
Abstract
Chronic respiratory diseases, such as asthma and chronic obstructive pulmonary disease (COPD), represent a major social and economic burden for worldwide health systems. During recent years, increasing attention has been directed to the role of small airways in respiratory diseases, and their exact contribution to the pathophysiology of asthma and COPD continues to be clarified. Indeed, it has been suggested that small airways play a distinct role in specific disease phenotypes. Besides providing information on small airways structure and diagnostic procedures, this review therefore aims to present updated and evidence-based findings on the role of small airways in the pathophysiology of asthma and COPD. Most of the available information derives from either pathological studies or review articles and there are few data on the natural history of small airways disease in the onset or progression of asthma and COPD. Comparisons between studies on the role of small airways are hard to draw because both asthma and COPD are highly heterogeneous conditions. Most studies have been performed in small population samples, and different techniques to characterize aspects of small airways function have been employed in order to assess inflammation and remodelling. Most methods of assessing small airways dysfunction have been largely confined to research purposes, but some data are encouraging, supporting the utilization of certain techniques into daily clinical practice, particularly for early-stage diseases, when subjects are often asymptomatic and routine pulmonary function tests may be within normal ranges. In this context further clinical trials and real-life feedback on large populations are desirable.
Introduction
Chronic respiratory diseases represent one of the major global issues for national healthcare systems [Gibson et al. 2013]. The condition of chronic obstructive pulmonary disease (COPD) has been ranked as the fourth leading cause of death in the world [Lozano et al. 2012] and together with asthma, affects an individual patient’s quality of life, with over 100,000 disability-affected life years (DALYs) in 2010 [Vos et al. 2012]. These staggering figures translate into significant healthcare costs and a considerable economic-social burden [Mannino et al. 2015].
During recent years, increasing attention has been directed to the importance of the contribution of small airways in respiratory diseases. The pathophysiological involvement of small airways in both COPD and asthma has been extensively documented [Usmani, 2012, 2014; Stewart and Criner, 2013] and there are ongoing efforts to define their exact contribution to these disorders. Indeed, whether small airways play a distinct role in specific disease phenotypes (i.e. severe or nocturnal asthma, exercise-induced bronchoconstriction, emphysema) and are involved in certain patient clusters (i.e. frequent exacerbators, smokers) has been suggested, but further comprehensive studies are needed to confirm this.
The aim of this review is to provide updated evidence on the role of small airways in the pathophysiology of asthma and COPD and of their specific phenotypes, undertaking a search strategy up to December 2014 in the principal electronic databases of MEDLINE, EMBASE and CENTRAL. The keywords ‘asthma’, ‘COPD’, ‘chronic obstructive pulmonary diseases’ and ‘small airways’ were used in the search strategy.
Small airways structure
The lungs are a branching structure, segmentally dividing from the trachea (generation 1) down to the alveoli (generation 23) [Weibel, 1963]. The lower airways can be divided into a conducting airway zone (generations 1–16) that transports the inhaled air and a respiratory acinar zone (generations 17–23) involved in gas exchange [Hyde et al. 2009].
Comprehensive studies into the small airways were undertaken by Malcolm Green [Green, 1967], whose calculations were applied to the anatomical findings of Ewald Weibel [Weibel, 1963]. The small airways were subsequently defined as those airways with an internal diameter less than 2 mm. They are generally located from the eighth generation of airways to the respiratory bronchioles and account for 98.8% (approximately 4500 ml) of the total lung volume [Virchow, 2009]. Because small airways contain little or no cartilage, they are easily collapsible (i.e. during forced expiration or smooth muscle contraction). Furthermore, with a higher generation number, the airway diameter gradually decreases, suggesting that obstruction may occur more easily. In contrast, the cross-sectional area of the airways increases rapidly from a total of 2.5 cm2 in the trachea to approximately 180 cm2 in the terminal bronchioles. Resistance to airflow in the airways varies inversely with the fourth power of the entire cross-sectional area. These numbers explain why most of the resistance to airflow in healthy subjects is located in the proximal airways and why small airways account for less than 10% of airway resistance [Martin et al. 2013]. For this reason, small airways have been historically called ‘the quiet zone’, because of their large reserve capacity and the concept that extensive disease could be present with mild abnormalities in conventional pulmonary function tests and no change in symptoms [Usmani and Barnes, 2012]. However, in patients affected by chronic airway diseases, it has been reported that peripheral airways are the predominant site of airflow resistance, irrespective of the different pathophysiological mechanisms involved [Yanai et al. 1992].
