
Abstract
Treatment of latent tuberculosis (TB) infection is an important component of TB control programs in both high- and low-prevalence countries. Clinical trials of treatment of latent TB conducted over several decades have demonstrated that preventive treatment can reduce the risk of developing active TB up to 90%. Although 9 months of daily, self-administered isoniazid has been the most widely used and recommended regimen for the treatment of latent infection, other regimens such as 3 months of daily isoniazid and rifampin, or 4 months of daily rifampin alone have also been recommended and used. Most recently, a 12-dose regimen of once-weekly isoniazid and rifapentine has been shown to be noninferior to 9 months of daily isoniazid in a large and well conducted clinical trial. Adoption of such a regimen on a large scale could have significant implications for TB elimination efforts.
Introduction
Over 2 billion people, nearly one-third of the world’s population, as estimated by the World Health Organization (WHO), have latent Mycobacterium tuberculosis infection; approximately 12 million of whom live in the United States [WHO, 2012; Bennett et al. 2007]. As the United States is among the countries with a low incidence of tuberculosis (TB), of particular concern is reactivation of latent infection, resulting in active disease. While reactivation usually occurs in approximately 5–10% of people with latent infection, certain hosts are more susceptible to this progression [American Thoracic Society, 2000]. Reactivated latent infection comprises the majority of cases found in the United States today (greater than 80%) [Bennett et al. 2007; American Thoracic Society, 2000; Geng et al. 2002]. Identification and treatment of individuals who are highly susceptible to reactivation of latent infection with antimicrobial therapy is imperative to reduce the burden of disease and is an important strategy in the attempt to eliminate TB [Sterling et al. 2003]. Similarly, a mathematical modeling exercise of various TB control interventions suggests that, around the world, treatment of latent infection will be necessary to control the global TB epidemic [Abu Raddad et al. 2009]. There are challenges to this task, however, as there is no direct diagnostic tool for latent infection and treatment requires long courses of antibiotic therapy with the potential for unfavorable side effects. As such, in recent years, there has been impetus for the development of novel screening mechanisms as well as shorter courses of therapy [Horsburgh and Rubin, 2011].
Screening
To date, there is no direct biological tool for diagnosis of latent infection with M. tuberculosis; detection methods rely primarily on identification of host cellular immune responses. For decades, the only commercially available screening test was the tuberculin skin test, an intradermal injection of purified tuberculin protein, which elicits a local delayed-type hypersensitivity reaction (mediated by cellular immunity) if a person has been exposed to M. tuberculosis. However, this test has somewhat limited sensitivity (about 70% based on the number of people with active TB who have positive tuberculin skin tests), and its ability to predict reactivation of latent infection is poor. In recent years, two new tests have become commercially available, interferon-γ release assays (or IGRAs), the QuantiFERON-TB Gold (Qiagen; Victoria, Australia) and the T-SPOT.TB test (Oxford Immunotec; Oxfordshire, UK). These tools also utilize the host immune response, but unlike the skin test, measure the production of interferon γ by peripheral lymphocytes when exposed to tuberculin antigens ex vivo. IGRAs are more likely to be positive in people who have recently been infected by M. tuberculosis, a group at high risk for reactivation, and have a higher specificity than the skin test (though perhaps modestly so) [Horsburgh and Rubin, 2011; Pai et al. 2008; Centers for Disease Control and Prevention, 2010]. Of note, both tests may be less sensitive when used in patients who are immunosuppressed [Aichelburg et al. 2009; Clark et al. 2007]. Vaccination with bacille Calmette-Guérin (BCG) can result in a positive delayed-type hypersensitivity response to skin testing, but the likelihood of interference with the test over time diminishes as immunity wanes, and should not affect the test after 10 or more years [Farhat et al. 2006].
