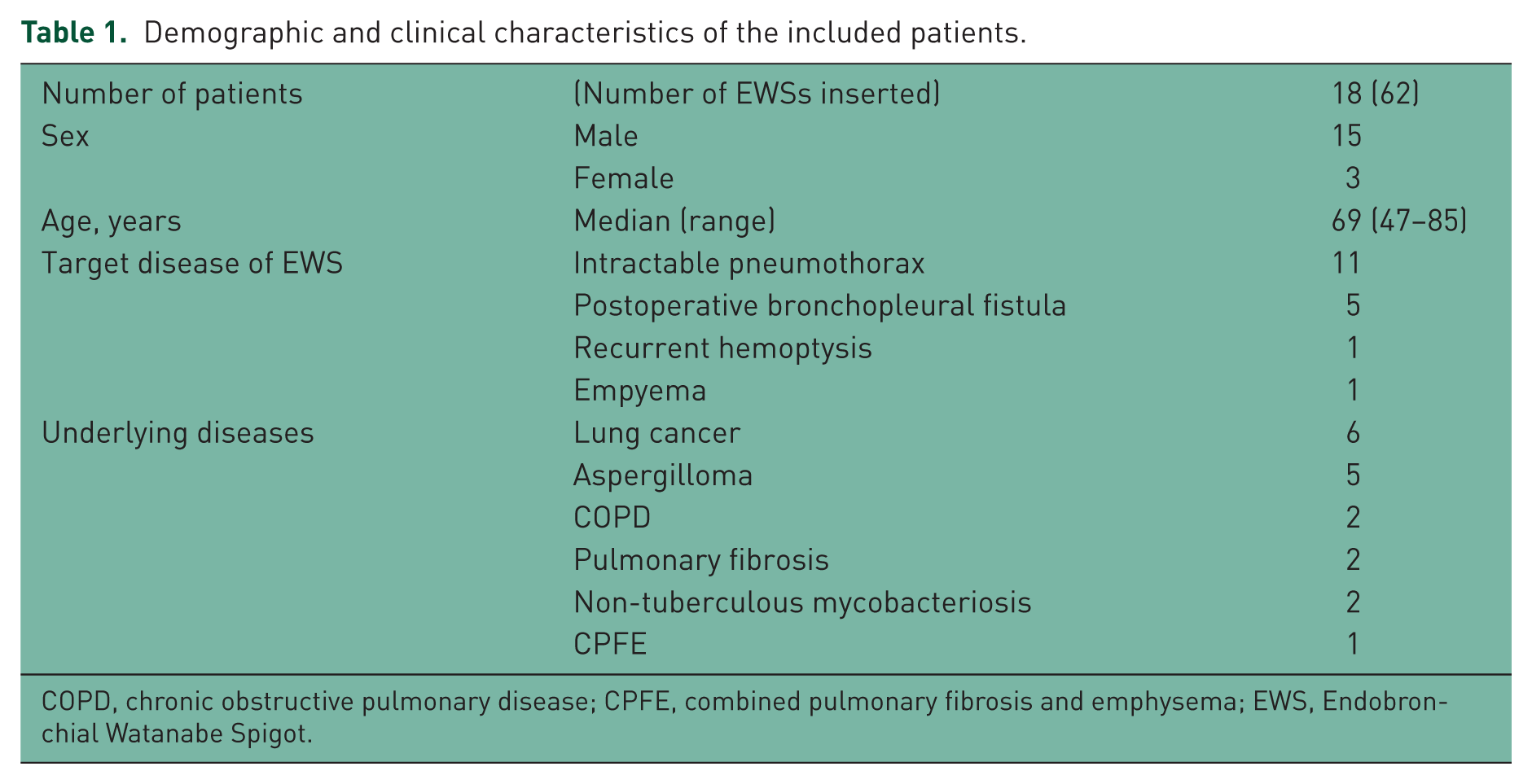
COPD, chronic obstructive pulmonary disease; CPFE, combined pulmonary fibrosis and emphysema; EWS, Endobronchial Watanabe Spigot.
An EWS was inserted into bronchi located in the right upper (n = 8), left upper (n = 5), right lower (n = 2), left lower (n = 2), and right middle (n = 1) lobes. Although 72% of the target bronchi were located in upper lobes, an EWS was successfully inserted into all target bronchi (success rate, 100%). The median time required for insertion of an EWS into the target bronchus was 158.5 sec (range, 65–528 sec). The median number of EWSs inserted per patient was 4 (range, 1–7), and the mean procedure time per EWS insertion ranged from 92–365 sec (Table 2). Of the total of 62 procedures, 36 (58.1%) were completed within 3 min and 58 (93.5%) within 5 min (Figure 2). An EWS was dropped from a curette into the trachea or main bronchi during 9 of the 62 procedures. Dropped EWSs were easily retrieved by bronchoscopic suction or by grasping using biopsy forceps. These data clearly showed that EWS insertion using a curette is a simple and useful method. In addition, it is noteworthy that we mainly used thin bronchoscopes (BF type 260 or BF p260F, Olympus Co. Ltd. Tokyo, Japan). This method did not require any devices other than a curette, such as grasping forceps. Thin bronchoscopes were more convenient as they could be inserted into the target bronchus more easily.