Small airways assessments
It can be appreciated that the measurement of small airways dysfunction represents a big challenge, and progress in this area has been hampered by technical limitations related to the small size of these airways and to their deep location in the thoracic cavity [Siddiqui and Usmani, 2012; Sterk and Bel, 2011]. Over the years, several procedures have been suggested and adopted to study this region of the lung, including complex and sometimes invasive techniques. Such procedures can either provide functional information on the degree and extent of ventilation heterogeneity and air trapping, or facilitate the understanding of inflammatory and remodelling processes (Table 1) [Contoli et al. 2010]. Nevertheless, a unanimously agreed approach to investigate small airways, and more generally the distal lung, is still lacking.
Features of the principal techniques for assessing small airways (adapted from Contoli et al. [2010]; Usmani [2014]).
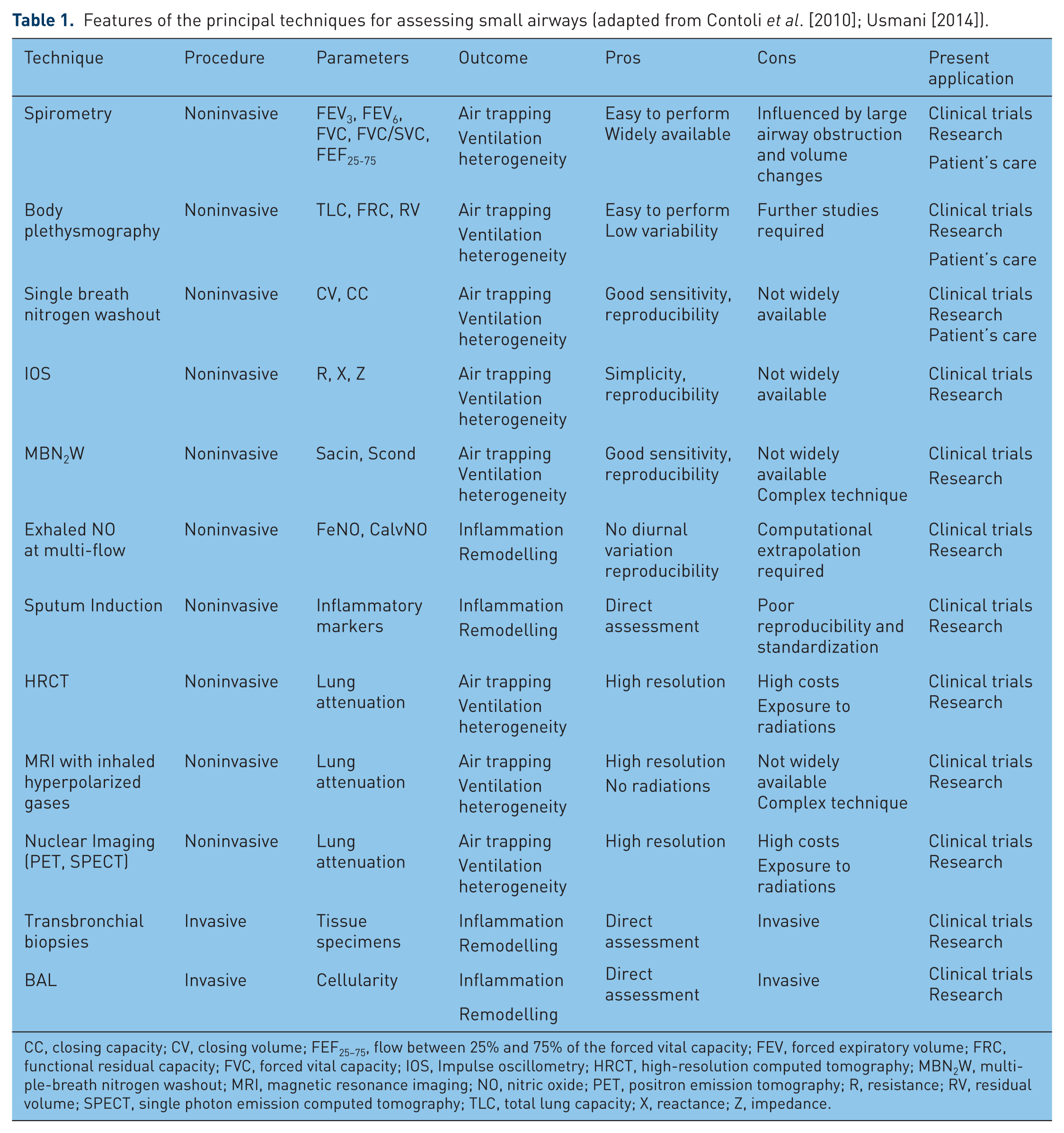
CC, closing capacity; CV, closing volume; FEF25–75, flow between 25% and 75% of the forced vital capacity; FEV, forced expiratory volume; FRC, functional residual capacity; FVC, forced vital capacity; IOS, Impulse oscillometry; HRCT, high-resolution computed tomography; MBN2W, multiple-breath nitrogen washout; MRI, magnetic resonance imaging; NO, nitric oxide; PET, positron emission tomography; R, resistance; RV, residual volume; SPECT, single photon emission computed tomography; TLC, total lung capacity; X, reactance; Z, impedance.
Spirometry is the gold standard for the diagnosis and management of chronic obstructive respiratory diseases. However, it is widely recognized that forced expiratory volume in 1 s (FEV1) does not properly reflect small airways abnormalities [Cosio et al. 1978]. Other lung function indices have been proposed and evaluated as markers of small airways function. Among these, the forced expiratory flow between 25% and 75% of the forced vital capacity is the most commonly adopted, although the literature on its reliability is not conclusive [Sutherland et al. 2004; Sorkness et al. 2008], and the American Thoracic Society does not support its use for determining small airways disease [Becklake et al. 1991]. Measurement of lung volumes by body plethysmography, such as total lung capacity, functional residual capacity, and residual volume may provide more reliable information [Kraft et al. 2001], but are only available in specialized pulmonary function units in respiratory centres.