While the tuberculin skin test is readily available, and IGRAs are becoming more widely accessible, a targeted screening approach is still recommended by the US Public Health Service. A broad screening approach could more readily eliminate TB in low-incidence countries such as the United States, but it is unclear if this would be cost effective. While the sensitivity of these novel screening tests is good (>90%), only 5–10% of those with positive tests will go on to develop active pulmonary disease [American Thoracic Society, 2000]. As such, given the generally low overall risk of reactivation despite a positive screening test, the false positive rate for disease could potentially be high. Given the challenges and risks associated with treatment, screening only those at high risk for reactivation of latent infection, who will benefit the most from treatment, is the most reasonable approach.
People at greatest risk for reactivation include those who have either been infected recently with M. tuberculosis or have clinical conditions associated with an increased risk of progression of latent to active disease. Recent infection includes those who have close contact with cases of active TB, those with screening tests that have converted from negative to positive within a 2-year span (for example, healthcare workers), and recent immigrants (less than 5 years) from countries with a high incidence of TB. In addition, homeless people, injection-drug users, and prisoners have been shown to have a higher prevalence of latent infection. A number of medical conditions are associated with an increased risk of reactivation of latent infection, notably states of immunosuppression. These include human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome, medical immunosuppression for treatment of a variety of diseases (notably with prednisone, tumor necrosis α inhibitors), radiographic evidence of old healed TB (untreated), poorly controlled diabetes, malnutrition, chronic renal failure, gastrectomy, ileojejunal bypass, solid organ transplant, head and neck malignancy, silicosis and tobacco smoking [American Thoracic Society, 2000; Horsburgh, 2004]. The majority of cases of active TB seen in the United States are from reactivation of latent infection in recent immigrants and close contacts of incident cases [Bennett et al. 2007; American Thoracic Society, 2000; Geng et al. 2002]. If any of these at-risk groups has a positive screening test for latent infection, treatment is generally recommended.
Treatment strategy and regimens
First, a clinical evaluation of active pulmonary TB must be performed, given risks associated with inappropriate treatment (e.g. monotherapy) of active disease. If active disease has been ruled out, the decision of whether or not to treat a patient for latent infection must take into account their individual likelihood of reactivation balanced against potential risks of therapy. The American Thoracic Society, the Centers for Disease Control and Prevention, and the Infectious Diseases Society of America have jointly recommended several treatment regimens (Table 1).
