
Abstract
Objective:
Glycopyrronium bromide has a quaternary ammonium structure and a low oral bioavailability, which reduces its systemic effects; it acts through a bronchodilating blockade of muscarinic receptors. The aim of this retrospective study was to analyze a possible relationship between the changes in the small airways and the efficacy of a bronchodilation with glycopyrronium bromide; exercise tolerance was also assessed, by performing the six-minute walking test.
Methods:
Forty-one patients were identified (23 females/18 males; mean age 66.82 ± 9.75 years), with a normal forced expiratory volume in 1 s (FEV1)/forced vital capacity ratio of 77.45% ± 4.86%, a reduced forced mid-expiratory flow between 25% and 75% of forced vital capacity (FEF25–75) of 42.9% ± 10.5%, with an increased residual volume/total lung capacity ratio of 132.68% ± 6.41%, FEV1 1.85 ± 0.54 L, forced vital capacity 2.39 ± 0.71 L, airway resistance (sR tot) 168.18% ± 42.5%, total lung capacity 98.28% ± 8.9%, six-minute walking test distance 318.3 ± 36.6 m, modified British Medical Research Council dyspnea scale 1.48 ± 0.77. All patients were initiated with glycopyrronium bromide 50 μg/die and reassessed after 4 months.
Results:
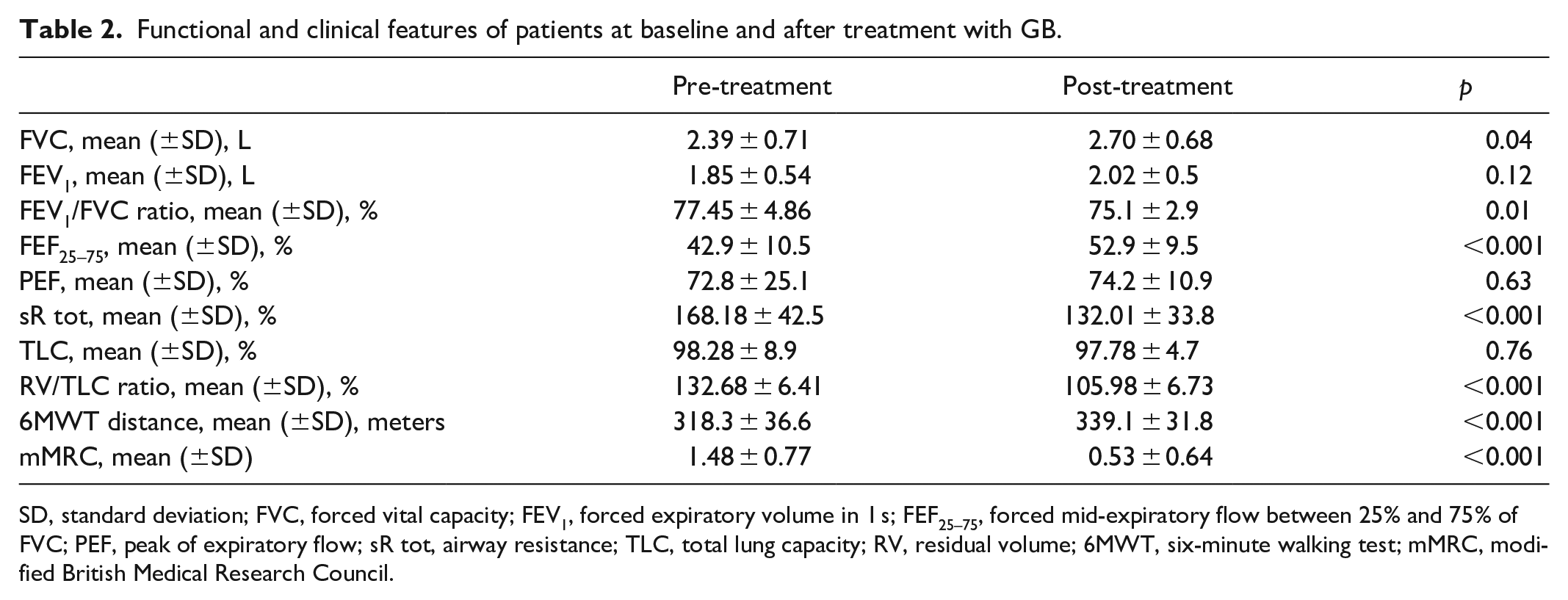
After the treatment with glycopyrronium bromide, a significant improvement was noted regarding forced vital capacity (p = 0.04), FEF25–75 (p < 0.001), sR tot (p < 0.001), residual volume/total lung capacity ratio (p < 0.001) with reduction of dynamic hyperinflation, the significant increase of the distance covered during the six-minute walking test (p < 0.001), and modified British Medical Research Council (p < 0.001) showed enhanced exercise tolerance. FEV1 improved, but the difference was not statistically significant.