Recently, interest has focused on reutilizing historically established physiological techniques. The single-breath nitrogen (N2) washout test allows one to distinguish between ventilation heterogeneity originating in the peripheral airways versus that in the more proximal conducting airways. Gas distribution in the lungs is analysed by measuring the change in N2 concentration during the expiration phase of a vital capacity manoeuvre, following a single breath of 100% oxygen. Measurements that can be undertaken include closing capacity (CC), closing volume (CV), the nitrogen slope of phase III and lung volumes and it has been shown that an increased CV or CC reflects air trapping due to small airways narrowing or closure [Al-Bazzaz, 1979].
The multiple-breath nitrogen washout (MBN2W) test involves inhalation of 100% oxygen to wash out resident airway nitrogen gas during tidal breathing and it is highly reproducible [Downie et al. 2007; Verbanck et al. 2012]. The rate and extent of nitrogen exhalation from the tracheobronchial tree allows an assessment of ventilation heterogeneity in the lungs, distinguishing between the contribution from the proximal conducting airways compartments and that from the distal acinar regions in both asthma and COPD [Crawford et al. 1985; Robinson et al. 2013]. Furthermore, MBN2W has also been shown to predict small airways changes in smokers even before conventional spirometry becomes abnormal [Verbanck et al. 2006].
Impulse oscillometry (IOS) has been utilized to measure small airways function in both asthma and COPD. IOS generates oscillating pressure-flow signals of air during tidal breathing to determine central and peripheral lung mechanical parameters, such as resistance (R), reactance (X) and impedance (Z) [Goldman et al. 2005]. An increasing number of studies suggest that IOS measurements could be useful in the diagnosis of obstructive lung disease [Kolsum et al. 2009]. Both IOS and MBN2W may be used not only to assess functional abnormalities in the small airways, but also to longitudinally monitor the effects of interventions and pharmacological treatments [Borrill et al. 2008; Verbanck et al. 1999]. Further studies are being undertaken to determine whether they can be adopted in daily clinical practice [Latzin and Thompson, 2014].