Available treatment regimens for latent tuberculosis infection.
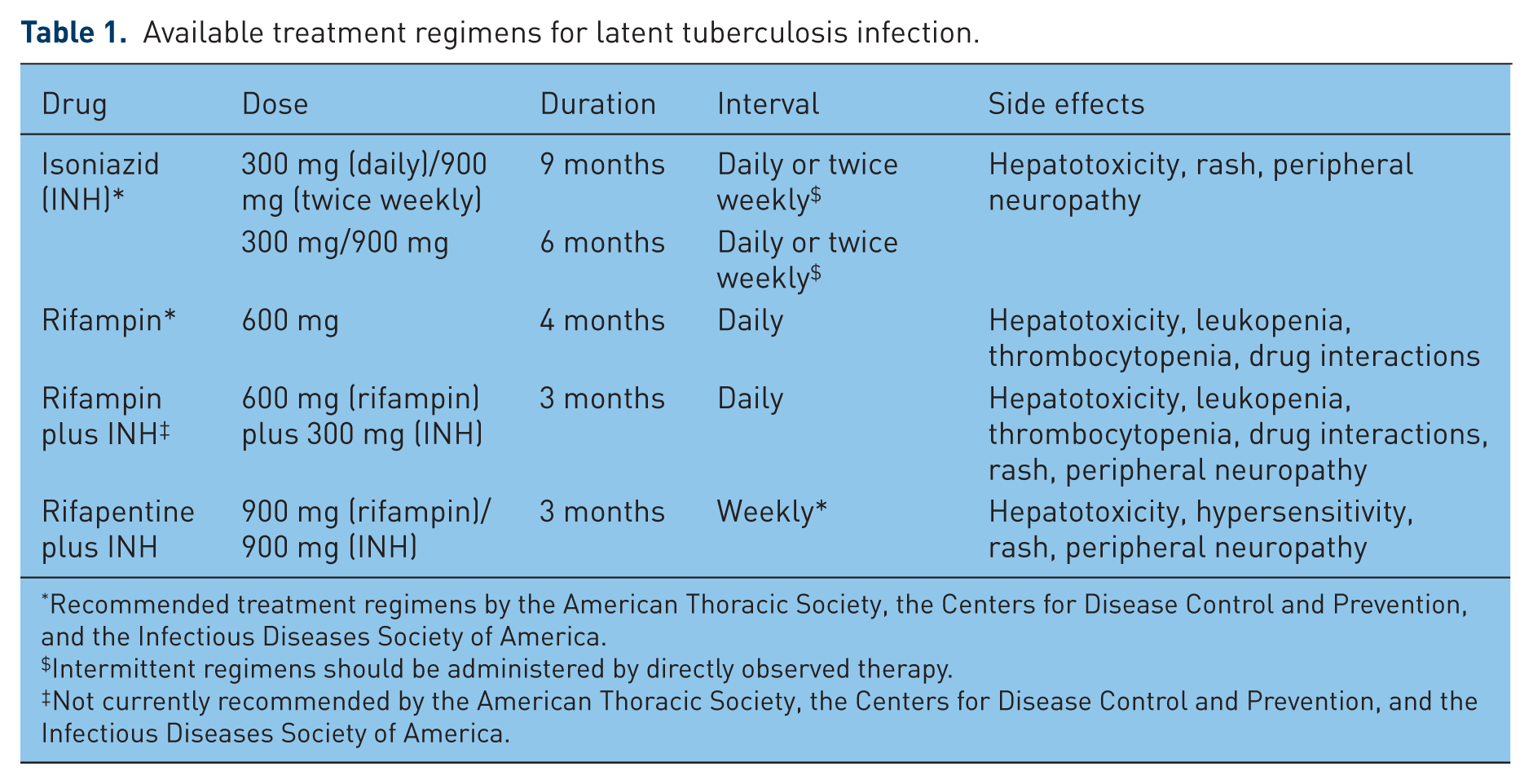
Recommended treatment regimens by the American Thoracic Society, the Centers for Disease Control and Prevention, and the Infectious Diseases Society of America.
Intermittent regimens should be administered by directly observed therapy.
Not currently recommended by the American Thoracic Society, the Centers for Disease Control and Prevention, and the Infectious Diseases Society of America.
Numerous randomized, placebo-controlled trials have examined the effectiveness of different regimens of isoniazid for treatment of latent infection of TB in the 1950s–1970s in multiple countries; these data suggest that daily or intermittent isoniazid is highly effective in preventing progression to active disease when taken as directed compared with placebo for a 12-month course (90%), and effective but less so if taken for a 6-month course (60–70%). These studies also revealed that in those who did not complete their full length of treatment (upwards of 30%) as prescribed, in part due to the prolonged course, there was less success at preventing reactivation. However, it was noted that protection was achieved even with irregular but sustained duration of treatment, suggesting intermittent (e.g. twice daily) dosing could be as successful as daily dosing [American Thoracic Society, 2000]. An International Union Against Tuberculosis study examined various lengths of isoniazid regimens (3, 6, 12 months), which found 12 months of therapy conferred better protection than 6 months, especially when compliance is good (93% versus 69% efficacy respectively) [International Union Against Tuberculosis Committee on Prophylaxis, 1982]. In patients who are HIV positive, trials have shown that isoniazid therapy for 6–12 months does reduce the risk of active TB in those with latent infection but with varied success (32–64%) [American Thoracic Society, 2000; Pape et al. 1993; Martinson et al. 2011; Grant et al. 2005]. Meta-analyses suggest the risk is significantly reduced with isoniazid therapy in patients with HIV and skin test positivity, though in high-prevalence countries, reinfection is always a possibility and can limit the effectiveness of short courses of preventive therapy [Bucher et al. 1999; Akolo et al. 2010]. Modeling of the data from these studies suggests that a course between treatment periods of 6 and 12 months (e.g. 9 months) would optimize protection and would have better compliance than a 12-month regimen [Comstock, 1993]. These data suggest for isoniazid monotherapy for treatment of latent infection, a 9-month regimen is favored over 6 months, either by daily or twice weekly administration; if intermittent dosing is preferred, directly observed therapy (DOT) should be used [American Thoracic Society, 2000].