Target bronchi and mean procedure time per patient.
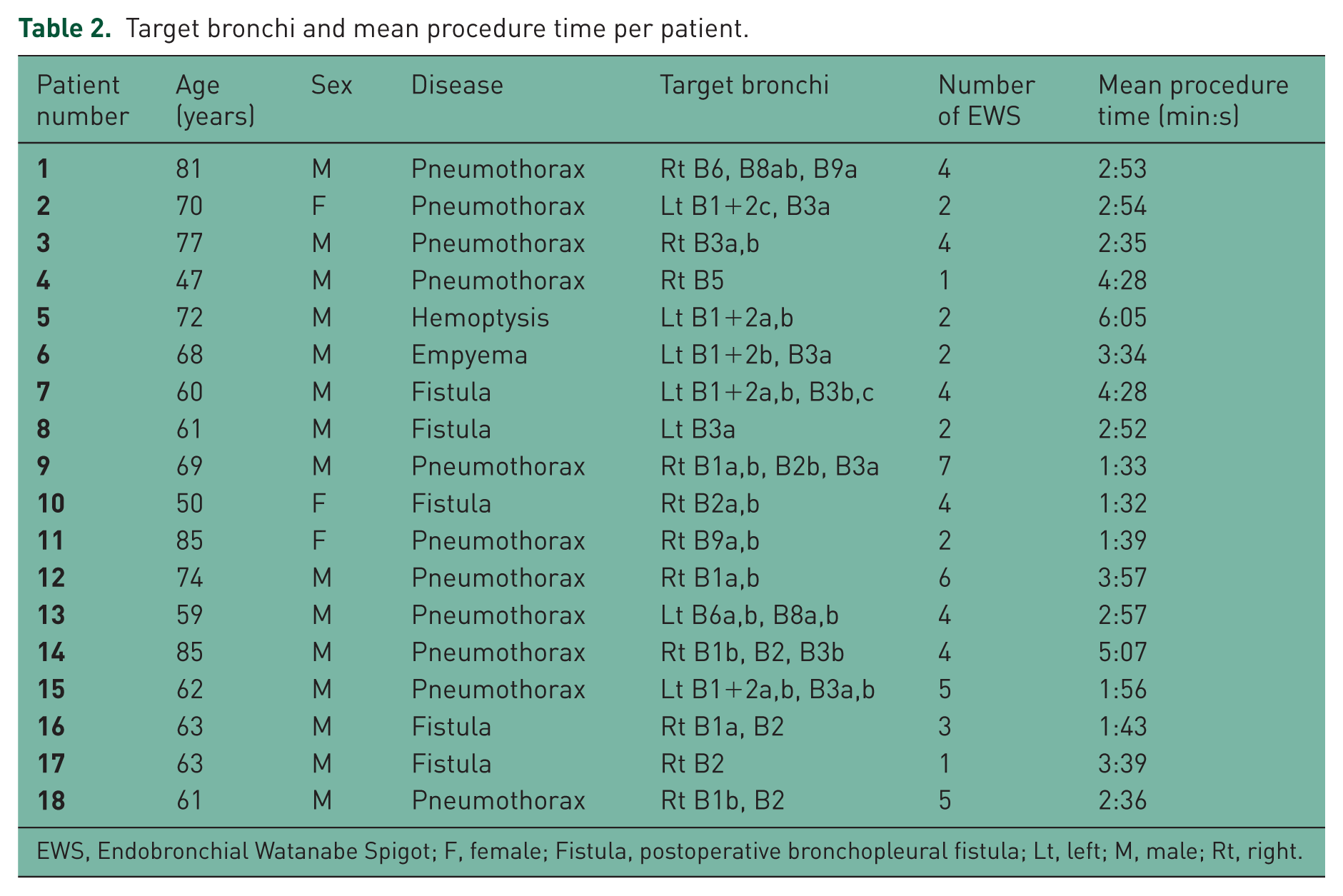
EWS, Endobronchial Watanabe Spigot; F, female; Fistula, postoperative bronchopleural fistula; Lt, left; M, male; Rt, right.

Time from the insertion of the bronchoscope into the endobronchial tube until successful insertion of an EWS into the target bronchus during each procedure. Of the 62 procedures, 36 (58.1%) were completed within 3 min, and 58 (93.5%) within 5 min.