Several novel exhaled biomarkers have recently been evaluated for studying distal lung inflammation and oxidative stress, including exhaled nitric oxide (NO), endothelin 1, eotaxin 1, regulated on activation, normal T cell expressed and secreted(RANTES) and hydrogen peroxide [Burgel, 2011]. NO is the most widely used biomarker in exhaled breath. It has been demonstrated that NO is increased in subjects with intrapulmonary inflammation [Barnes et al. 2010]. Measurements of exhaled NO are typically obtained using a single exhalation flow rate during tidal volume, but in view of its characteristic flow rate dependency, the use of several different flow rates allows one to assess where the inflammation is more active by separating NO produced from central airways (low flows) from that generated in the alveolar region (high flows) [Tsoukias and George, 1998]. Alveolar NO has been widely investigated as a potential marker of distal lung inflammation. Recent studies suggest that alveolar NO measurement does not require sophisticated equipment or mathematical models, and is reproducible and applicable in both asthma and COPD [Paredi et al. 2014; Brindicci et al. 2005, 2007]. However, since alveolar NO measurement is derived from a computational extrapolation that follows exhaled NO assessment at different flow rates, rather than being directly quantified, its clinical significance is still not completely established. Certainly, the role of back diffusion of NO into small airways and alveoli has been highlighted as a potential bias for the meaningful interpretation of altered alveolar NO [Van Muylem et al. 2010], although recent data suggest this may not be as critical in the clinical scenario as initially predicted by mathematical models [Scichilone et al. 2013]. The technique of assessing the number concentration of particles in exhaled breath (that are thought to originate from the respiratory tract lining fluid) using laser light scattering particle spectrometry has been utilized to assess the airways [Fairchild and Stampfer, 1987; Wan et al. 2014], and this noninvasive technique may be valuable to differentiate proximal and distal airway effects [Holmgren et al. 2014].
Sputum induction following inhalation of hypertonic saline is a noninvasive technique that has proven to be valid for studying inflammatory cells in central airways [Magnussen and Holz, 1999]. Modified protocols have been proposed to evaluate whether this method can also assess inflammation in small airways. In particular, it has been suggested that sequential inductions, performed after short intervals of time (20–30 min), may provide useful information on distal airway inflammation [Gershman et al. 1999; Richter et al. 1999; Tsoumakidou et al. 2003]. However, this procedure may be associated with issues regarding reproducibility and standardization, and no studies have been performed to directly compare the inflammatory profile in sputum with small airways assessment through transbronchial biopsies.
The use of blood biomarkers has also been suggested for the study of small airways involvement. In particular, 16 kDa Clara cells (CC-16) proteins, which are mainly produced in the terminal bronchioles and play an immunoregulatory and anti-inflammatory role in innate immunity, may be predictive of lung epithelial damage and serve as a sensitive indicator of nonciliated bronchial cell dysfunction [Bernard et al. 1992].
Lung imaging is an increasing area of interest that has been utilized for the assessment of small airways involvement in asthma and COPD and that deserves consideration. High-resolution computed tomography (HRCT) is a noninvasive method that may provide anatomical details of the bronchial tree. However, HRCT can only estimate wall thickness of bronchi that are 1–2 mm in diameter [Vos et al. 2013]. Although this only partially allows a direct assessment of small airways abnormalities, air trapping and ventilation heterogeneity have been quantified to indirectly support small airways functional parameters [Ueda et al. 2006]. Further studies also suggest that HRCT parameters of air trapping can be selectively modified by inhaled and systemic pharmacological treatments [Goldin et al. 1999]. However, despite the promising results obtained, this technique is still expensive, technically challenging and hampered by exposure of patients to radiation, although the use of the low-dose radiation procedures has been employed [Lutey et al. 2013].