Hepatotoxicity remains a significant concern in those receiving isoniazid therapy. In 1970–1971, the US Public Health Service monitored 14,000 people receiving isoniazid for development of hepatotoxicity. While the rate of hepatitis was found to be between 1% and 2.3%, a number of fatal cases during that surveillance period prompted awareness of this potentially serious adverse effect [Kopanoff et al. 1979]. This risk of hepatitis is increased in those with chronic liver disease and with alcohol consumption. More recent data suggest a greater (3.8%) risk of serious hepatotoxicity during a 9-month course of isoniazid [Menzies et al. 2008]. Peripheral neuropathy has also been noted in patients receiving isoniazid due to alteration in pyridoxine metabolism, though is rare at doses prescribed for treatment of latent disease, and can be prevented with pyridoxine supplementation [American Thoracic Society, 2000].
Despite the success rates of isoniazid, given the risk of hepatotoxicity and long course of treatment, shorter (3–4 months) rifampin and rifapentine containing regimens have also been evaluated. Administration of a 4-month course of rifampin only, for which there is very little efficacy evidence to date from clinical trials, has been recommended as an alternative regimen for those unable to receive 9 months of isoniazid, largely due to efficacy demonstrated in animal studies [American Thoracic Society, 2000]. In one study examining treatment of latent infection in patients with silicosis in Hong Kong, a 3-month course of rifampin was found to have similar efficacy to the 9-month regimen of isoniazid [Hong Kong Chest Service/Tuberculosis Research Centre, 1992]. Data do suggest cost effectiveness and reduction in hepatotoxicity for 4 months of rifampin compared with 9 months of isoniazid [Menzies et al. 2004]. Two trials comparing the efficacy of a 4-month course of rifampin and 9 months of isoniazid for the treatment of latent infection are currently ongoing [ClinicalTrials.gov identifiers: NCT00931736, NCT01398618]. A 3-month regimen of isoniazid and rifampin is an alternative regimen that has also been suggested, though it is not currently recommended in the United States. Limited clinical trial data exist; a meta-analysis of four small studies and a study conducted in people with HIV have shown the efficacy of this regimen [Martinson et al. 2011; Ena and Valls, 2005; Whalen et al. 1997]. A 2-month regimen of rifampin and pyrazinamide had promise from studies performed in the 1990s [Halsey et al. 1998; Gordin et al. 2000] but thereafter was shown to have high rates of severe hepatotoxicity [Jasmer et al. 2002] and is no longer recommended. Rifampin is known to cause hepatotoxicity, though less so than isoniazid [Menzies et al. 2008], and has also been shown to have various drug interactions, limiting widespread use, notably oral contraceptives, protease inhibitors and non-nucleoside reverse transcriptase inhibitors [Horsburgh and Rubin, 2011]. In addition, though less commonly, rifampin can cause leukopenia, thrombocytopenia and rash [American Thoracic Society, 2000].
The most recent and perhaps most promising short-course regimen studied is 3 months of rifapentine and isoniazid, administered weekly. Rifapentine is a rifamycin derivative, has a longer half life and is more potent against M. tuberculosis than rifampin in animal models. PREVENT-TB was a large, international, open-label, randomized noninferiority trial that compared 3 months of rifapentine and isoniazid (with DOT) with the standard self-administered 9-month isoniazid therapy between 2001 and 2008. With nearly 8000 participants, the short-course combination regimen was found to be noninferior to 9 months of isoniazid therapy. In addition, this study revealed a higher completion rate, as well as a lower rate of drug-related hepatotoxicity (0.4% in the combination group versus 2.7% in the isoniazid group) [Sterling et al. 2011]. Still in question is how large a role DOT played in the results obtained in the combination arm of the study; as such, there is an ongoing trial examining the effectiveness of this regimen by DOT compared with self-administered therapy [ClinicalTrials.gov identifier: NCT01582711]. Another recent study examined the effectiveness of various regimens (3 months rifapentine/isoniazid, 3 months rifampin/isoniazid, 6 months isoniazid, continuous isoniazid) for treatment of latent infection in patients with HIV in South Africa. This study revealed similar effectiveness of all regimens [Martinson et al. 2011]. Of note are minimal drug–drug interactions due to rifapentine compared with rifampin, making the 3-month rifapentine/isoniazid combination therapy even more appealing [Horsburgh and Rubin, 2011; Sterling et al. 2011].