Conclusions:
Small airway dysfunction is associated with bronchodilator responsiveness. Glycopyrronium bromide has proven to be capable of inducing favorable effects on lung hyperinflation and its functional and clinical consequences, with a decrease in dyspnea and an increase in exercise capacity. The use of anticholinergic drugs is useful in the management of small airway disease.
Introduction
Glycopyrronium bromide (GB) is an inhaled, long-acting muscarinic receptor antagonist (LAMA) with a quaternary ammonium structure and a low oral bioavailability, which reduces its systemic effects. It acts as a bronchodilator by blocking the muscarinic receptors M1 and M3. It does not cross the blood–brain barrier and therefore has few or no central effects. In clinical trials, patients who received GB as a symptom controller for moderate or severe chronic obstructive pulmonary disease (COPD)1,2 experienced a relevant amelioration in lung function, associated with an increased control of COPD symptoms, as well as with a lower need for rescue medication inhalers. An improvement in the quality of life was also reported. Quality of life represents an important aspect of COPD management.3,4 Published studies have shown that the damage caused by the inhalation of toxic particles, such as cigarette smoke and environmental pollutants, affects the “small airways.” Small airways—the quiet zone between the conducting and the respiratory lung zones—consist of respiratory bronchioles, which have a partially alveolated wall, and terminal bronchioles, that are devoid of cartilage and mucous-secreting glands. 5 The disease of the small airways is characterized by an inflammation of smallest bronchi and bronchioles, with inflammatory cellular infiltration, metaplasia of goblet cells and fibrosis, which leads to an increased thickness and tortuosity of the walls, as well as to an enhanced airway resistance, due to bronchial obstruction. This produces airflow limitation during expiration, resulting in lung hyperinflation and air trapping.6,7 We have studied a particular phenotype of patients, in whom the rate of bronchial caliber as forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio was in the normal range, but the forced expiratory flow in the middle half of the patient’s exhaled volume, forced mid-expiratory flow between 25% and 75% of FVC (FEF25–75) was reduced. FEF25–75 may be a more sensitive index for identifying obstruction at level of small airways. We recorded an increased value of residual volume (RV)/total lung capacity (TLC) ratio, as a marker of lung hyperinflation, and assessed the exercise tolerance by performing the six-minute walking test (6MWT) distance. The aim of this study was to determine whether there is a relationship between the changes in the small airways and the efficacy of the bronchodilation with GB.
Methods
This study included consecutive patients without acute manifestations of any disease and in a stable clinical state, whose dyspnea and exercise intolerance induced a referral to the Department of Respiratory Pathophysiology of “Mariano Santo” Hospital in Cosenza, Italy. Participants were evaluated by respiratory physicians from January 2018 to December 2018. All data were collected retrospectively. A detailed clinical history was taken, and a physical examination was performed. Lung function was measured through spirometry, carried out according to the American Thoracic Society/European Respiratory Society guidelines 8 ; exercise tolerance was assessed by performing the 6MWT. 9 Symptoms were also evaluated using the modified British Medical Research Council (mMRC) scale. 10 Patients were excluded if they had reported exacerbations in the previous 4 weeks, or in case of other lung diseases and uncontrolled comorbidities, such as severe cardiovascular diseases and malignant disorders.