In the last decade, investigators have focused efforts on magnetic resonance imaging (MRI) of the lung, following inhalation of hyperpolarized helium and xenon, in order to provide additional structural insight into small airways involvement in chronic obstructive respiratory diseases [Kauczor et al. 2001]. Indeed, these gas-enhanced techniques allow higher resolution and can detect and quantify ventilation and perfusion heterogeneity, without radiation exposure. Hyperpolarized helium has been used to assess regional airflow obstruction and ventilation abnormalities in asthma, COPD and emphysema, by providing information at the alveolar and small airways level [de Lange et al. 2006]. However, at present, this procedure is only available in a few centres, technically demanding and not established for clinical applications. Ventilation perfusion relationships in the peripheral airways have also been assessed with single photon emission computed tomography and positron emission tomography, although these procedures are limited due to the requirement of high doses of radiation [Musch and Venegas, 2005].
The pathophysiology of small airways and the degree of airway inflammation can be directly assessed using invasive techniques, such as bronchoalveolar lavage, endobronchial and transbronchial biopsies [Shaw et al. 2002; Balzar et al. 2002]. However, although in the past such procedures have been of great support for understanding the pathology of small airways in respiratory diseases, and more recently this approach has been used to assess the distribution and type of inflammatory cells in small airways, they are obviously not applicable in daily clinical practice.
Small airways involvement in asthma
Despite the increasing interest in small airways involvement in asthma, the number of original articles specifically addressing their role in disease pathophysiology is relatively limited. Most of the evidence derives from invasive historical pathological studies that collected lung tissues from autopsied patients or from subjects with asthma needing lung resection because of malignancy, as well as from data on patients undergoing transbronchial biopsies [Corren, 2008]. Small airways are thickened in asthma due to chronic inflammation in the epithelium, submucosa and muscle area [Carroll et al. 1993]. It has been suggested that the outer wall is more inflamed than the inner wall, with a higher numbers of lymphocytes, eosinophils, and neutrophils associated to an increased mRNA expression of interleukin (IL)-4, IL-5 and eotaxin [Hamid et al. 1997]. The latter may contribute to an uncoupling of the small airways with the surrounding lung parenchyma increasing their collapsibility. Some investigations suggest that the cellular infiltrate increases towards the periphery, while others show different patterns [Haley et al. 1998; Balzar et al. 2005]. These contradictory data may be ascribed to the heterogeneity of asthma and to the different methods adopted in the studies.
Researchers have also explored the features of the small airways in subjects with asthma using noninvasive techniques. Battaglia and coworkers showed, in a group of 16 patients with asthma, that the single breath nitrogen washout (nitrogen slope of phase III and closing volume) was significantly related to exhaled NO and pulmonary function test results, suggesting small airways involvement in the pathogenesis of the disease [Battaglia et al. 2005]. Abnormal acinar ventilation heterogeneity has also been reported to be present despite mild symptoms and normal spirometry, supporting the role of small airways as early marker of disease [Singer et al. 2014].
A more robust amount of data relates to the clinical course and the degree of control of asthma with small airways disease. Van Veen and colleagues found that exhaled NO predicts lung function decline in patients with severe asthma during 5 years of prospective follow up [van Veen et al. 2008]. Interestingly, this relationship was only observed in subjects with baseline FEV1 greater than 80% predicted, suggesting that these findings may be related to small rather than larger airways. Bourdin and coworkers reported that patients with asthma and a history of two or more exacerbations per year had a significant increase in the slope of phase III nitrogen washout [Bourdin et al. 2006]. However, since this study had a cross-sectional design, it is unclear whether this represents simply an association or whether abnormalities in small airways may be considered as a predictive marker of subsequent exacerbations. In a further trial, a group of patients with asthma and recurrent exacerbations (at least two exacerbations in the previous year) were compared with a group of subjects with equally severe but well controlled asthma. The authors reported that patients with asthma who had recurrent exacerbations had increased closing volume and closing capacity compared with controls, even after bronchodilation [in’t Veen et al. 2000]. Schichilone and colleagues have shown that the alveolar component of exhaled NO was associated with a lack of asthma control in 78 patients with mild, untreated asthma [Scichilone et al. 2013]. Similar results were reported in patients with acute severe asthma by Thompson and coworkers, who showed a direct correlation between functional abnormality in the acinar zone and airflow obstruction, degree of asthma control and treatment requirement [Thompson et al. 2013]. It has also been reported that peripheral airway function assessed by IOS significantly contributes not only to the level of asthma control, but also to patients’ quality of life and perception of symptoms [Takeda et al. 2010].