Compliance and safety monitoring
Imperative to success of treatment for latent infection is adherence to therapy. As completion rates have been relatively low for decades, this poses a major challenge to large-scale TB control. Generally, the length of treatment course has been the major determinant for completion, with 6 months and 9 months of isoniazid having the poorest completion rates (44–69%), and 4 months of rifampin with completion rates reported between 60% and 91% [American Thoracic Society, 2000; Menzies et al. 2004; Hirsch-Moverman et al. 2010; Li et al. 2010; Horsburgh et al. 2010]. Three months of rifapentine and isoniazid also had higher completion rates than 9 months of isoniazid (82% and 60%, respectively), but this may be confounded by directly observed administration of the combination regimen. While prior attempts at reducing length of treatment have previously been modest, this short 3-month regimen does offer significant potential for improved adherence to therapy [Sterling et al. 2011]. Other factors associated with reduced completion rates include younger age, employment in a healthcare facility, homelessness, and substance abuse, all of which are important targets for strategic TB control [Hirsch-Moverman et al. 2010; Li et al. 2010; Horsburgh et al. 2010].
Hepatotoxicity remains the adverse effect of greatest concern with all potential treatment courses and is greater in isoniazid-containing regimens. While prospective data are lacking for optimal safety monitoring, it is generally recommended that serum liver-enzyme screening should be performed in all patients with underlying liver disease, HIV infection, women who are pregnant or postpartum, and patients who consume considerable amounts of alcohol prior to treatment. Monthly follow-up levels should be performed in those with abnormal baseline values. Clinical monitoring is recommended for all patients for signs and symptoms of hepatotoxicity and other reactions; if a patient has symptoms suggestive of hepatitis, and aminotransferase levels greater than or equal to three times the upper limit of normal, or asymptomatic patients have levels greater than or equal to five times the upper limit of normal, therapy should be discontinued. Coadministration of pyridoxine is recommended for patients receiving isoniazid at increased risk for development of peripheral neuropathy, notably diabetes, renal failure, alcoholism, malnutrition and HIV infection, but given its ease and tolerability, it may be given to any or all patients being treated with isoniazid [American Thoracic Society, 2000; Horsburgh and Rubin, 2011].
Recommendations
Targeted screening and treatment of latent infection with M. tuberculosis is an important public health strategy to curb a reservoir of TB, especially in the United States, where reactivation of latent infection accounts for most cases of active disease. Screening should be performed among those with greatest risk for development of active disease, namely those with recent infection, and those at increased risk for reactivation. While tuberculin skin testing was previously the mainstay of screening tools, in more recent years, IGRAs have emerged as novel tests, and may provide more specificity for reactivation of latent infection in very high-risk groups. Once latent TB has been diagnosed in high-risk people, active TB must first be ruled out clinically and radiographically prior to therapy initiation. US guidelines recommend either a 6- or 9-month course of isoniazid (9 months preferred), or 4 months of rifampin, with efficacy studies for 4 months of rifampin currently underway. Recently added to these options is a 3-month course of weekly rifapentine and isoniazid, which may provide the best balance of length of course (and therefore likelihood of completion) and side-effect profile, and has the potential to be the mainstay of therapy for latent infection [Centers for Disease Control and Prevention, 2011]. Monitoring of safety, development of active pulmonary TB, and adherence are imperative for any regimen chosen. Looking ahead, investigation is needed to determine the efficacy of new antimicrobial agents in the treatment of latent infection, namely for those with known exposure to drug-resistant TB.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.