Small airway obstruction is characterized by premature airway closure and air trapping, regional heterogeneity, and exaggerated volume dependence of airflow limitation. Therefore, tests that focus on these functional aspects can be useful surrogates in order to detect and quantify small airway disease. High levels of RV can be detected in the presence of premature airway closure and air trapping, TLC is commonly increased in obstructive disease, and the RV/TLC ratio is the best measure of RV increase, being also considered the first indicator of hyperinflation. FEF25–75 is the most cited functional measure of small airway obstruction. By excluding the initial peak of expiratory flow and averaging the flow rate over the mid-quartile range of FVC, FEF25–75 is very sensitive to the same small airway characteristics that result in the concavity of the expiratory flow-volume curve.
As a measure of airflow limitation, FEF25–75 is highly correlated with FEV1/FVC ratio, but non-linearly, so that FEF25–75 decreases more steeply than FEV1/FVC at mild obstruction levels. We considered a FEV1/FVC ratio <70% as a marker of obstruction, 11 a FEF25–75 <60% of predicted value as an expression of small airway dysfunction, 12 and an increase in RV/TLC ratio >20% as an indicator of lung hyperinflation. All subjects who exhibited a FEF25–75 reduction, a normal FEV1/FVC ratio, and an increased RV/TLC ratio with symptoms of dyspnea upon exertion, were treated with a bronchodilator therapy consisting of GB at the dosage of 50 μg once a day for 4 months. Patients did not receive other inhaled therapies during the study period. Clinical and functional parameters were collected at baseline and after 4 months of GB treatment. Because of the mild impairment of lung function detected in these patients, we decided to treat them only with an effective and safe LAMA, and our choice thus pointed to GB. Therefore, this therapeutic approach was part of an institutional protocol, aimed to avoid the use of albuterol or salbutamol on demand. Indeed, we think that the use of short-acting β2 agonists as rescue medications is not able to improve lung hyperinflation in such patients as those recruited in our retrospective study. All subjects released a written informed consent to the study, in accordance with the Helsinki Declaration.
Statistical analysis
The statistical analysis was performed using the SPSS program for Windows, version 9.0.0 (SPSS, Inc., Chicago, IL, USA). Data are shown as mean ± standard deviation (SD). Comparisons between data before and after treatment, within each group of patients, were done by paired Student’s t-test. The level of significance was set at p < 0.05.
Results
Overall, 115 patients were screened. Among these, 41 subjects met the inclusion criteria (23 females/18 males; mean age 66.82 ± 9.75 years), who had a normal FEV1/FVC ratio of 77.45% ± 4.86%, a reduced FEF25–75 of 42.9% ± 10.5%, with increased RV/TLC ratio of 132.68% ± 6.41%, FEV1 1.85 ± 0.54 L, FVC 2.39 ± 0.71 L. Their main demographic and clinical features are shown in Table 1. All patients had a diurnal respiratory function characterized by an obstruction of the small airways, associated with air trapping. Twenty-eight patients were smokers, while 13 subjects never smoked. A decreased exercise tolerance was shown by both baseline 6MWT (318.3 ± 36.6 m), and the information provided in the mMRC questionnaire (1.48 ± 0.77).
Demographics and clinical characteristics of patients.

SD, standard deviation; BMI, body mass index.
After treatment with GB, a significant improvement in lung function was noted as FVC (2.39 ± 0.71 L versus 2.70 ± 0.68 L, p = 0.04), FEF25–75 (42.9% ± 10.5% versus 52.9% ± 9.5%, p < 0.001), sR tot (168.18% ± 42.5% versus 132.01% ± 33.8%, p < 0.001), RV/TLC ratio (132.68% ± 6.41% versus 105.98% ± 6.73%, p < 0.001), with a reduction in dynamic hyperinflation (Table 2).
Functional and clinical features of patients at baseline and after treatment with GB.
SD, standard deviation; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 s; FEF25–75, forced mid-expiratory flow between 25% and 75% of FVC; PEF, peak of expiratory flow; sR tot, airway resistance; TLC, total lung capacity; RV, residual volume; 6MWT, six-minute walking test; mMRC, modified British Medical Research Council.