An important question is whether small airways involvement in asthma is variable among distinct asthma phenotypes or whether it occurs in all patients. Cluster analyses have been recently used to identify specific asthma phenotypes [Moore et al. 2010], but markers of small airways function have not been investigated. However, evidence is accumulating to support the concept that small airways dysfunction and inflammation may contribute to distinct asthma phenotypes. Kraft and colleagues reported that patients with nocturnal asthma had significantly greater numbers of eosinophils in the small airways compared with the proximal airways in biopsies undertaken during the night. In addition, eosinophil and macrophage counts were increased in biopsies of their distal airways undertaken at night compared with those taken in the afternoon [Kraft et al. 1996]. Furthermore in a follow-up study performed by the same group, it was reported that patients with nocturnal asthma showed significantly increased peripheral airways resistance compared with those with non-nocturnal asthma [Kraft et al. 2001]. Patients with severe asthma have more neutrophils in the lung parenchyma and display more extensive air trapping, as measured with quantitative CT scanning, indicating small airways disease [Wenzel et al. 1997]. More thickened small airways and higher numbers of eosinophils are detectable in subjects with fatal asthma, who also exhibit more goblet cells and neutrophils when affected by a disease of short duration, suggesting that the underlying inflammatory process is also present in the distal airways [Carroll et al. 1997]. Small airways involvement has been also implicated in the onset and severity of exercise-induced bronchoconstriction. Kaminsky and colleagues challenged patients with asthma with dry cool air and observed, using a wedged bronchoscope, that there was a significant postchallenge increase in peripheral airways resistance in patients with mild asthma compared with healthy subjects [Kaminsky et al. 1995]. It has also been found that hyperventilation increased urinary levels of CC16 proteins which, being produced by epithelial cells in the bronchiole, may act as a biomarker for peripheral airways [Kosmas et al. 2004]. Abnormalities within small airways, associated with some degree of air trapping, may lead to delayed emptying of the peripheral airways during exercise and this may contribute to the frequently observed phenomenon of dynamic hyperinflation [Kosmas et al. 2004].
Until recently, small airways function had not been used to differentiate between asthma and COPD. However, mathematical and statistical analyses of the dynamic fluctuations in IOS impedance have now revealed that patients with asthma and COPD behave differently, suggesting that this technique may be helpful to discriminate between the two diseases [Muskulus et al. 2010; Paredi et al. 2010]. Noninvasive measurement of volatile organic compounds using the electronic nose may also be helpful in discriminating these two morbid conditions [Fens et al. 2009]. On the contrary, no literature data are available on the role of small airways in the asthma–COPD overlap syndrome.
Small airways involvement in COPD
The role of small airways in COPD is based on an established history of scientific findings. Lynne Reid, a pathologist working at the Royal Brompton Hospital, was the first to quantitate airway remodelling in COPD. In 1960 she developed the Reid Index to describe the thickness of the airway wall occupied by hyperplastic mucus glands in smokers and patients with COPD [Reid, 1960]. Thurlbeck and Angus used this index to show that airway disease was also present in patients with emphysema, though these conditions could occur separately [Thurlbeck and Angus, 1964]. A research group in Oxford explored this observation further and showed that COPD without emphysema was quite common and that the disease involved the whole bronchial tree [Dunnill, 1969].