Bronchial occlusion with an EWS yielded successful outcomes in 15 (83.3%) of the 18 patients (Table 3). Pleural drainage tubes could be successfully removed from 8 (72.7%) of the 11 patients with intractable pneumothorax due to reduction of air leakage followed by pleurodesis. Overall, two patients with postoperative bronchopleural fistula required a repeat EWS insertion to stop air leakage. Complications included obstructive pneumonia (n = 1), myocardial infarction (n = 1) and paroxysmal supraventricular tachycardia (n = 1). Overall, one patient with empyema died of sepsis. In this patient, EWS insertion failed to stop continuing air leakage via bronchopleural fistulas. A total of two patients with intractable pneumothorax died of underlying diseases (lung cancer and acute exacerbation of pulmonary fibrosis) before air leakage was stopped.
Outcomes of each procedure.

Recurrences in patients 7 and 8.
AE, acute exacerbation; COPD, chronic obstructive pulmonary disease; CPFE, combined pulmonary fibrosis and emphysema; EWS, Endobronchial Watanabe Spigot; fistula, postoperative bronchopleural fistula; NTM, nontuberculous mycobacteriosis; PSVT, paroxysmal supraventricular tachycardia.
Discussion
Persistent bronchopleural fistula is a problem occurring frequently in daily clinical settings. It may cause intractable pneumothorax or refractory pleural infection. Techniques described for the sealing of leaks have included those using tissue or fibrin glues, endobronchial devices of various kinds, and combination approaches [Slade, 2014]. Bronchial occlusion with an EWS is an established and useful method of treating intractable secondary pneumothorax. In some patients, especially those with severe emphysema or end-stage pulmonary fibrosis, a single bronchial occlusion would not be sufficient, and repeated bronchial occlusions may be required [Ishida et al. 2015]. As these patients may experience severe respiratory failure, the bronchial occlusion procedure with EWS should be completed in a short time. In addition, EWS insertion was recently shown to be useful for the management of massive hemoptysis, one of the most common emergency situations [Dutau et al. 2006; Adachi et al. 2016]. Thus, EWS insertion should be both easy and reliable, without requiring special skills. The conventional method, in which the EWS is grasped with larger sized grasping forceps, is the most popular method currently utilized [Kida et al. 2016]. However, because of difficulties turning the forceps in any direction, the conventional method may require expert bronchoscopists.
The method described in this report is a very simple technique, allowing an EWS to be inserted into bronchi within a few minutes. Although many young bronchoscopists in our institute perform this procedure, the total procedure time required for inserting one EWS ranged from 1–9 min (mean, 3 min). More than half of our young bronchoscopists had less than 3 years of bronchoscopic experience. Compared with other novel techniques for inserting an EWS, including the side-grasping and guide-wire assisted methods, [Kida et al. 2016; Coiffard et al. 2014] our method was characterized by the use of a curette. As a curette equipped with an EWS can be easily rotated in any direction, an EWS could be inserted into any bronchus in a shorter period of time. Moreover, because an EWS pierced by a curette to the first joint was strictly fixed, EWS dropout during the procedure seldom occurred. As a curette can be inserted through a working channel 2.0 mm in diameter, a thin bronchoscope 4.0 mm in outer diameter was frequently used, allowing an approach to further bronchi, such as subsegmental bronchi, directly. This may have led to good results, even when performed by less experienced bronchoscopists.
Several patients experienced complications during the study. Overall, one patient experienced a myocardial infarction just after the procedure, and a second developed paroxysmal supraventricular tachycardia during the procedure. Although both patients had no obvious cardiovascular medical history, their general condition had deteriorated due to chronic lung inflammation caused by aspergillosis. These cardiovascular complications may have been associated with diagnostic bronchoscopy [Asano et al. 2012]. Cardiovascular complications are not likely caused by EWS insertion but by bronchoscopy on patients in poor general condition. Overall, one patient experienced obstructive pneumonia following successful bronchopleural fistula obstruction of refractory pneumothorax resulting from drainage tube removal. The pneumonia resolved immediately after the removal of the EWS with administration of antibiotics. Although plugged EWSs were not removed from other patients, no other patient has experienced obstructive pneumonia. Although long-term placement of EWS would be safe in most cases [Kaneda et al. 2015], EWS insertion may induce obstructive infection.
This study was an observational study involv-ing a limited number of patients at a single institution. The method described here could not be directly compared with other, previously reported methods. Despite these limitations, our method for bronchial occlusion with an EWS using a curette is simple and reliable, even when performed by less-experienced bronchoscopists. Prospective, multicenter clinical trials comparing this method with other methods are warranted.
Footnotes
Acknowledgements
The authors thank Mrs Naomi Maeda for her excellent secretarial help. They also thank Mrs Chikako Hibiya and Ms Noriko Hiramatsu for their generous technical assistance.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by JSPS KAKENHI (grant number 15K09198).
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.