Patients showed an enhanced exercise tolerance, quantified as a significant increase in the distance covered during the 6MWT (318.3 ± 36.6 m versus 339.1 ± 31.8 m, p < 0.001) and a subjective reduction in the dyspneic symptoms reported in the mMRC questionnaire (1.48 ± 0.77 versus 0.53 ± 0.64, p < 0.001) (Table 2). FEV1 improved numerically but the difference was not statistically significant (1.85 ± 0.5 L versus 2.02 ± 0.5 L, p = 0.12) (Table 2).
Smokers showed a greater obstruction at the level of the small airways (31.1% ± 6.9% versus 55.2% ± 4.1%, p < 0.001) (Table 3).
Smokers/non-smokers and obstruction in the small airways.

SD, standard deviation; FEF25–75, forced mid-expiratory flow between 25% and 75% of FVC.
No side effects were recorded after the administration of GB.
Discussion
COPD is currently recognized as a complex clinical syndrome, rather than a specific disease entity, thus being considered as a broad term comprising a heterogeneous group of phenotypes that may have different treatment responses. In light of this understanding, the approach based on “one treatment to fit all” may not be appropriate, and there is a trend toward the individualization of the COPD therapy based on distinct phenotypes. More specifically, a key contributing factor to poor disease control might be the fact that such patients express a “small airway phenotype,” in the presence of an ongoing and unopposed small airway inflammation which is not being targeted nor controlled.13,14 Many patients who come to our observation with symptoms such as shortness of breath and recurrent cough display small airway parameter changes (decreased FEF25–75) and significant hyperinflation (increased RV/TLC ratio), with a FEV1/FVC ratio within the normal range as observed with spirometry testing. It can be useful to treat patients with this phenotype. This is the first study that highlights the efficacy of LAMA treatment in patients with FEV1/FVC ratio within the normal range, but with a significant obstruction of small airways. Generally, small airway dysfunctions are associated with bronchodilator responsiveness. Bronchodilation effectiveness can be demonstrated as a significant improvement in both FEV1 and FVC, when compared to the values measured before bronchodilator use.15,16 In our study, after LAMA treatment, we recorded an improvement in FVC. Lung hyperinflation is more closely associated with symptoms and exercise performance than spirometric assessments of reduced maximal expiratory flow rates. The progressive increase in resting hyperinflation as the disease advances has major implications for dyspnea and exercise limitation in COPD.17,18 It is well established that the widespread inflammatory damage to the peripheral airways, lung parenchyma and pulmonary vasculature can occur with only minor airflow obstruction. 19 Gas trapping, as assessed by expiratory CT scans, can exist in the absence of structural emphysema, and it is believed to indirectly reflect small airway dysfunction in mild COPD.20,21 Corbin et al., 22 in a 4-year longitudinal study on smokers with chronic bronchitis, reported a progressive increase in lung compliance leading to gas trapping, manifested by an increase in RV without significant changes in FEV1. 22 The net effect is that resting lung hyperinflation contributes to an increased elastic load on the inspiratory muscles, while simultaneously impairing their force-generating capacity.22,23 Small airway closure can lead to expiratory flow limitation through the increase in airways resistance, a consequence of the bronchial-bronchiolar caliber reduction due to structural remodeling and augmented vagal tone, together with the destruction of elastic pulmonary tissue. In these conditions, the RV increases, because the volume at which the balance between the elastic pressures of the lung and chest wall occurs is increased, leading to static lung hyperinflation.24,25 Thus, lung hyperinflation and the consequent changes in respiratory mechanics cause an increased respiratory work, that in turn leads to respiratory muscles fatigue, increased load, and respiration inefficiency. Dyspnea usually arises when the gas exchange is inefficient, as in ventilation/perfusion mismatching, exercise-induced hypoxemia, and impaired respiratory mechanics, where an uncoupling occurs between the increased ventilatory stimulus and the decreased mechanical performance.26,27 Bronchodilators, the cornerstone of COPD therapy, reduce the airway obstruction, leading to a decrease in the RV, and allow patients to exercise longer, thus positively impacting their quality of life. 28 The majority of the published studies aim to estimate the effectiveness of the drug through the improvement in FEV1, which correlates with little change in symptoms and exercise tolerance, being more linked to the reduction in lung inflation. In this study, we showed that GB can induce favorable effects on lung hyperinflation and its functional and clinical consequences, leading to a decrease in dyspnea and an increase in exercise capacity. In these patients, the most important effect was the increase in FVC, which sustained symptom improvement, even in the absence of FEV1/FVC ratio changes.29,30 FEV1 increase after bronchodilation is generally small, if any.