It was the landmark study of Hogg and colleagues that characterized the small airways abnormalities in COPD. In this study, peripheral airway resistance was increased because of mucus plugging, narrowing and obliteration of the small airways. [Hogg et al. 1968]. However, why some patients manifested airflow obstruction in the form of airway narrowing and others because of reduced elastic recoil remained unclear. More clarity on this observation was provided in 2004 when Hogg examined the small airways of 159 patients with COPD and related pathologic findings with their Global Initiative for Chronic Obstructive Lung Disease(GOLD) severity physiological staging, showing that the progression from stage 0 to 4 was associated with small airways wall thickening, as a repair response to the airway wall inflammatory injury [Hogg et al. 2004]. However, the degree of small airways luminal occlusion and the extent of the localized regional inflammatory response were weakly associated with disease severity. Subsequently, McDonough and colleagues analysed multidetector computed tomography images from 78 patients with COPD undergoing imaging as part of a lung cancer screening study, as well as by examining lung tissue on micro-CT and histologically. They showed that the number of small airways per lung pair was reduced in patients with GOLD stage I COPD compared with control subjects and that this was even further reduced in patients with GOLD stages 3 and 4 [McDonough et al. 2011].
More recently, Timmins and colleagues undertook to definitively determine the independent contributions of emphysema and small airways disease to airflow obstruction and COPD severity. Twenty-six subjects with COPD underwent measurements with impulse oscillometry, single-breath nitrogen washout and CT lung scanning, in addition to baseline pulmonary function tests. Results obtained showed that the degree of airway obstruction and the disease severity were significantly predicted by both the extent of emphysema and by small airways parameters, such as the expiratory flow limitation and closing volume/vital capacity ratio [Timmins et al. 2012]. Hogg and coworkers have also provided new insights based on micro-CT imaging and MRI imaging to support that both narrowing and reduction in numbers of terminal bronchioles contribute to the rapid decline in FEV1 which leads to severe airway obstruction in COPD. Moreover, the observation that terminal bronchiolar loss precedes the onset of emphysematous destruction suggests this process begins in the very early stages of COPD [Hogg et al. 2013] and might be an area that needs to be specifically targeted with pharmacological therapy early on in the disease, potentially by using small particle aerosols that reach deeper into the lungs [Usmani et al. 1003, 2005].
Moving from a mechanical to a cellular perspective, it is widely recognized that CD8+ T lymphocytes are the predominant inflammatory cells in both large and small airways of COPD lungs and that their number correlates with the degree of airflow obstruction. These CD8+ T lymphocytes induce apoptosis and necrosis of epithelial and endothelial cells, which likely contribute to the lung damage observed in COPD [Stewart and Criner, 2013]. Several studies demonstrated that the small airways inflammatory reaction results from exposure to cigarette smoking and occurs earlier than the development of tissue destruction and fibrosis, and also prior to clinically detectable airflow obstruction [Niewoehner et al. 1974; Saetta et al. 2011]. However, although inflammatory cell infiltration of the small airways is started by smoke exposure, it seems to be independent of the intensity of smoking and may be prolonged even after smoking ceases [Burgel, 2011; Cosio et al. 2009]. Distinguishing patterns of inflammatory responses in the small airways compared with large airways may be relevant to elucidate the pathogenesis of COPD. Battaglia and colleagues examined lung tissue in a group of smokers and found an increased neutrophil density in the lamina propria of small airways, while the CD4+ T-lymphocyte count was higher in the lamina propria of large airways; no statistically significant difference was detected in CD8+ T lymphocytes [Battaglia et al. 2007]. More recently, Isajevs and colleagues studied lung tissue from 19 nonsmokers, 20 smokers with normal lung function, and 20 smokers with moderate COPD undergoing lung resection [Isajevs et al. 2011]. The investigators showed that cigarette smoke induced an increase in proinflammatory cytokine levels, by activating the nuclear factor κB (NFκB) transcription factor and by inhibiting histone deacetylase 2(HDAC2), which is associated with increased inflammation in alveolar macrophages and leukocytes. The authors also reported that patients with COPD had more macrophages in proximal airways and more CD8+ T lymphocytes and neutrophils in distal airways. The NFκB p65 expression was greater in large airways, correlating with an increased number of macrophages, while the HDAC2 expression was mainly decreased in small airways, suggesting its potential role in the development of bronchiolitis. Such nonuniform distribution of inflammatory cells could be ascribed to anatomic or immune differences, although further studies need to be undertaken to clarify these differences.