The most significant change after bronchodilation is the decrease in RV/TLC ratio, with a subsequent RV reduction, underlying a lowered lung hyperinflation, regardless of the basal FEV1 value. 27 Interestingly, the therapeutic efficacy of anticholinergic bronchodilation was primarily shown in our patients by the decrease in peripheral airway resistance. This appears to be a class effect due to LAMA utilization. In particular, we decided to use GB rather than the more referenced tiotropium bromide, because GB is characterized by a faster onset of action which provides a more rapid relief of dyspnea. Antimuscarinic bronchodilators, such as GB, have proven to be very useful in terms of lung deflation and exercise tolerance.30,31 Indeed, after treatment our patients experienced a better 6MWT performance. Evidence is growing in support of the concept that the airways dysfunction and inflammation in the small airway region of the lung may be contributing to distinct patient phenotypes. Besides the well-known concept that non-neuronal acetylcholine plays a relevant inflammatory role, the muscarinic receptor antagonism of non-neuronal acetylcholine released from airway epithelium is also important,32,33 thus potentially contributing to GB effects at level of small airways.34–36 Taken together, the results of the present study suggest that GB is capable of positively and significantly affecting lung hyperinflation, respiratory symptoms, and the psycho-physical status of patients with mild lung function impairment, likely allowing them to better use tidal volume and improve their ventilatory performance.37,38 Bronchodilation induced by GB is maintained throughout 24 h, after the administration of a single daily dose. This certainly represents a considerable advantage with regard to therapy adherence, because it is well known that the efficacy of a treatment also depends on patient’s compliance.29,31 An increased awareness of the importance of small airway dysfunction is an obvious first step, but the therapeutic challenge is to reverse the damage or at least to prevent disease progression. Earlier diagnosis could allow a more effective understanding of the role of small airways in triggering COPD pathogenesis, thereby driving a more rational approach to treatment, which may ultimately affect the prognosis of this disabling respiratory disorder. However, the small size of patient population, the lack of an appropriate calculation regarding sample size/power analysis, the absence of both a control arm and a randomization procedure, as well as the single-center nature of this study represent some relevant limitations.
Conclusions
In summary, based on the above-mentioned results, this study shows that GB can provide a beneficial effect on lung hyperinflation and its clinical and functional consequences. Anticholinergic bronchodilators such as GB can play an important role in the management of small airway dysfunction. There is currently a great interest in identifying clinical phenotypes of COPD that will ultimately guide toward a more personalized approach to disease management. This is a retrospective study which suggests, without definitely establishing, that LAMA may be potentially effective in patients with small airway impairment. Within this context, our limited clinical experience implies that further studies are needed to determine whether the patient with lung hyperinflation due to diseases of small airways will qualify as a distinct phenotype, possibly susceptible to specific therapeutic approaches.
Footnotes
Acknowledgements
The Authors thank Carmen Innes, an independent medical writer, who provided English language editing and journal styling on behalf of Springer Healthcare Communications. This editorial assistance was funded by Novartis Farma, Italy.
Author contributions
AP, CP, GP, MQ analyzed, interpreted the patient data regarding the respiratory physiopathology, and were a major contributor in writing the manuscript. LP, CC, LM were involved in data collection and statistical procedures. All authors read and approved the final manuscript.
Availability of data and material
All data generated or analyzed during this study are included in this published article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The study was approved by the local Ethical Committee of Calabria Region (N. 12/2018). All patients provided a written informed consent.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No specific funding was received for this research. The editorial assistance was funded by Novartis Farma, Italy.
Informed consent
Written informed consent was obtained from all subjects before the study.