It is difficult to determine the effect of small airways abnormalities on COPD progression and survival due to the limited number of studies and the complexities of assessing this lung area, as described above. Verbanck and colleagues studied the impact of small airways disease in a group of asymptomatic smokers of greater than 10 pack-year history, with spirometric airflow obstruction and who had successfully stopped smoking, in comparison to a control group of active smokers [Verbanck et al. 2006]. While lung function parameters were relatively unaffected by smoking cessation, ventilation heterogeneity of the distal airway compartments, assessed with the MBN2W technique, improved by 30% at 1 week and 42% at 1 year. In another study, Gennimata and colleagues reported a progressive increase in the slope of the phase III single breath nitrogen test, from smokers with normal lung function to patients with COPD at GOLD stage IV [Gennimata et al. 2010]. In a study using lung tissue from lung volume reduction surgery, Kim and colleagues studied 25 patients with severe COPD and related small airways pathologic findings to changes in FEV1 at 6 months after surgery [Kim et al. 2005]. Classifying patients as responders to the surgical treatment, if they had a change in FEV1 greater than 12% or greater than 200 ml, the authors showed that the small airways of nonresponders had increased epithelial height and area, more mucous metaplasia, and less bullous disease. These results were replicated a few years later, by the same group of authors, in 67 patients with advanced upper lobe predominant emphysema [Kim et al. 2010]. Hogg and colleagues assessed other pathological features, including the presence of luminal occlusion, wall thickening and lymphoid follicles in the small airways of 101 individuals who underwent lung volume reduction surgery for advanced COPD [Hogg et al. 2007]. Subjects with the greatest luminal occlusion were shown to die significantly earlier. This association persisted even after adjustment for covariates (surgical procedure, age, symptoms, FEV1). However, as this study only involved severe patients, it is hard to generalize whether all patients with COPD with significant small airways involvement have reduced survival.
Conclusions and perspectives
Small airways represent a topic of scientifically and clinically relevant interest. Their structure and involvement in chronic obstructive respiratory diseases have been extensively assessed. However, most of the available information derived, particularly for COPD, is either from nonexperimental papers (reviews) or from invasive historical pathological studies. The precise physiological role of small airways in the onset and progression of asthma and COPD needs further clarification, and definitive conclusions have often been hard to draw because both asthma and COPD are highly heterogeneous diseases with different phenotypes. The development of newer, modern, accurate and noninvasive techniques that have been validated may now facilitate the study of a lung region which in the past had been hardly accessible. The application of these innovative procedures, at present mainly confined to research investigations, may realistically be extended to the daily clinical practice with more user-friendly equipment and portable machines. It is tantalizing to postulate that the comprehensive assessment of the small airways in the diagnostic flow chart of asthma and COPD could be of extreme help, particularly in the assessment of the initial stages of the disease, when subjects are often asymptomatic and commonly adopted pulmonary function tests may be within normal ranges. Data reinforcing this notion relate to observations that small airways indices have been reported to be altered not only in very mild clinical disease states, but even in healthy smoker subjects [Gennimata et al. 2010; Niewoehner et al. 1974], representing potential valuable early markers of risk and disease.
Furthermore, small airways indices may provide useful information to better understand the heterogeneity of chronic obstructive lung diseases and to additionally characterize different clinical phenotypes. With the latter, particular value could be assigned to the evaluation of small airways in the study of the asthma–COPD overlap syndrome [Gibson and Simpson, 2009], which despite being encountered more often in clinical practice still has indeterminate pathophysiological literature. Indeed, recent findings support the usefulness of small airways assessment in the choice of treatment strategies and in monitoring patients’ response to therapies that are directed to the deeper lungs and may be beneficial in contrast to conventional treatments targeted predominantly to the proximal airway tree [Usmani, 2015; Corradi et al. 2014; Usmani et al. 2005]. In conclusion, both clinical trials and real-life study interventions on large populations would be desirable for accurately assessing the pathophysiological role of small airways in asthma or COPD and determining the value of small airways markers in phenotyping and managing patients with chronic respiratory diseases.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/ or publication of this article: Dr Omar S. Usmani is a recipient of an NIHR (National Institute of Health Research, UK) Career Development Fellowship. The study was supported by the NIHR Respiratory Disease Biomedical Research Unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College London. The authors do not report any sources of financial and material support directly related to the preparation of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.